
Abstract
Background:
Survivin is involved in human cancer and is responsible for aggressive biological behavior and poor clinical outcomes in several human malignancies. Thus, we hypothesized that the upregulation of survivin protein expression may be enhanced in parallel with transition toward a poorly differentiated phenotype in human thyroid carcinomas.
Methods:
The expression of survivin was evaluated, using a standard linked streptavidin-biotin horseradish peroxidase technique technique, in a series of 56 human thyroid carcinomas (42 papillary, 4 poorly differentiated, and 10 anaplastic carcinomas) and thyroid carcinoma cell lines at different degrees of differentiation.
Results:
The cytoplasmic expression of survivin protein was significantly upregulated in all thyroid tumors. A statistically significant association was found between nuclear survivin expression and anaplastic thyroid cancer (mean±SD: well-differentiated thyroid cancer, 1.22±20.21; non–well-differentiated thyroid cancer, 34.00±25.17; anaplastic thyroid cancer, 56.50±22.10; p<0.001). Nuclear staining of survivin has been shown in poorly differentiated and anaplastic thyroid carcinomas, and this is likely due to the upregulation of the ΔEx3 survivin splicing variant, as shown in poorly differentiated/anaplastic thyroid carcinoma cell lines. Of note, selected thyroid tumors characterized by a mixed population of differentiated and undifferentiated neoplastic cells, likely progressing from well to poorly differentiated and anaplastic phenotypes, exhibited cytoplasmic expression of survivin in differentiated fields and nuclear protein staining in poorly differentiated and anaplastic areas. This expression profile provides substantial added value to conventional clinical markers in predicting anaplastic cancer. The cut-off for distinguishing thyroids that developed ATC from those that remained differentiated was >30% of nuclear survivin expression. The receiver operating characteristic (ROC) area was 0.92, with a p-value of <0.0001.
Conclusions:
Upregulation of survivin expression may be a molecular marker of dedifferentiation in thyroid epithelial carcinomas, likely being responsible for survival responses of tumor cells and, thus, favoring progression toward a poorly differentiated phenotype.
Introduction
T
Considerable interest has been focused on the identification of regulators of programmed cell death or apoptosis, which may influence the cell death/cell viability balance in cancer. In particular, deregulation of apoptosis, that is, aberrantly reduced cell death, is thought to participate in cancer by facilitating the insurgence of additional transforming mutations. In addition to pro- and anti-apoptotic Bcl-2 molecules, a gene family of inhibitors of apoptosis (IAP proteins) has been recently identified. Some IAPs target a downstream step in apoptosis by inhibiting the terminal effectors caspase-3 and -7, and interfering with processing/activation of caspase-9 (11,12).
Survivin is a recently characterized member of the IAP gene family, involved in both programmed cell death and mitosis (13 –15). It is abundantly expressed in various solid as well as hematologic malignancies, but it is undetectable in most normal adult differentiated tissues. Survivin expression was correlated with unfavorable outcomes in neuroblastoma (16), reduced overall survival in colorectal (17) and recurrent colorectal cancer (18), non-small-cell lung (19), and breast cancer (20), and increased rates of recurrences in bladder cancer (21).
Despite the redundancy of cell-death pathways, survivin appears to be required for cancer-cell viability, and interference with survivin expression/function has been associated with catastrophic defects of mitotic transition and induction of mitochondrial-induced cell death (22). In cancer-cell models, overexpression of survivin provided a broad cytoprotective mechanism, counteracting apoptosis induced by FAS/TNF legation, pro-apoptotic Bax, effector caspases, and various chemotherapeutic drugs. These features are consistent with a critical role of apoptosis inhibition in tumor progression (23).
Growing evidence suggests that survivin expression in cancer-cell nuclei may represent an important prognostic marker to predict disease outcome for cancer patients (24). Retrospective analyses of several solid tumors have linked survivin expression to decreased overall survival, aggressive disease, resistance to therapy, and accelerated rates of recurrence (22). Moreover, expression of survivin together with survivin splice variants has been associated with poor disease-specific and progression-free survival (23,25). The aim of this study was to investigate the expression of survivin in thyroid carcinomas and its potential value as a predictor of tumor progression.
Materials and Methods
Study population
Upon approval by the Ethical Committee of the University of Foggia, we identified 56 patients (37 males) with a mean age of 58 years (range: 24–103 years) from the University of Foggia Thyroidectomy Registry, from the Endocrine Unit of Second University of Naples, from Mazzoni Hospital (Ascoli Piceno), and from the Pathology Unit of the University of Siena. Patients originated from Foggia, Ascoli, Siena, and Napoli and their provinces, and underwent total thyroidectomy. Forty-two of them were affected by papillary thyroid carcinoma (PTC), four by poorly differentiated thyroid carcinoma, and ten had an anaplastic thyroid carcinoma (ATC). All of them received surgical treatment with curative intention between 2000 and 2011.
Characteristics of the group of the patients, including clinical data referring to sex, age, stage, degree of differentiation, and uni/multifocality of the tumors, are shown in Table 1. All patients gave their informed written consent. Demographical and clinical data were extracted from clinical records. The histopathological diagnosis was carefully reviewed at the Department of Clinical and Experimental Medicine, Section of Pathology of the University of Foggia, and all the cases were classified as well-differentiated thyroid cancers (WDTCs), non-WDTCs, or poorly differentiated thyroid cancers (PDTCs) and ATCs, according to the last WHO classification of thyroid tumors (26). Tumor extent was revised and classified according to the recent classification system of the AJCC (27). Normal noninfiltrated thyroid tissue was obtained during the surgical removal of the gland for benign disease.
WDTC, well-differentiated thyroid cancer; non-WDTC, non-well-differentiated thyroid cancer; ATC, anaplastic thyroid cancer.
Immunohistochemistry
Briefly, 4-μm serial sections from formalin-fixed and paraffin-embedded blocks were cut and mounted on poly-
Results of the immunohistochemical staining were evaluated separately by two observers particularly trained for thyroid pathology and immunohistochemistry (AS, GP), and completely blind to the histological diagnosis and especially to follow-up data. The inter-rater reliability between the two investigators examining the immunostained sections was assessed by the Cohen's K test, yielding K values >0.70 in all instances. Normal distribution of the data was analyzed by the Kolmogorov–Smirnov test.
Immune-stained cells were counted in at least 10 high-power fields (HPF) analyzed with an optical microscope (Olympus BX41; Olympus America Inc., Melville, NY) at 40× magnification. For each case, the cumulative percentage of positive cells among all sections examined was determined. The number of survivin expressing tumor cells was estimated as a mean percentage of the final number of cells per section. A positive result was obtained with a percentage of positive cancer cells ranging from 5% to 100%. The intensity of staining was graded as weak (+), moderate (++), or strong (+++), and the cellular distribution of the marker was also reported.
Statistical analysis
Data were analyzed utilizing MedCalc v12.2.1.0 (for Windows) and R v2.11.1 (for Linux) statistical software. Multiple observations were presented as arithmetic means with standard errors of means. Statistical evaluations were carried out using one-way analysis of variance (ANOVA) and the Student–Newman–Keuls test to compare the distribution of clinical and pathological features among patients with the different locations of survivin expression (cytoplasm/nucleus). To estimate the association among anaplastic variant and nuclear expression of survivin, we conducted a multivariate multiple regression analysis to analyze and test the interaction between the degree of differentiation and different nuclear/cytoplasmic survivin expression covariates, controlling for age, sex, TNM stage, and uni/multifocality. Only p-values <0.05 were considered significant. In order to select a relevant immunohistochemical cut-off score to describe nuclear localization in ATC, receiver-operating characteristic (ROC) curve analysis was carried out. For each immunohistochemical score, the sensitivity and specificity of survivin expression for the degree of differentiation under study was plotted, generating a ROC curve. Criterion values and coordinates of the ROC curves for cytoplasmic and nuclear survivin expression in thyroid cancers are described in Table 2. The point on the curve, maximizing sensitivity and specificity of survivin for nuclear and cytoplasmic localization, was selected as the cut-off score above which survivin expression was considered a positive marker of anaplastic tumors. To use ROC curve analysis, the differentiation of carcinomas was dichotomized: DTC (WDTC+non-WDTC) or ATC. The expected average value of the ROC area is 0.5 if there is no discrimination between the groups. In order to distinguish a real discrimination between the groups from the case of no discrimination, a p-value was calculated. A small p-value makes it unlikely that the ROC area can be reconciled with the case of no discrimination. Only p-values <0.05 were considered significant.
ROC, receiver-operating characteristic; CI, 95% confidence interval.
Cell lines and immunoblot analysis
Human poorly differentiated WRO, and anaplastic BHT101 and CAL62 thyroid carcinoma cells were purchased from ATCC (Manassas, VA) and cultured in Dulbecco's modified Eagle's medium (DMEM) containing 10% (v/v) fetal bovine serum, 1.5 mM glutamine, and 100 U/mL penicillin and streptomycin. Total cell lysates were obtained by homogenization of cell pellets and normal thyroid tissue in a cold lysis buffer (20 mM Tris, pH 7.5 containing 300 mM sucrose, 60 mM KCl, 15 mM NaCl, 5% (v/v) glycerol, 2 mM EDTA, 1% (v/v) Triton X-100, 1 mM PMSF, 2 mg/mL aprotinin, 2 mg/mL leupeptin, and 0.2% (w/v) deoxycholate) for 2 min at 4°C and further sonication for 30 sec at 4°C. Immunoblot analysis was performed, as previously reported (30). Specific proteins were detected by using a rabbit polyclonal anti-Survivin (#NB500-201; Novus Biologicals) and a mouse monoclonal anti-GAPDH (sc-47724; Santa Cruz Biotechnology, Segrate, Italy).
Immunocytochemistry
Cells were grown on four-chamber tissue culture-treated glass slides (Falcon Becton Dickinson, Labware, NJ) precoated with poly-
RNA extraction and RT-PCR analysis
Total RNA from cell pellets and normal thyroid tissue was extracted using the TRIzol Reagent (Invitrogen, Milan, Italy). For first-strand synthesis of cDNA, 1 μg of RNA was used in a 20 μL reaction mixture utilizing a Transcriptor First Strand cDNA Synthesis Kit (Roche, Mannheim, Germany). For real-time PCR analysis, 0.5 ng of cDNA sample was amplified using the LightCycler 480 SYBR Green I Master (Roche) in a Light Cycler 480 (Roche). The following primers were used: main survivin isoform, forward 5′-GAC CAC CGC ATC TCT ACA TTC-3 ′, reverse 5′-TGC TTT TTA TGT TCC TCT ATG GG-3′; ΔEx3 splice variant, forward 5′-GAC CAC CGC ATC TCT ACA TTC-3′, reverse 5′-ATT GTT GGT TTC CTT TGC ATG-3′; GAPDH forward 5′-CAA GGC TGA GAA CGG GAA-3′, reverse 5′-GCA TCG CCC CAC TTG ATT TT-3′. Primers were designed to be intron-spanning. Reaction conditions were as follows: pre-incubation at 95°C for 2 min, followed by 45 cycles of 15 sec at 95°C, 30 sec at 58°C, and 30 sec at 72°C. GAPDH was chosen as an internal control. Specific bands for the ΔEx3 isoform of survivin were also visualized by standard 1.5% agarose gel electrophoresis.
Results
Histopathological and descriptive findings of the studied population
Data regarding clinicopathological findings (sex, age ranges, tumor stage, classification of carcinomas, and pattern of distributions) are shown in Table 1. Our study included 16 stage I tumors, 3 stage II tumors, 15 stage III cases, and 22 stage IV carcinomas. The mean diameter of the tumors was 2.60 cm (range: 0.4–10 cm).
In the positive cases, the intracellular localization of survivin in tumor cells was heterogeneous with a prevalent diffuse cytoplasmic distribution in all WDTC and nuclear location in the anaplastic tumors (Fig. 1). Immunohistochemical cytoplasmic positivity for survivin has been observed in all cases of PTC, with an overall higher degree of protein immunostaining than normal thyroid epithelium. On the other hand, immunohistochemical nuclear positivity for survivin has been observed in all but one case of anaplastic carcinomas, with an overall higher degree of protein immunostaining than normal thyroid epithelium and PTC.
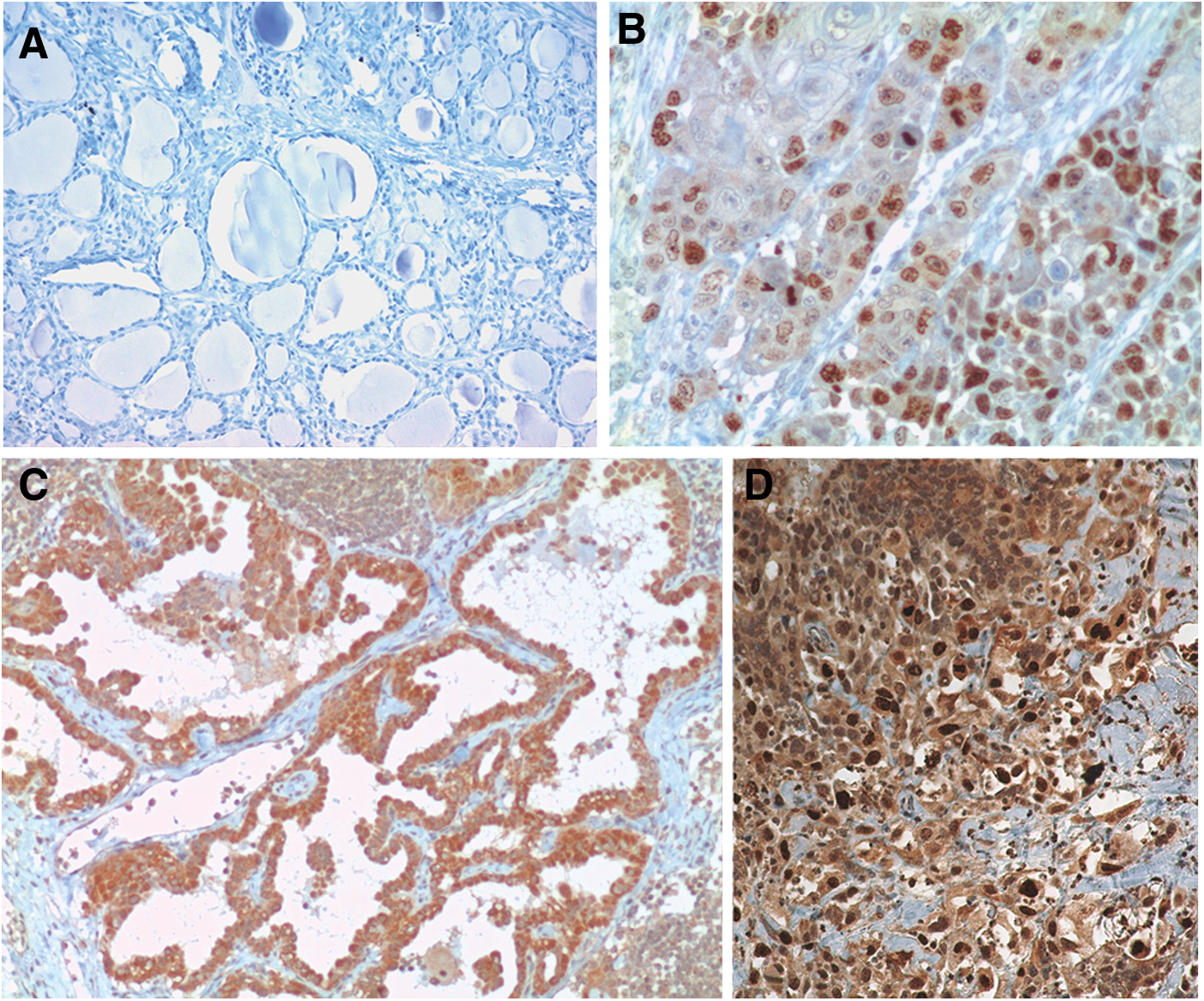
Survivin expression in thyroid cancers, as evaluated by immunohistochemistry: morphological evaluation.
Moreover, of note, selected thyroid tumors characterized by a mixed population of differentiated and undifferentiated neoplastic cells, likely progressing from well to poorly differentiated and anaplastic phenotypes, have exhibited cytoplasmic expression of survivin in differentiated fields and nuclear protein staining in poorly differentiated and anaplastic areas.
In order to evaluate further whether the nuclear survivin staining observed in poorly differentiated/ATC depends on the expression of the ΔEx3 splicing variant, whose localization is known to be restricted to the nucleus (31), we analyzed survivin expression in normal thyroid gland and in poorly differentiated WRO and anaplastic BHT101 and in CAL62 thyroid carcinoma cell lines. Indeed, the RT-PCR analysis showed a parallel upregulation of the main survivin isoform and the ΔEx3 splicing variant in poorly differentiated/ATC cells compared to normal thyroid tissue (Fig. 2A). Of note, the mRNA encoding for the ΔEx3 survivin isoform is poorly expressed in the thyroid gland and is upregulated in thyroid carcinoma cell lines (Fig. 2B). In parallel experiments, the immunocytochemical evaluation of survivin expression in WRO, BHT101, and CAL62 cells exhibited significant survivin nuclear staining (Fig. 2C). The immunoblot analysis confirmed the upregulation of the 16.7 kDa survivin corresponding to the ΔEx3 splicing variant (Fig. 2D).
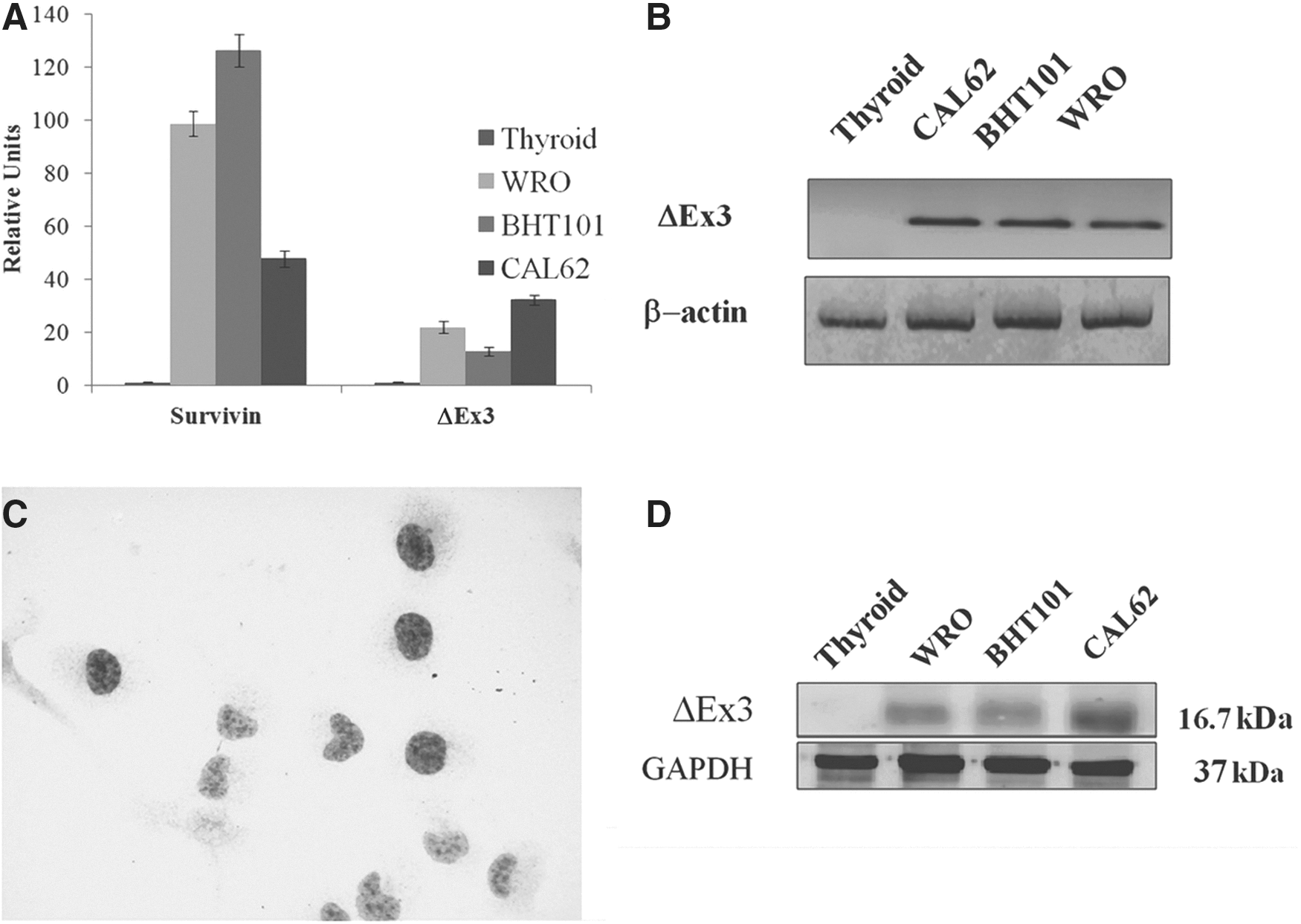
ΔEx3 survivin expression in thyroid carcinoma cell lines.
Statistical analysis
The ANOVA/SNK test was employed to describe the association between the location of survivin expression and the degree of differentiation. A significant statistical association was found between nuclear survivin expression and anaplastic cancer (mean±SD: WDTC, 1.22±20.21; non-WDTC, 34.00±25.17; ATC, 56.50±22.10; p<0.001; Fig. 3). No association with cytoplasmic survivin expression was observed (Fig. 3). Then, multivariate multiple regression analysis was used to assess independent predictors of ATC among histopathological and descriptive variables that have shown statistically significant correlation by univariate analyses. A statistically significant association was found between ATC and nuclear survivin expression (r=0.7327; p<0.0001) and with stage (Group 1: stage I, II, III; Group 2: stage IV; r=0.5796; p=0.0483). No statistical association was observed with other investigated covariables (cytoplasmic survivin expression, age, uni/multifocality).

Survivin expression in thyroid cancers as evaluated by immunohistochemistry: statistical analysis. Mean percentage of survivin cytoplasmic
Receiver-operating characteristic curve analysis
With respect to survivin expression, the most significant cut-off scores in anaplastic tumors were >30% for the nuclear survivin expression, whereas cytoplasmic expression was not significant. The receiver-operating characteristic (ROC) areas were 0.92 ([95% confidence interval (CI) 0.810–0.973]; Youden index J: 0.835; p<0.0001) for nuclear survivin expression and 0.57 ([CI 0.438–0.708]; Youden index J: 0.23; p=0.49) for cytoplasmic survivin expression.
Discussion
The overall incidence of thyroid cancer is rising for reasons that remain unclear, and recurrence is a common event (15–30% of patients), even in early-stage disease (32). Therefore, it is crucial to identify high-risk patients in order to implement more aggressive therapy and adequate monitoring.
A recent genome-wide expression profiling approach (Gene Set Enrichment Analysis; GSEA) and in vitro and in vivo functional studies have revealed that BRAFV600E, the most common genetic mutation in PTC, affects extracellular matrix composition and promotes thyroid cancer migration and invasion. BRAFV600E, through the phospho-MEK1/2 and phospho-ERK1/2 pathway, may control a network of genes crucial in integrating and regulating the extracellular and intracellular signaling in thyroid cancer cells, which may be fundamental to trigger an abnormal cell differentiation/totipotency and shape/polarity, in this way contributing to tumor aggressiveness mechanisms (i.e., cell adhesion, migration, and invasion) (33). BRAF mutations alone may not be sufficient to induce dedifferentiation, and the true predictive nature of BRAF mutations for aggressive behavior remains a topic of debate. Angiogenesis, the formation of new blood vessels from pre-existing vasculature, also plays a key role in the development, growth, and metastases of carcinomas (34). Potential stimulators of angiogenesis, such as vascular endothelial growth factor A (VEGF-A), have also been identified in PTC (35), in which their expression appears to be closely correlated with tumor size, extrathyroidal invasion, stage, and the presence of a BRAF mutation.
Although there are three types of VEGF receptors, VEGF receptor 2 (VEGFR2; also named KDR or FLK1) is the principal receptor that transmits VEGF-A signals in vascular endothelial cells, which subsequently results in enhanced endothelial cell proliferation (angiogenesis) and migration (36). An aggressive subtype of PTC is resistant to treatment with VEGFR2 inhibitors. Shaik et al. have shown that the ubiquitin E3 ligase SCF(β-TRCP) promotes ubiquitination and destruction of VEGFR2. Therefore, β-TRCP knockdown causes accumulation of VEGFR2, resulting in increased activity of signaling pathways downstream of VEGFR2. Importantly, these investigators have found an inverse correlation between β-TRCP protein levels and angiogenesis in PTC, also showing that high levels of β-TRCP inhibits cell migration and decreases sensitivity to the VEGFR2 inhibitor sorafenib in poorly differentiated PTC cells (37).
Other molecules involved in cancer progression such as survivin are becoming a focus of scientific interest. Since its discovery in 1997 (13), survivin has attracted attention as a unique member of the IAP gene family with a potential dual role in apoptosis inhibition and regulation of mitosis. However, the subcellular distribution of survivin has been controversial, and it has been variously described as a microtubule-associated or a chromosomal passenger protein. The preponderant survivin pool is associated with microtubules and participates in the assembly of a bipolar mitotic spindle (38). In addition, a mitochondrial pool, localized in the intermitochondrial membrane space, exists (39) as evidence of the dynamic nature of survivin (38). Survivin localization to mitochondria may be preferentially, or exclusively, associated with oncogenic transformation (39). On the other hand, the cytoplasmic pool is representative of its active anti-apoptotic function, and is associated with parameters of poor prognosis in most human cancers, including carcinomas of the oral cavity, lung, breast, colon, stomach, esophagus, and pancreas (40,41).
Data on survivin expression in thyroid carcinomas are limited. Its diagnostic value and its prognostic role remain poorly understood.
At the gene expression level, Xiang et al. evaluated survivin mRNA expression by quantitative RT-PCR in a group of 98 thyroid carcinomas, finding that the expression rate of survivin was closely related to cell proliferation activity, pathological type, lymph-node metastasis, and hematogenous metastasis (42). Dong et al. stated that survivin expression was significantly correlated with angiogenesis, measured as levels of VEGF expression, and with clinical stages and lymph-node metastasis (43). Zhang et al. observed higher mRNA expression and positive immunostaining for survivin in thyroid carcinoma compared with thyroid adenomas and normal thyroid tissue, with a significant positive correlation with histological type, clinical staging, and lymph-node metastasis (44). Haghpanah et al. proposed survivin as a potential diagnostic marker for the discrimination between follicular thyroid adenomas and follicular thyroid carcinomas (45). Only Ito et al. reported significantly higher levels of survivin expression in ATC than in papillary or follicular carcinomas, suggesting that survivin is strongly related to the dedifferentiation of thyroid carcinoma (46).
By IHC and RT-PCR, Chen et al. found significant differences in survivin expression between carcinomas tissues and thyroid goiter. In their study, higher survivin expression was found in the tumor tissues of pT3/pT4 lesions, in undifferentiated carcinomas, and in the tumors with lymph-node and distant metastasis. They additionally demonstrated that siRNA directed against survivin markedly decreased the protein expression, indicating that siRNA may have potential as a therapeutic modality in the treatment of human thyroid cancer (47). Yazdani et al. observed a statistical correlation of a survivin polymorphism at position -31 (G/C) (rs 9904341) with the risk of PTC in an Irananian population. They also have reported that the presence of the C allele was significantly associated with the presence of more aggressive manifestations, including lymph-node involvement, vascular involvement, and multifocality (48).
Resistance to chemotherapy predicts an unfavorable outcome for patients with radioiodine-insensitive thyroid cancer. Tirrò et al. showed that, in thyroid cancer cells, early resistance to chemotherapeutic agents requires high levels of c-IAP1 and survivin and low levels of Smac. Furthermore, increased expression of c-IAP1 and survivin contributes to the acquisition of permanent resistance to cytotoxic compounds. Silencing of these proteins by RNA interference can restore sensitivity to doxorubicin and cisplatin (49).
In terms of subcellular survivin distribution, Antonaci et al. showed an exclusive cytoplasmic immunohistochemical expression of the protein in large PTC and microcarcinomas (50). In our study, survivin protein expression pattern showed a cytoplasmic localization in well-differentiated PTC, and a nuclear localization in anaplastic tumors. Recent immunohistochemical studies have shown that survivin is localized either in nuclear or in cytosolic compartments (38). The nuclear survivin corresponds to the ΔEx3 isoform (51). Numerous authors have suggested that nuclear survivin expression in cancer cells may be interpreted as an important prognostic marker to predict disease outcome for cancer patients, being associated with an unfavorable prognosis in many malignancies (52 –54). Other current reports in this research area, however, seem to contradict the negative prognostic value of survivin nuclear expression, proposing the neoplastic nuclear localization of the marker as a predictive factor of a favorable outcome (55 –57).
In the thyroid, Vandghanooni et al. found by RT-PCR that survivin-ΔEx3 is significantly upregulated in malignant thyroid carcinoma tissues (approximately 10-fold) compared to normal tissue (58). They suggested that gene expression of the survivin gene and its splice variant, survivin-ΔEx3, could be potential candidates as reliable biomarkers in the diagnosis of human PTC (58). It is intriguing that the upregulation of the ΔEx3 nuclear variant of survivin was observed mostly in poorly differentiated and anaplastic carcinomas, which typically have a low affinity for radioiodine. Further studies are needed to evaluate whether positive nuclear survivin staining may represent a biomarker predictive of resistance to radioiodine therapy in poorly differentiated thyroid tumors that, at present, are selected based only on clinical parameters (59). Thus, because precise determination of prognostic factors remains an essential step in the evaluation of thyroid cancer patients, further investigations on larger and more heterogeneous populations should be carried out to validate and extend our results. They should further address the possible prognostic significance of the different intracellular isoforms, and correlations of the various survivin isoforms with patient outcomes, and response to radioiodine therapy.
Conclusions
Our study suggests an important role of survivin in thyroid cancer progression. The overexpression and the subcellular localization of survivin may identify a cohort of tumors with aggressive biological and clinical behavior, rapid progression toward a poorly differentiated phenotype, and poor prognosis. This may be helpful in order to improve patient management and provide novel prognostic tools to differentiate among the numerous thyroid neoplastic entities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.