
Abstract
Background:
The tall cell variant of papillary thyroid carcinoma is an aggressive subtype that generally presents as a large tumor in the advanced stage; however, little is known about the tall cell variant of microcarcinoma (tumors measuring <1 cm). In this study, we compare the tall cell variant of microcarcinoma (microTCV) with classic papillary microcarcinomas to examine the hypothesis that, despite the small size, the microTCV may be more aggressive than the classic papillary microcarcinoma.
Methods:
We identified 27 microTCV patients and compared their clinicopathologic features and BRAF V600E mutational status with classic papillary microcarcinomas matched by age and size. The patients with microTCV included 22 women and 5 men aged 33 to 74 years (median age, 56 years). All patients underwent total thyroidectomy; 20 patients had lymph node dissection.
Results:
Tumor size in microTCV patients ranged from 2 mm to 10 mm (median, 7 mm). Extrathyroidal extension and lymphovascular invasion were seen in 9 (33%) and 4 (15%) tumors, respectively. Thirteen patients (48%) harbored multifocal papillary carcinomas. Metastasis to central compartment lymph nodes was seen in 8 patients and to lateral cervical nodes in 3 patients. Nine of the 25 patients (36%) presented at an advanced stage (stage III/IVA). The BRAF V600E mutation was detected in 25 of 27 tumors (92.6%). In contrast, age- and size-matched classic papillary microcarcinomas (n=26) showed no extrathyroidal extension (p=0.002), lymphovascular invasion in 1, central compartment lymph node metastasis in 2, lateral cervical node metastasis in 1, multifocal tumors in 10 (38.5%), the BRAF V600E mutation in 20 (76.9%), and it infrequently presented in stage III/IVA (7.7%, p=0.02).
Conclusions:
The microTCV form is associated with aggressive features at presentation, and it should be differentiated from other papillary thyroid microcarcinomas.
Introduction
P
The BRAF V600E mutation has emerged as the most common genetic alteration in sporadic papillary thyroid carcinomas in adults. The BRAF V600E oncogene is a strong activator of the mitogen-activated protein kinase (MAPK) signaling pathway, which leads to uncontrolled cell proliferation and transformation into malignancy (6,7). Approximately one third of microcarcinomas may harbor the BRAF V600E mutation (5). This mutation is reportedly associated with a poor prognosis and a higher risk of recurrence, even in microcarcinomas (5). Recognition of poorly behaving microcarcinomas may help triage patients for additional therapy and closer surveillance.
The tall cell variant of papillary thyroid microcarcinoma (TCV) is a clinically aggressive form of thyroid carcinoma. Originally described in 1976 by Hawk and Hazard, these tumors are defined as being comprised of elongated tumor cells, the height of which is at least twice their width (8). The tumor cells have moderate to abundant homogeneous eosinophilic cytoplasm with exaggerated nuclear features of papillary carcinoma and frequent, often multiple intranuclear inclusions (9). In a recent analysis of 573 TCVs, the patients were significantly older, had larger tumors, higher rates of extrathyroidal extension, lymph node and distant metastases at presentation, and increased disease-related mortality than classic papillary carcinomas (10). Another matched-pair analysis of TCV and classic papillary carcinoma concluded that the tall cell histology was a significant prognostic factor for disease-specific mortality, and that the aggressive biological behavior was independent of age, gender, and tumor size (11). The tall cell variants are also overrepresented in papillary carcinomas refractory to radioactive iodine therapy (12). The prevalence of the BRAF V600E mutation is reported to be as high as 80–100% in tall cell variants (7,13).
The microTCV is a relatively undefined entity of unknown significance, as subtyping of microcarcinoma is usually not attempted in general surgical pathology practice. To the best of our knowledge, there are no large studies of microTCV, despite anecdotal reports of aggressive behavior (14). In this study, we compare the clinicopathologic features and BRAF V600E mutational status of microTCV with age- and size-matched classic papillary microcarcinomas to examine the hypothesis that, despite the small size, microTCV may be more aggressive than the classic papillary microcarcinoma.
Materials and Methods
Approval from the institutional review board was obtained before commencing this retrospective study. The surgical pathology database of the Yale–New Haven Hospital was queried for thyroid malignancies, specifically papillary microcarcinomas. Hematoxylin- and eosin-stained glass slides from all microcarcinomas were reviewed by two pathologists, and 27 microTCVs were identified. The criteria for microTCV diagnosis were as follows: tumors comprised of >30% of tall cells whose heights were at least twice their width (15). The following histologic features were evaluated: location of tumor within the thyroid (subcapsular/capsular or intraparenchymal), tumor capsule, tumor-associated stromal reaction (fibrosis and/or desmoplasia) and lymphocytic infiltrate, extrathyroidal extension, tumor interface with non-neoplastic thyroid, psammoma bodies, cystic change, lymphovascular invasion, and any additional pathology in the non-neoplastic thyroid parenchyma. Fine-needle aspiration (FNA) cytology of the microTCV was reviewed if available. Clinical information, including patient demographics, therapy, and follow-up information, was obtained from medical records.
BRAFV600E mutational analysis
The mutational analysis was performed on formalin-fixed paraffin-embedded tumor tissues from the thyroid resections in 24 patients with microTCV. The tumors were identified and marked on the hematoxylin- and eosin-stained glass slides by an experienced endocrine pathologist. Five to 10 unstained sections (2–5 μm thick) from the tumor were deparaffinized and macrodissected. DNA was extracted using a Qiagen tissue kit according to the manufacturer's protocol (Qiagen, Chatsworth, CA). Five to 20 ng of extracted DNA was amplified using 0.2 μM polymerase chain reaction (PCR) primers flanking the region of the 1799T>A mutation in the BRAF gene that results in the V600E substitution (5′ primer: CTC TTC ATA ATG CTT GCT CTG ATA GG and 3′ primer: TAG TAA CTC AGC AGC ATC TCA GG) in a 50 μL PCR reaction solution containing 1× PCR buffer, 0.1 mM deoxyribonucleotide triphosphate, 1.5 mM MgCl2, and 2.5 units of AmpliTaq Gold DNA polymerase. PCR started with initial denaturation at 95°C for 8 minutes, followed by 35 cycles of denaturation at 94°C for 1 minute, annealing at 55°C for 1 minute, and synthesis at 72°C for 2 minutes, and it was finished by a final extension at 72°C for 10 minutes (ABI Veriti Thermal Cycler, Applied Biosystem, Foster City, CA). The 250 base pair–amplification product was analyzed by single-strand conformational polymorphism (SSCP) using 4 μL of the PCR product on a mutation detection enhancement nondenaturing gel. Electrophoresis was carried out on ice for 2 hours and 45 minutes at 325 volts. The SSCP gel was then stained with SYBR Gold (Molecular Probes, Carlsbad, CA) 1:10,000 in tris-EDTA added for 20 minutes and imaged by BioRad GelDoc UV System (BioRad, Hercules, CA). The presence of the BRAF V600E mutation was determined by comparing the SSCP banding pattern of the case with positive (colonic adenocarcinoma and papillary thyroid carcinoma) and negative (normal tonsil, benign thyroid nodule) controls (Fig. 1). In the remaining patients (n=3) the mutational analysis was performed with DNA obtained from FNA of the tumors, as described previously (16). After making direct smears for cytologic evaluation, the needle was rinsed in Cytorich Red solution (Thermo-Fisher Scientific Inc., Kalamazoo, MI) for ThinPrep (Hologic Inc., Boxborough, MA), and the solution was subjected to BRAF V600E mutational analysis.
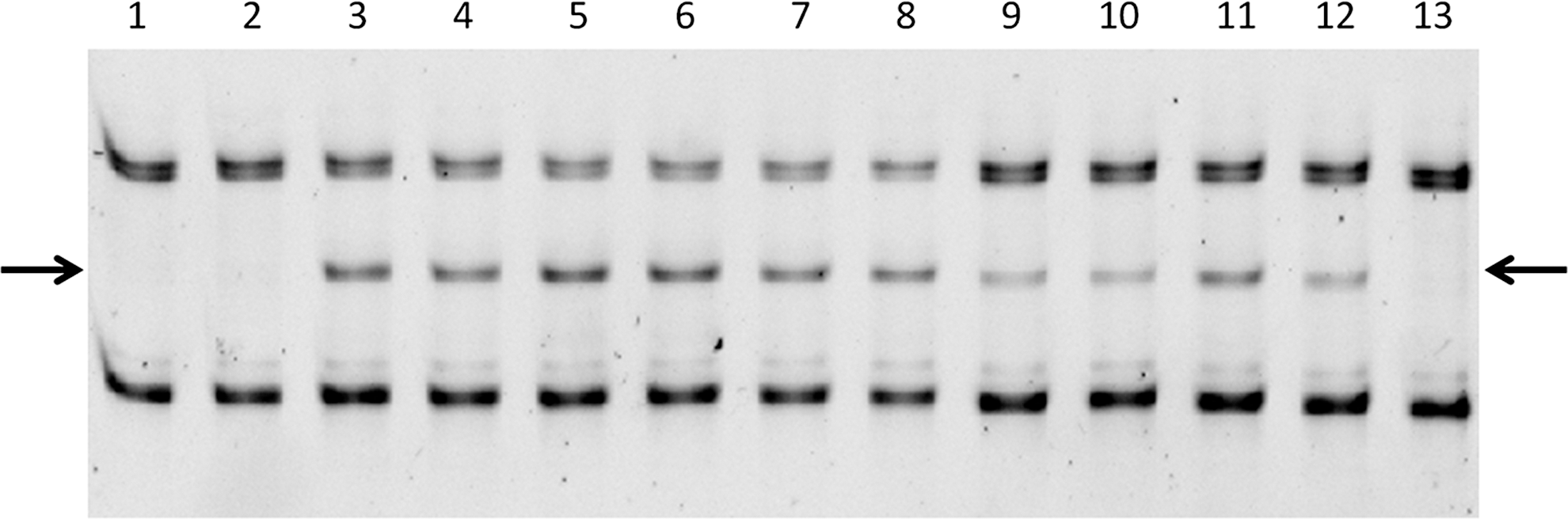
Detection of the 1799T>A mutation encoding the V600E substitution in the BRAF gene (BRAF V600E) by single strand conformational polymorphism. Lanes 1–10, test samples in duplicate; lanes 11 and 12, BRAF V600E mutation-positive papillary thyroid carcinoma control showing an abnormal band in the middle (arrows); lane 13, negative control (tonsil). Lanes 1 and 2, benign thyroid nodule with wild-type BRAF; lanes 3 and 4, mutation-positive classic papillary thyroid carcinoma; lanes 5 and 6, tall cell microcarcinoma (case 19); lanes 7 and 8, mutation-positive colonic adenocarcinoma; lanes 9 and 10, another mutation-positive classic papillary thyroid carcinoma. The analytical sensitivity of the test is indicated by the mutation-positive controls in lane 12 at 5% dilution.
Data analysis
Age- and size-matched consecutive classic papillary microcarcinomas were selected for comparison from a previous study set (17). The association between categorical variables was evaluated using the two-tailed Fisher exact test with α set at <0.05 (GraphPad InStat 3.1, GraphPad, San Diego, CA).
Results
Table 1 shows age, sex, location, size, and follow-up information on patients with microTCV (n=27). Eighteen tumors were in the left lobe, and 9 were found in the right lobe. The tumors ranged in size from 2 to 10 mm (median, 7 mm). The patients were aged 33 to 74 years (median, 56 years) and presented with thyroid nodules that were evaluated by ultrasound (US). US-guided FNA cytology of the thyroid nodules was available in 26 patients, and 21 of these targeted the microTCV. The criteria for selectively sampling subcentimeter thyroid nodules by US-guided FNA cytology were as follows: hypoechoic nodules with infiltrative margins, length greater than width, presence of microcalcifications, and increased vascularity. All 21 microTCV samples yielded adequate cellularity and were interpreted as positive (n=19) or suspicious (n=2) for malignant cells (21/21, 100% positive). In 5 patients, a nodule other than the microcarcinoma was sampled, which lead to cytology diagnoses of benign (n=2), Hürthle cell neoplasm (n=1), and indeterminate (atypia of unknown significance [AUS], n=2).
Incidental tall cell microcarcinoma.
C, capsular; ETE, extrathyroidal extension; F, female; IP, intraparenchymal; M, male; NA, not available; neck+, positive lymph nodes, neck–, negative lymph nodes; NED, no evidence of disease; RAI, radioactive iodine therapy (+received, – not received); SC, subcapsular.
All 27 patients underwent total thyroidectomy. Six patients had incidental (22%) microTCV (size 2 to 7 mm) associated with multinodular goiter (cases 22, 23, 26) and Hashimoto/chronic lymphocytic thyroiditis (cases 21, 24, 25). Twenty patients underwent central neck dissection and 3 patients (cases 15, 18, 25) had a lateral neck dissection after confirmation of cervical node metastasis by US-guided FNA.
Gross examination of the microTCV samples showed a grey-tan, firm, solid-cut surface with infiltrative borders and without encapsulation (Fig. 2). Sixteen tumors (59%) were capsular/subcapsular, and 11 were intraparenchymal in location. At microscopy, the tumor cells were at least 2–3 times as tall as wide and exhibited moderate to abundant homogeneous eosinophilic cytoplasm with enlarged nuclei showing chromatin clearing, exaggerated intranuclear inclusions, irregular nuclear membrane, and grooves. Trabeculated architecture with back-to-back papillae with slit-like spaces were seen in all tumors, whereas psammoma bodies were noted in 2 tumors only (Fig. 3). All but one of the tumors exhibited an infiltrative interface with non-neoplastic thyroid. Microscopic extension into the perithyroidal fat was seen in 9 tumors (Fig. 4). Tumor-associated stromal reaction included fibrosis (n=26), desmoplasia (n=11), and lymphocytic response (n=24). Sixteen of the 27 thyroids exhibited chronic lymphocytic thyroiditis/Hashimoto thyroiditis (59%), and 13 (48%) thyroids contained multifocal papillary carcinoma with an average of 2 in each, including 2 thyroids with 2 microTCVs in each (cases 14 and 19).

Case 4: A 6-mm subcapsular tumor in a 51-year-old woman. The tumor shows a grey-tan, firm, solid-cut surface with infiltrative borders and without encapsulation.
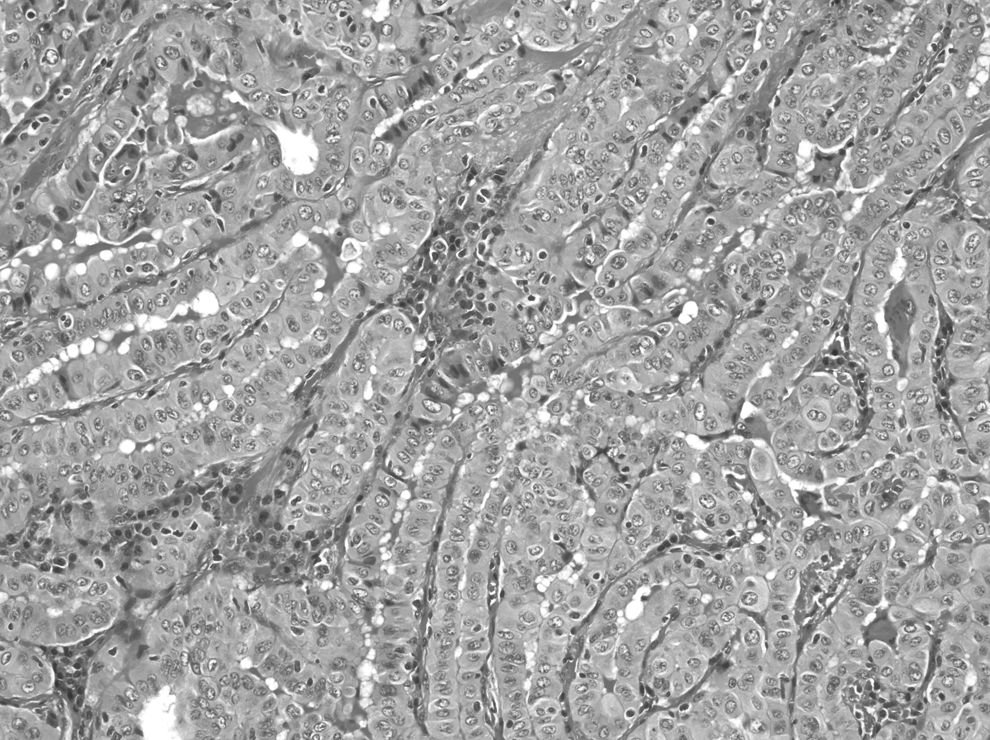
Case 14: Tall cell microcarcinoma (size, 9 mm) in a 34-year-old woman. The tumor shows tumor cells with moderate to abundant homogeneous eosinophilic cytoplasm, enlarged nuclei with chromatin clearing, exaggerated intranuclear inclusions, and irregular nuclear membrane and grooves. The tumor cells are 2 to 3 times as tall as wide. The architecture is trabeculated with back-to-back papillae and slit-like spaces with little colloid (H&E, ×200).
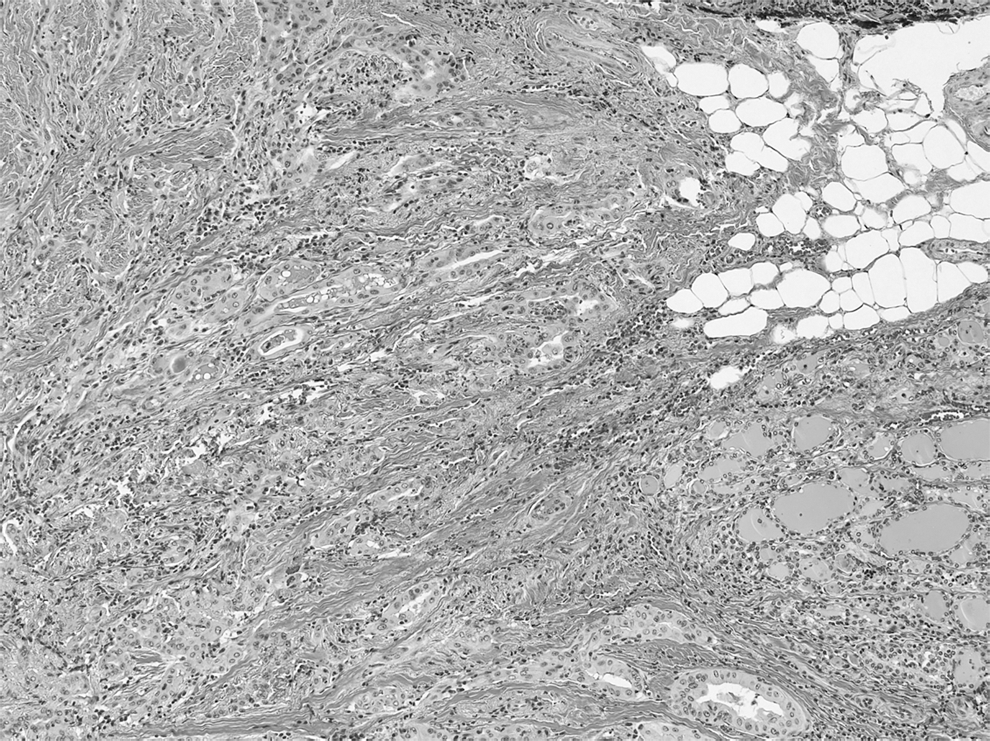
Case 3: The tumor has an infiltrative interface with non-neoplastic thyroid (left side). Microscopic extrathyroidal extension is seen in the perithyroidal fat (H&E, ×100).
Table 2 compares the microTCV to age- and size-matched classic papillary microcarcinomas. Differences between tall cell and classic papillary microcarcinoma included a slight male preponderance, a predilection for extrathyroidal extension (p=0.002), lymphovascular invasion, multifocality, central and lateral neck metastasis, a higher stage at presentation (p=0.02), and a higher incidence of the BRAF V600E mutation in the former, when compared to the latter (Table 2).
Two patients (cases 10 and 16) were excluded from staging as the T, N, and the AJCC stage was determined by synchronous, larger (2.4 cm and 1.3 cm, respectively) follicular variant of papillary carcinomas.
AJCC, American Joint Committee on Cancer; T1a, tumor ≤1 cm, limited to thyroid; T3, any size tumor with minimal extrathyroidal extension; N0, no regional lymph node metastasis; N1a, metastasis to level VI (central neck) lymph node; N1b, metastasis to cervical (levels I–V) lymph nodes (lateral neck dissection was performed after confirmation of the positive lymph nodes by US-guided FNA biopsy).
Follow-up information was available from 1 month to 9 years (mean, 20 months) in the patients with microTCV. Nine of 13 patients where information was available were treated with postoperative radioactive iodine (RAI) therapy. All patients were alive and free of disease as of last follow-up, including 6 patients with more than 2 years of follow-up (Table 1).
Discussion
The tall cell variant of papillary carcinoma typically affect older patients and are larger and higher stage at presentation compared to classic papillary carcinoma (15,18). Terry et al. showed that the tall cell morphology, as well as age and tumor size, were a significant predictor of recurrence (19). Our study shows that despite controlling for age and size, microTCV were still associated with higher stage and aggressive features at presentation. Extrathyroidal extension was seen exclusively in microTCV, and the BRAF V600E mutation was detected in 93% of all microTCV. We found that 39% of the microTCV metastasized to the central compartment lymph nodes compared to 13% of size-matched classic papillary microcarcinoma, a three-fold increase in the former. Metastasis to lateral cervical lymph nodes is unusual in microcarcinomas and suggests aggressive behavior; this was also three times more frequent in microTCV compared to classic papillary microcarcinoma.
MicroTCV is underrecognized for many reasons: the World Health Organization Classification of Tumors (2004) does not subtype thyroid microcarcinoma with regards to histologic variants; the criteria for subtyping microcarcinoma are not well defined and their small size renders subtyping difficult. Thyroid microcarcinomas are usually incidental findings with excellent prognosis and the significance of subtyping microcarcinomas is unknown. Thus microcarcinomas are not histologically subtyped in routine practice. The introduction of synoptic reports for thyroid cancers in our practice in 2009 prompted the pathologists to evaluate microcarcinomas similar to larger tumors in order to complete the data element “histologic subtype.” This increased scrutiny helped in identifying microTCV among all thyroid microcarcinomas. Despite this, only 14 tumors (52%) in the current series were diagnosed as microTCV at initial pathologic examination, and the remaining tumors were identified upon review. Our experience further highlights the underreporting of microTCV.
In the original description of tall cell variant of papillay carcinoma, Hawk and Hazard defined these tumors as being comprised of cells that were twice as tall as wide (8). However, there is controversy regarding the proportion of tall cells required to meet the definition of tall cell carcinoma. According to one expert, classic papillary carcinoma may contain 5% to 10% tall cells (9). Various investigators have used a >10%, >30%, >50%, or >75% tall cell component to define the tall cell variant of papillary thyroid carcinoma (15,18 –23). Irrespective of the proportion of tall cells, all investigators reached the conclusion that the tall cell variant is an aggressive variant of papillary thyroid carcinoma. Little is known about microTCV. In our opinion, >30% tall cells in a microcarcinoma that is only a few millimeters in size is significant, and the proportion of tall cells may additionally be altered by FNA preceding surgical resection.
Interestingly, all 21 microTCV that were evaluated by US-guided FNA cytology were positive or suspicious for malignancy, leading to total thyroidectomy with lymph node dissection in 20 cases. The majority of microTCV was superficial with a capsular/subcapsular disposition and had infiltrative borders—features that were detected with ultrasonography. Choi et al. published the sonographic characteristics of tall cell variant of papillay carcinoma: taller than wide, irregular, solid, markedly hypoechoic, and multilobulated tumors that are often associated with microcalcifications, extrathyroidal extension, and lymph node metastasis (24). Solomon et al. reported that elongated tumor cells, oncocytic cytoplasm, distinct cell borders, and “soap bubble”–like intranuclear inclusions were readily evident in tall cell carcinoma and concluded that they can be reliably diagnosed by FNA cytology (25). Our data suggests that despite their subcentimeter size, microTCV are also highly amenable to preoperative diagnosis by ultrasonography and by FNA cytology. This may be helpful in planning the appropriate management strategy.
We observed several similarities between microTCV and larger tall cell carcinoma. We noted an incidence of 9% tall cell variants in our database of papillary microcarcinomas similar to larger tumors (14,17 –19,22). Other similarities included older age (>50 years), slight male predilection, higher prevalence of the BRAF V600E mutation (>90%), and extrathyroidal extension (8,11–12,18). The BRAF V600E mutation plays a role in extracellular matrix remodeling and is associated with an increase in matrix metalloproteinases, desmoplastic stromal reaction, and invasiveness (26). In a previous study, we found a significant association between the presence of the BRAF V600E mutation and infiltrating tumor borders, fibrosis, and desmoplastic stromal reaction (27). In this series, more than 93% of the microTCV harbored the BRAF V600E mutation and showed tumor-associated stromal fibrosis and infiltrating tumor borders.
The current study is limited by its retrospective nature and lack of long-term follow-up. Several of the features (e.g., male sex, lymphovascular invasion, metastasis to central and lateral neck lymph nodes, and BRAF V600E mutation) were more frequently associated with the microTCV compared to the classic papillary microcarcinoma, but they failed to reach significance. We excluded microcarcinoma that were not classic papillary types (e.g., the follicular variant of papillary carcinoma, which has an exceedingly low prevalence of BRAF V600E mutation and is usually not considered in the differential diagnosis of tall cell carcinoma). It is possible that several of the clinicopathologic differences between the two groups may have reached significance if we had included all types of papillary microcarcinomas without age and size matching; however, this needs to be evaluated with a larger number of cases. Although we did not observe any recurrence or distant metastasis in our cases, including those followed for 2 years or longer, a recently published series of 47 tall cell carcinomas describes one microcarcinoma that metastasized to the lung (14). This highlights the need for long-term follow-up of all microTCV in order to understand their biological significance.
In summary, we report the largest series of the tall cell variant of papillay thyroid microcarcinoma and demonstrate for the first time that despite the small size, these microcarcinomas are significantly associated with extrathyroidal extension and higher stage at presentation, and they are associated with a higher predilection for male sex, multifocality, lymphovascular invasion, lymph node metastasis, and the BRAF V600E mutation compared to classic papillary microcarcinoma. The microTCV are phenotypically and genotypically similar to larger tall cell carcinomas. This suggests that the molecular events driving the tall cell phenotype may be early and de novo. Recognition of the microTCV on histopathology and long-term follow-up of a large number of cases may help in better understanding its biological behavior.
Footnotes
Acknowledgments
The authors thank Dr. R. Ghossein for reviewing several of the tumors in the current series. This study was supported by funding from the Department of Pathology, Yale School of Medicine, New Haven, Connecticut.
Disclosure Statement
The authors declare that no competing financial interests exist.