
Abstract
Background:
The McGill Thyroid Nodule Score (MTNS) is a scoring system devised to help physicians to assess the preoperative risk that a thyroid nodule is malignant. It uses 22 different known risk factors for thyroid cancer (radiation exposure, microcalcifications on ultrasound, positive HBME-1 stain on biopsy, etc.) and attributes a percentage risk that the nodule is malignant. Recently, preoperative thyroglobulin (Tg) levels have been shown to correlate with the risk of malignancy. The aim of this study was to incorporate Tg levels into the already established MTNS.
Methods:
This is a retrospective analysis of 184 thyroidectomy patients at the McGill University Thyroid Cancer Center. Patients with preoperative Tg levels were included in the study, and patients with incidental papillary microcarcinoma without extrathyroidal extent on final pathology were excluded. MTNS scores were calculated for all patients. Preoperative Tg levels of 75 ng/mL added one point to the MTNS, and levels of 187.5 ng/mL added two points. The new system is named MTNS+.
Results:
Malignancy rates were calculated for each MTNS+ score. Patients with a score of 0–1 were <5% at risk of malignancy. The malignancy rate for scores of 2–3 was 14.29%, followed by 28.95% for scores of 4–6, 32.65% for scores of 7–8, 64.86% for scores of 9–11, 71.43% for scores of 12–14, 78.57% for scores of 15–18, and 92.31% for scores of 19–22. All patients (five of five) with an MTNS+ score of 23 or more had a malignant final pathology result. Patients with scores greater than eight had a relative risk of 2.5 [CI 1.79–3.49] of malignancy compared to patients with lower scores. MTNS+ showed good specificity at higher scores, with 89%, 96%, and 100% at scores above 11, 14, and 20 respectively. Compared to MTNS, adding Tg levels did not improve positive predictive values (PPV) or specificity, but improved sensitivity by 7.89% for scores greater than eight, and by up to 10.48% for scores greater than seven.
Conclusion:
This study shows that adding Tg to the MTNS increases the sensitivity of this scoring system. Moreover, it suggests that a combined scoring system such as the MTNS+ can accurately stratify the risk of well-differentiated malignancy in patients with thyroid nodules.
Introduction
R
Most experts agree that the current standard of care for the treatment of well-differentiated thyroid carcinoma (WDTC) is surgery, which harbors risks, namely recurrent laryngeal nerve injury and hypoparathyroidism (4). As a result, careful selection of patients for surgery is necessary. One of the challenges of thyroid nodule management still resides in accurate preoperative categorization of those nodules as malignant or benign.
Many authors have identified risk factors for thyroid cancer that help in the decision making of the management of thyroid nodules. However, tools for objective evidence-based risk stratification as opposed to individual clinical judgment have been lacking until now. The McGill Thyroid Nodule Score (MTNS) has yielded a risk estimation scale that combines 22 risk factors for thyroid cancer into a 77-point scale (Table 1). These risk factors include clinical and laboratory parameters (e.g., male sex, age >45 years, thyrotropin (TSH) >1.4 mIU/L) (5 –7), as well as imaging features (e.g., echogenicity, size, calcifications) (6,8,9) and fine-needle aspiration cytology (FNAC; e.g., degree of atypia, suspicion for malignancy) (6,10,11). In their study, Sands et al. provided support for the role of the MTNS as an accurate assessment tool for patients with thyroid nodules, finding a positive predictive value of 86% for patients with eight points or more on the scale, and 100% for scores above 19 in a sample of 844 patients (6).
TSH, thyrotropin; Tg, thyroglobulin; PET, positron emission tomography.
Continuous efforts have been made to find biomarkers that would facilitate the discrimination between malignant and benign thyroid nodules. One promising marker under investigation is serum thyroglobulin (Tg). Increasing serum levels of Tg seem to correlate with higher risk of WDTC (12,13). Therefore, we have conducted a study to investigate the value of adding preoperative serum Tg levels to the MTNS system, and here we evaluate the accuracy and usefulness of that modified MTNS system for the estimation of risk of malignancy of thyroid nodules.
Methods
The records of patients undergoing thyroidectomy at the McGill University Thyroid Cancer Centre between 2008 and 2012 were reviewed. Patients were excluded if there were insufficient data to be assigned an MTNS, if a preoperative Tg value within six months of surgery was not measured, if the patient had non-WDTC, and if the patient had a focus of incidental (i.e., not part of the biopsied nodule) papillary microcarcinoma, the ipsilateral side of the thyroid nodule was found to be confined to the thyroid on final diagnosis. However, papillary microcarcinomas with extrathyroidal extension (ETE) present on microscopic examination were included. The rationale for this selective inclusion of certain microcarcinomas lies in the difficulty of predicting their behavior. Recent studies show that whereas the majority of papillary microcarcinomas follow an indolent course, a certain proportion behaves aggressively (14). This unfavorable clinical behavior has been strongly associated with the presence of certain histopathological factors, such as ETE (14). Therefore, only papillary microcarcinomas with ETE were included in the current study.
The MTNS has been previously described (6). Cutoffs for serum Tg levels were based on previous reports (12,13,15). Scores were allotted as follow: Tg levels >75 ng/mL added one point to a patient's MTNS, and levels >187.5 ng/mL added two points. This final score was labeled MTNS+ and is displayed in Table 1.
Risk categories for malignancy were created based on positive predictive values (PPV). Groups were compared on categorical variables using the independent Student's t-test for between-group comparisons on continuous variables, and the chi-square test for between-group comparisons on categorical variables.
Ethics approval for this study was obtained from the McGill University Health Center Research Ethics Board.
Results
Of the 231 patients with complete data, 44 patients presented with papillary microcarcinomas without ETE, two with medullary carcinoma, and one with anaplastic carcinoma. Those 47 patients were excluded, as the goal of the study was to examine the predictive value of the MTNS+ for well-differentiated thyroid malignancy. Of the remaining 184 patients included in the analysis, 89 (48.37%) had a benign pathology. Of the 95 well-differentiated malignancies, 78 patients (82.1%) had papillary carcinoma, 11 (11.6%) had papillary microcarcinoma with ETE, and 6 (6.3%) had follicular carcinoma. The range of MTNS+ scores spanned from 2 to 25 in our sample, with a mean and standard deviation of 9.97±5.08. Mean MTNS+ scores were significantly higher in patients with malignant versus benign final pathology (12.16±5.49 vs. 7.63±3.26, p<0.001). The patient characteristics of the sample are presented in Table 2.
All continuous variables are presented as mean±standard deviation.
MTNS, McGill Thyroid Nodule Score; MTNS+, McGill Thyroid Nodule Score Plus; NS, not significant.
Of all patients with malignancy, 8.9% had either a false negative (3.3%) or indeterminate (5.6%) FNAC. Of these patients, all but one had a malignancy risk of ≥30% as per MTNS+. In terms of ultrasound findings, six (6.3%) patients with malignancy had dominant nodules of <1 cm, 74 (77.9%) had nodules of 1–4 cm, and 15 (15.8%) had nodules >4 cm. Of the six patients with micronodules on ultrasound, one had an MTNS+ score of 5 (28.95% risk of malignancy), one had an MTNS+ of 7 (32.65% risk of malignancy), and the remainder had scores ranging from 10 (64.86% risk of malignancy) to 23 (100% risk of malignancy). MTNS+ means were significantly higher in papillary carcinomas when compared to follicular and micropapillary carcinomas with ETE (13.04 vs. 8.88 vs. 8.83, p=0.02).
The incidence of malignancy by MTNS+ is provided in Tables 3 and 4. The malignancy rate for scores of 2–3 was 14.29%, followed by 28.95% for scores of 4–6, 32.65% for scores of 7–8, 65.86% for scores of 9–11, 71.43% for scores of 12–14, 78.57% for scores of 15–18, and 92.31% for scores of 19–22. All patients (five of five) with an MTNS+ score of 23 or more had a malignant final pathology result.
The receiver operating curve (ROC) for the MTNS+ is presented in Figure 1, with a score of eight being the most favorable point of convergence. A score less than or equal to eight corresponded to a 29.79% (28 in 94) risk, whereas a score greater than eight corresponded to a 74.44% (67 in 90) risk of malignancy. The relative risk of malignancy for patients with scores greater than eight compared to patients with lower scores was 2.5 (95% CI 1.79–3.49), and the difference in risk was significant with a p-value of <0.0001. Positive predictive value and specificity for malignancy were 54.78% and 20.22% for scores >5, 74.44% and 74.16% for scores >8, 87.5% and 95.51% for scores >14, and 100% and 100% respectively for scores >20.
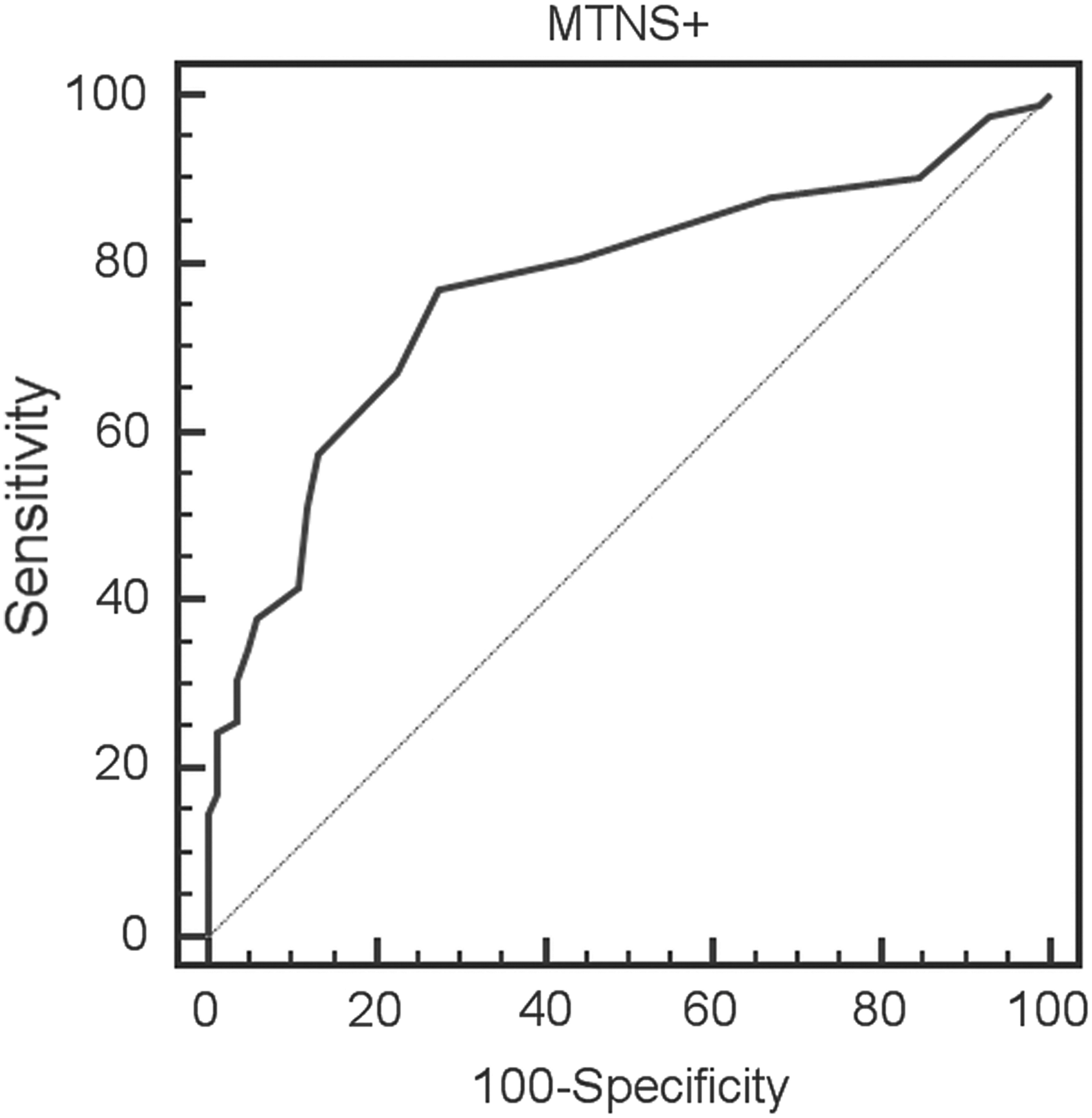
Receiver operating characteristic curve for the McGill Thyroid Nodule Score Plus.
Table 5 compares positive predictive value, sensitivity, and specificity of MTNS+ and MTNS.
PPV, positive predictive value.
Discussion
Thyroid nodules remain a challenge from both a diagnostic and a management perspective. There is a substantial body of evidence supporting individual risk factors for malignancy. However, a tool incorporating all these risk factors—derived from history, clinical exam, imaging modalities, and FNAC results—to help determine the risk of malignancy more objectively on a case-by-case basis does not exist. An objective, accurate, and integrative risk assessment system that can quantify the likelihood of malignancy within a thyroid nodule is needed.
Sands et al. elaborated the MTNS system and assessed its value in predicting the risk of malignancy in thyroid nodules. In a sample of 844 patients, they found that the relative risk of a MTNS score greater than eight was 2.66 compared to lower scores, and found the positive predictive value and specificity of a MTNS score >19 to be 100% (6). Although this scoring system is useful, we looked into other biomarkers known to be predictors of malignancy to improve the accuracy and reliability of the MTNS.
Previous studies have indicated that preoperative serum Tg levels could be a predictor of WDTC (12,13,15). More specifically, Sands et al. showed that preoperative serum Tg levels of ≥75 ng/mL have a predictive value for WDTC in patients with indeterminate FNAC (12). In line with these results, Lee et al. found Tg levels of 187.5 ng/mL to have a specificity of 90.1% for WDTC in patients with indeterminate FNAC (15). These results have raised the possibility that preoperative serum Tg levels could add to the predictive value of the MTNS. We are the first to integrate Tg levels into a comprehensive risk assessment system and to assess the value of Tg in conjunction with other risk factors.
Our study shows that including preoperative Tg levels with the existing MTNS system adds great value in the decision-making process. We found that higher MTNS+ scores correlate with an increasing risk of malignancy in our study. In fact, an MTNS+ score greater than eight was associated with a two-and-a-half-fold risk of malignancy when compared with lower scores. Our results show very high positive predictive values for malignancy with higher MTNS scores, such as >80% with scores of ≥12, >95% with scores of ≥17, and 100% with scores of ≥20. Specificity of the MTNS+ was also very good to excellent at these levels, with 88%, 98%, and 100% respectively. We believe that these findings show that the MTNS+ system is a very useful tool to quantify a given patient's risk of thyroid malignancy.
However, whereas the original MTNS compares favorably in terms of positive predictive value and specificity, the MTNS+ showed a better sensitivity for malignancy when compared to its original version, ranging from a 1.05% benefit for scores of 17 to a 10.48% benefit for scores greater than seven, including a 8.42% benefit for scores greater than eight—the optimum point of convergence of both scoring systems (Tables 4 and 5). This implies a trade-off in the addition of Tg levels to the score in that improved sensitivity is traded for a slight decrease in specificity and positive predictive value.
It is noteworthy that the benefits of Tg levels were mostly noted for higher MTNS+ scores, that is, scores with higher rates of malignancy. This shows that, in combination with a higher sensitivity, the MTNS+ is a very useful tool to assess the risk of malignancy. It provides to both the physician and the patient a quantifiable risk based on the scientific literature of the individual patient's situation as opposed to deciding solely on prior clinical experience or patient intuition. The discussion is enhanced, and management can be tailored to every patient's characteristics and own risk. For example, the follow-up and counseling of a patient with a MTNS+ greater than eight who refuses surgery—even knowing and understanding the risk of malignancy—would probably be different from a patient with a lower score. Therefore, we would argue that improvements—even at higher MTNS+ scores—become clinically relevant, particularly to the patient, when they allow them to place a numerical range on their risk of malignancy in the process of weighing risks and benefits of surgical intervention.
Recent efforts from academia and industry have resulted in the development of analytical tools aiming to help resolve diagnostic uncertainty in cases of thyroid nodules with indeterminate FNAC. Nikiforov et al. (2011) published a paper showing that analysis for 87 gene mutations including BRAF, RAS, and RET/PTC can provide useful data to help to determine malignancy in thyroid nodules (16). Further, a recent industry-sponsored trial found good sensitivity as well as negative predictive value for Afirma, a gene expression assay, in the identification of malignant nodules (17). However, in a resource-limited setting, the high cost of this test modality becomes problematic. At high-volume tertiary centers such as the McGill University Health Center, where more than 3000 patients with thyroid nodules are evaluated each year, Afirma testing of each sample of indeterminate cytology would impose a significant monetary burden on both the center in question as well as the healthcare system as a whole. Initial risk stratification with an evidence-based screening tool such as the MTNS+ may present a significantly more cost-effective alternative, and can be applied to a large patient population at minimal expense.
Some limitations to the study should be noted. First, the current study is retrospective and not prospective. Whereas this methodological approach allows for access to a very large study population, it limits access to complete data for all variables under study, which is reflected in the significant number of excluded cases in this study. Nonetheless, these results are in agreement with previous literature on the MTNS. Statistical significance was reached in our analysis, attesting to the strength of the associations observed herein. Also, only patients undergoing thyroidectomy were included in our study. The high incidence of malignancy in our study (almost 50%) is not reflective of the general population with thyroid nodules. However, this approach allowed us to maximize the yield of malignancy for the purpose of adequately powering our analysis and to compare MTNS and MTNS+ with final pathology results. The purpose of the MTNS+ is to facilitate decision making in patients in whom surgery is considered a treatment option. Including surgical candidates in the current study is thought to reflect the population for whom this scoring system will be used. Also, limitations associated with Tg assays should be noted. More specifically, false-negative and false-positive Tg results due to nonsecreting carcinomas, deviations in Tg immunoreactivity, or autoantibody interferences may reduce the diagnostic accuracy of the assays (18,19). At our center, we test for these antibodies directly using the Immulite 2000 anti-Tg Ab assays (Siemens, Llanberis, United Kingdom), which has an analytical sensitivity of 2.2 IU/L. At our institution, values >20 IU/L are considered positive (despite the manufacturer's suggestion of a 40 IU/L cutoff) in an effort to capture most individuals with potential antibody interference. All entirely undetectable Tg levels (<1 μg/L) in an individual with an intact thyroid are considered abnormal and suggestive of occult antibody interference, and have been excluded from the analysis. Heterophilic antibody interference is generally considered less of a problem with Tg assays, as shown by a recent study (20).
We have demonstrated a considerable increase in the risk of malignancy for patients with MTNS+ scores greater than eight, as well as a progressive risk increase with a higher MTNS+ score culminating in a >95% positive predictive value for scores >17 and a perfect positive predictive value and specificity for scores >20. However, we did not want to propose an ultimate cutoff value for surgical decision making. The MTNS+ was developed to guide physicians and patients through the provision of a tangible and reliable risk estimate of thyroid cancer of a thyroid nodule rather than to replace clinical judgment.
In conclusion, the results of the current study demonstrate the usefulness and accuracy of a scoring system based on well-established risk factors for WDTC. Adding Tg levels to the MTNS, thereby creating a new scoring system named the MTNS+, improves the sensitivity values of the original scoring system. As such, our results support the role of the MTNS+ as a valuable tool for endocrinologists, surgeons, and patients in order to empower informed, evidence-based decision making. Prospective studies are ongoing to confirm the current risk reference values for the MTNS+, and to compare the comprehensive approach of the MTNS+ with ultrasound only as well as ultrasound with FNAC and/or mutation testing.
Footnotes
Author Disclosure Statement
There are no actual or potential conflicts of interest either of a financial or intellectual nature for all authors and members of the research team.