
Abstract
Background:
Hashimoto's thyroiditis (HT) is a common organ-specific autoimmune disease. Antithyroglobulin antibodies (TgAb) and antithyroperoxidase antibodies (TPOAb), predominantly of the immunoglobulin (Ig) G class, are hallmarks of HT. It has been reported that HT can be divided into IgG4 and non-IgG4 thyroiditis. The aim of our study was to investigate the meaning of this classification.
Methods:
Thyroid sections from 53 Hashimoto's patients with stored serum samples were collected to detect IgG4, IgG, α-smooth muscle actin, and transforming growth factor-β1 expression by immunohistochemical staining. The degree of fibrosis of thyroid parenchyma was qualitatively evaluated by Masson's trichrome. Serum total IgG, IgG4, TPOAb IgG, TgAb IgG, TPOAb IgG4, and TgAb IgG4 were detected by enzyme-linked immunosorbent assays (ELISAs).
Results:
Based on immunohistochemistry for IgG4 and IgG, 12 cases of IgG4-positive HT and 41 cases of IgG4-negative HT were identified in our study. The patients in the IgG4-positive HT group were significantly younger than those in the IgG4-negative HT group (p=0.023), and no significant differences were found in sex distribution, disease duration, and distribution of thyroid functional status between these two groups. The degree of fibrosis evaluated by Masson's trichrome and the immunohistochemical expression score of TGF-β1 in the IgG4-positive HT were significantly higher than those in the IgG4-negative HT (p<0.05). No significant differences were found in the levels of serum IgG4, total IgG, or IgG4/IgG ratio. However, TPOAb IgG4 and TgAb IgG4 levels and the ratios of TPOAb IgG4/TPOAb IgG, TgAb IgG4/TgAb IgG, TPOAb IgG4/IgG4, and TgAb IgG4/IgG4 were significantly higher in the IgG4-positive HT group than those in the IgG4-negative HT group respectively (p<0.05).
Conclusions:
Our study indicates that HT can be divided into IgG4-positive and IgG4-negative HT, and this classification might have important clinical implications. The levels of IgG4 binding to specific thyroid antigens might be noninvasive markers to differentiate these two different immunophenotypes.
Introduction
H
The typical histopathologic features of HT usually consist of diffuse lymphoplasmacytic infiltration, which consist predominantly of T cells intermixed with B cells and are associated with oxyphilic changes of follicular cells and obliteration of thyroid follicles (6). Some of these patients exhibit extensive replacement of thyroid parenchyma by dense fibrous tissue, and this histological picture is defined as fibrosing variant of HT (FVHT). Similar histopathologic features have also been noted in IgG4-related disease (IgG4-RD), the critical histopathologic features of which are a dense lymphoplasmacytic infiltration, a storiform pattern of fibrosis, and obliterative phlebitis (7). In 2010, a Japanese research group reported that a subset of HT may be classified as a member of the IgG4-RD spectrum (8), the findings of which have recently been confirmed by another group (9).
The aim of our study was to investigate whether HT can be divided into IgG4-positive and IgG4-negative HT and to explore further the meaning of this classification.
Materials and Methods
Study groups
Hashimoto's patients who underwent total or subtotal thyroidectomy were enrolled in the current study at Peking University First Hospital from April 2009 to August 2012. In all patients, serum samples were obtained before surgery and then stored until analysis. All the patients were diagnosed with HT based on the following criteria: (i) diffuse thyroid enlargement and elevated circulating thyroid antibodies; and (ii) histopathology with diffuse lymphoplasmacytic infiltration, prominent germinal center formation, oxyphilic change of follicular cells, and degeneration of thyroid follicles (10). There were 47 women and 6 men, with an average age of 47.1 years (range: 22–74 years). All patients underwent total or subtotal thyroidectomy for two reasons: nodular lesion suspicious for thyroid cancer (n=51, 96.2%) and tracheal compression (n=2, 3.8%). In the former group, the final pathology was HT in combination with thyroid cancer in 35 out of 51 patients, and thyroid specimens were obtained from the contralateral lobe with no evidence of thyroid cancer; the other 16 patients had HT alone. Seven patients had already taken thyroxine tablets due to hypothyroidism before surgery. The clinical data of all the patients were collected, and there was no evidence of other organs affected by IgG4-RD or other autoimmune diseases. None of the patients had evidence of hereditary and acquired variations in the concentration of thyroxine-binding globulin.
This study complied with the Helsinki Declaration and was approved by the Ethics Committee of Peking University First Hospital. All the patients gave written informed consent.
Preparation of tissue and serum samples
Tissue specimens were fixed in 10% neutral buffered formalin and embedded in paraffin. Serial sections were cut precisely at 4 μm from each paraffin block. Incidental findings of focal lymphocytic thyroiditis were excluded. Serum samples were collected before surgery and kept frozen at −80°C until use.
Histology and immunohistochemistry
Serial sections from each patient were stained with hematoxylin and eosin (H&E) immunohistochemical stainings and trichrome light green (Masson).
Immunostaining for IgG and IgG4 was performed using the EnVision system (Dako Cytomation, Glostrup, Denmark). Briefly, deparaffinated sections were treated with 3% hydrogen peroxide to inhibit endogenous peroxidase, and then blocked with 3% bovine serum albumin (BSA). After preliminary treatment with 0.4% pepsin, the sections were incubated overnight at 4°C with primary antibodies: anti-IgG (rabbit polyclonal, A0423, 1:8000; Dako Cytomation), and anti-IgG4 (mouse monoclonal, HP6025, 1:500; Southern Biotech, Birmingham, AL). The sections were then incubated with goat anti-mouse and anti-rabbit immunoglobulins conjugated to peroxidase-labeled dextran polymer (EnVision; Dako Cytomation) (11). Tonsil tissue served as a positive control (11). Negative controls were prepared by incubating a few sections with normal mouse IgG or normal rabbit IgG at the same dilution instead of the specific antibody; they showed no staining above the background (data not shown). IgG4-positive or IgG-positive plasma cells were counted in five different high-power fields (HPFs) (Olympus BX51T microscope, ×10 eyepiece and ×40 lens) with the highest density of positive cells (10). The ratio of the IgG4-/IgG-positive plasma cells was also calculated in each case.
Immunostaining for transforming growth factor-β1 (TGF-β1) and α-smooth muscle actin (α-SMA) was further performed. The procedures were similar as described above, except that after pretreatment of the paraffin sections, they were incubated with anti TGF-β1 (mouse monoclonal, ab27969, 1:1000; Abcam, Cambridge, United Kingdom) or anti α-SMA (rabbit polyclonal, ab5694, 1:20; Abcam), and the control sections were produced by incubating with normal mouse or rabbit IgG instead of the specific antibody. TGF-β1 levels were analyzed as follows: at least 10 randomly selected HPFs were examined, and 100 cells were counted per area of the immunohistochemically stained cell populations. The immunoreactivity was scored as 0+ if <2% of a given cell population was stained; 1+ if 2%–10% was stained; 2+ if 10%–50% was stained; and 3+ if >50% was stained (12).
In addition, thyroid sections were stained using Masson's Trichrome for qualitative evaluation of collagen deposition and fibrosis. The degree of fibrosis of thyroid parenchyma was determined by the following criteria: 1+ if less than one-third of the thyroid parenchyma had been replaced by fibrous tissue; 2+ if one-third to half of the thyroid parenchyma had been replaced by fibrous tissue; and 3+ if more than half of the thyroid parenchyma had been replaced by fibrous tissue (13). FVHT was diagnosed if the lesion was characterized by a marked fibrous replacement of one-third to the majority of the parenchyma (14). The quantification was performed by two independent researchers who were blinded to clinical data.
Detection of thyroid function
Chemiluminescence immunoassays (ADVIA Centaur; Siemens Healthcare Diagnostics, Tarrytown, NY) were used to detect total triiodothyronine (TT3), total tetraiodothyronine (TT4), and thyrotropin (TSH). All the patients were classified into three subgroups based on the results of thyroid function tests: subclinical thyrotoxicosis, euthyroidism, and hypothyroidism (including subclinical and overt hypothyroidism).
Detection of IgG4 and total IgG
Serum IgG4 and total IgG levels were measured by using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (BlueGene Biotech, Shanghai, China). All steps were performed according to the manufacturer's instructions. Briefly, standards or serum samples (diluted 1:10 for IgG4 in phosphate-buffered saline [PBS] containing 0.1% Tween 20 [PBST], undiluted for IgG) and enzyme conjugate were added to the antibody precoated microtiter plate and incubated for 1 h. After washing, substrate solution was added to each well, and the reaction was stopped with stop solution after approximately 10–15 min. The results were recorded as optical density at 450 nm.
Detection of TgAb IgG and TPOAb IgG
Serum TgAb IgG and TPOAb IgG were detected by antigen specific ELISAs. Briefly, 96-well plates (Costar, Cambridge, MA) were coated with 4 μg/mL of different antigens (Tg; Calbiochem Merck KGaA, Darmstadt, Germany; recombinant TPO ectodomain in-house) in 0.1 M carbonate/bicarbonate buffer (pH 9.6) at 37°C for 1 h and were blocked with 3% BSA. Every plate contained positive, negative, and blank controls. The volume in each well was 100 μL in all steps, and each sample was added in duplicate. Serum samples were diluted (1:50) in PBST, and incubated for 30 min. After washing, a horseradish peroxidase conjugate goat anti-human IgG (Jackson ImmunoResearch Laboratories, Inc., Baltimore Pike, PA), 1:2500 dilution, was added and incubated for 30 min. Subsequently, 0.4 mg/mL o-phenylenediamine and 1 μL/mL 3% H2O2 were used, and the reaction was stopped with 1 M hydrochloric acid after 10 min. The results were recorded at 490 nm and expressed as the optical density values.
Detection of TgAb IgG4 and TPOAb IgG4
The procedures were similar as outlined above. Briefly, 96-well microtiter plates were coated with antigens (4 μg/mL Tg or 4 μg/mL hTPO ectodomain in-house). After washing and blocking, serum samples were diluted 1:50 with PBST and incubated for 30 min. Horseradish peroxidase-labeled mouse anti-human monoclonal antibodies to IgG4 (HP6025; Southernbiotech, Birmingham, AL, 1:5000 for TgAb IgG4 and 1:1000 for TPOAb IgG4) were subsequently employed. Substrate was added and the results were recorded at 490 nm.
Statistical analysis
Statistical analysis was performed using the SPSS v13.0 (SPSS Inc., Chicago, IL) statistical package. Data are presented as medians and interquartile range (IQR) to account for the skewed nature of the parameters. Mann–Whitney tests were performed to test for differences between groups; chi-square test or Fisher's exact test was used for comparison of proportions between variables. A p-value <0.05 was considered statistically significant.
Results
Histopathologic and immunohistochemical findings
Histologic findings of all the patients were characterized by diffuse lymphoplasmacytic infiltration, lymphoid follicle formation, destruction, and fibrous replacement of the thyroid parenchymal tissue as evaluated after H&E staining. More than 20 per high-power fields (HPFs) IgG4-positive plasma cells and greater than 30% IgG4/IgG-positive plasma cells ratio were taken as the cutoff value in our study due to the high specificity and sensitivity for defining a significant increase of IgG4-positive plasma cells in HT (8). Based on these criteria, the 53 patients were divided into two groups: IgG4-positive HT (n=12) and IgG4-negative HT (n=41). In both groups, IgG4-positive plasma cells can be detected in germinal centers (Fig. 1).

Immunohistochemistry for IgG4 and IgG.
Clinical features of all the patients
The clinical features of IgG4-positive HT and IgG4-negative HT are summarized in Table 1. In the IgG4-positive HT group, two patients had subclinical thyrotoxicosis, six were euthyroid, and four had hypothyroidism. In the IgG4-negative HT group, two patients had subclinical thyrotoxicosis, 34 were euthyroid, and five had hypothyroidism. The four patients with subclinical thyrotoxicosis had no evidence of hyperthyroidism at clinical presentation and in pathology. In the hypothyroid group, seven patients (four in the IgG4-positive HT group and three in the IgG4-negative HT group) had taken thyroxine tablets before surgery. Overall, there were no significant differences in sex distribution, disease duration, and the distribution of thyroid functional status between the two groups, but the patients in the IgG4-positive HT group were significantly younger than those in the IgG4-negative HT group (p=0.023).
Age and disease duration are expressed as median (interquartile range).
HT, Hashimoto's thyroiditis; Ig, immunoglobulin; TGF, transforming growth factor.
Comparisons of the levels of total IgG, IgG4, TPOAb IgG, TgAb IgG, TPOAb IgG4, and TgAb IgG4
Serum samples from all the patients drawn preoperatively were analyzed for total IgG, IgG4, TPOAb IgG, TgAb IgG, TPOAb IgG4, and TgAb IgG4. As shown in Table 2, there were no statistical differences in the levels of IgG4, total IgG, and the IgG4/IgG ratio between IgG4-positive and IgG4-negative HT. Moreover, no significant differences were found for TPOAb IgG and TgAb IgG levels. However, the levels of TPOAb IgG4 and TgAb IgG4, the ratios of TPOAb IgG4/TPOAb IgG, TgAb IgG4/TgAb IgG, TPOAb IgG4/IgG4, and TgAb IgG4/IgG4 were significantly higher in the IgG4-positive HT group than those in the IgG4-negative HT group (p<0.05).
Numbers are expressed as median (interquartile range). The levels of IgG4, IgG, TPOAb IgG4, TPOAb IgG, TgAb IgG4, and TgAb IgG are shown by the optical density values, and the ratios were also calculated by the corresponding optical density values.
TPOAb, antithyroperoxidase antibodies; TgAb, antithyroglobulin antibodies.
Evaluation of the degree of fibrosis of thyroid parenchyma by staining for collagen, α-SMA, and TGF-β1
The degree of fibrosis was determined by qualitative evaluation of collagen deposition using Masson's Trichrome and staining for α-SMA (Fig. 2). According to these criteria (14), 43 cases of typical HT (seven in the IgG4-positive HT group, and 36 in the IgG4-negative HT group) and 10 cases of FVHT (five in the IgG4-positive HT group, and five in the IgG4-negative HT group) were identified based on Masson's Trichrome results. Myofibroblasts, which were identified based on immunohistochemical staining of α-SMA, were concentrated in areas of collagen deposition. The degree of fibrosis in the IgG4-positive HT group was significantly more severe than in the IgG4-negative HT group (Table 1; p=0.029).
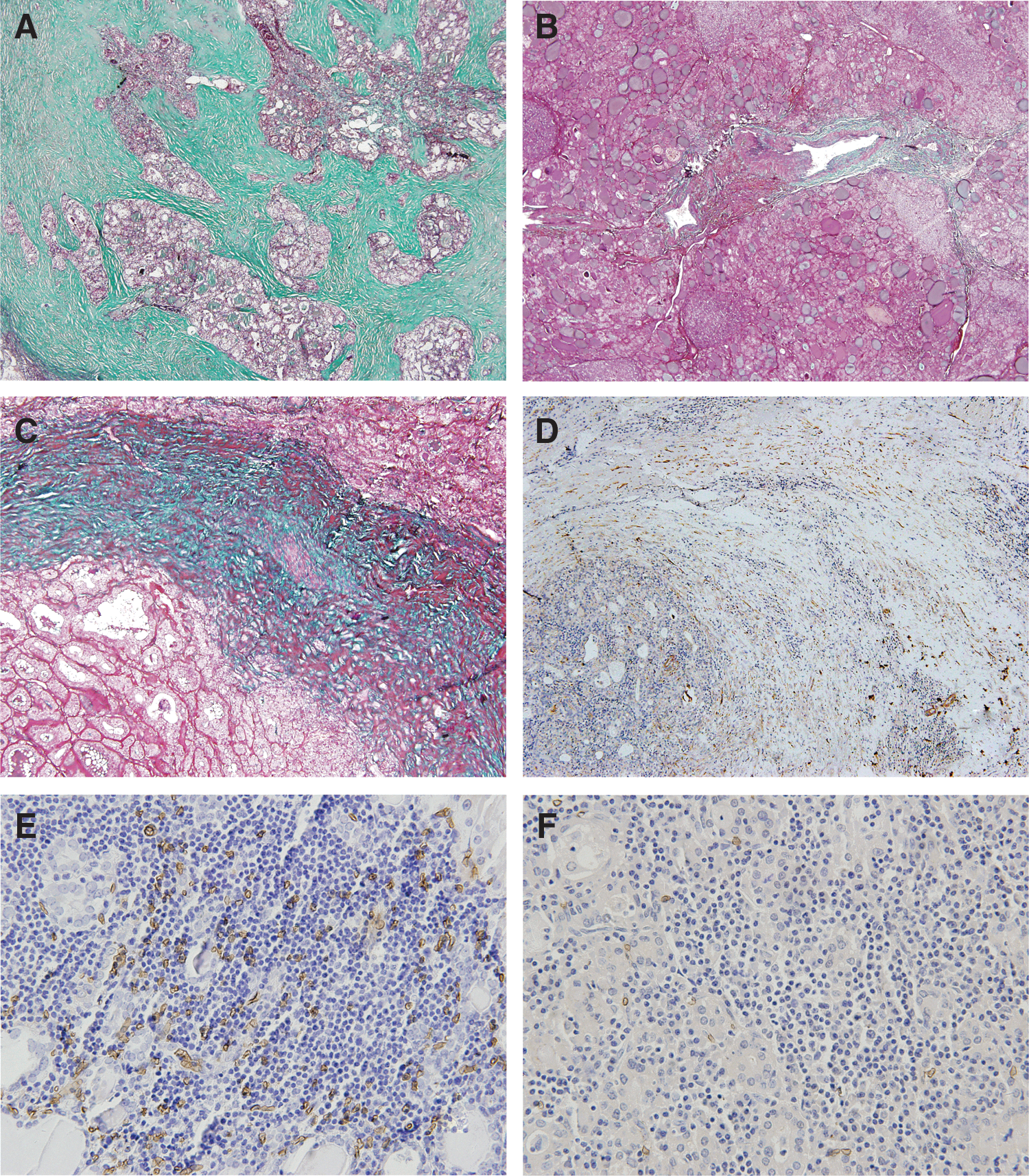
Masson's trichrome and immunohistochemistry for α-SMA, a marker of myofibroblasts, and TGF-β1, the most important profibrotic cytokine.
The immunohistochemical expression score of TGF-β1 in FVHT was significantly higher than that in typical HT (p=0.003; data not shown). It was also significantly higher in the IgG4-positive HT group than in the IgG4-negative HT group (Table 1 and Fig. 2; p<0.001).
Discussion
Our research indicates that HT can be divided into IgG4-positive and IgG4-negative groups based on immunohistochemistry for IgG4 and IgG. In the study by Li et al. (13), IgG4-positive HT was clinically associated with younger age, a lower female–male ratio, shorter disease duration before thyroidectomy, and more frequent subclinical hypothyroidism. In Kojima's study, besides a high incidence of hypothyroidism in IgG4-positive HT, no significant differences in age and sex distribution were found between these two groups (15). Our study shows that the patients in the IgG4-positive HT were younger than those in the IgG4-negative HT group, similar to the findings of Li et al. (13). No significant differences were found in sex distribution, disease duration, or the distribution of thyroid functional status between the two groups. Since thyroid specimens were collected from Hashimoto's patients with stored serum samples, there was a selection bias in the current study. In addition, given that this is a retrospective study, the time of onset and the disease duration may not have been determined entirely accurately. We speculate that a special chronic disease management system might be helpful to observe the clinical features and disease progression of different immunophenotypes of HT in the future.
Li et al. (8) and Deshpande et al. (9) have reported that IgG4-positive HT showed a significantly higher grade of stromal fibrosis. In contrast, no significant difference was found in the study of Kojima et al. (15). Our findings reveal a significantly higher degree of fibrosis of thyroid parenchyma and immunohistochemical expression score of TGF-β1 in IgG4-positive HT than in IgG4-negative HT. This observation supports the view that IgG4-positive HT might be more likely to progress to fibrosis. Katz and Vichery have reported that the thyroid function tests often indicated hypothyroidism in Hashimoto's patients with more severe fibrosis (14). Therefore, patients with IgG4-positive HT might be at higher risk of developing thyroid failure. Although we could not confirm this further in our study, thyroid function should be assessed longitudinally in such patients to detect hypothyroidism as early as possible.
TgAb and TPOAb, predominantly of the IgG class, are synthesized by B lymphocytes that infiltrate the thyroid gland (16). Antigen-specific IgG4 are produced in response to long-term exposure to different antigens from affected organs (17). Serologically, in our study, no significant differences in the preoperative serum levels of IgG4 and IgG were found between IgG4-positive and negative HT. However, the levels of TPOAb IgG4, TgAb IgG4, the ratios of TPOAb IgG4/TPOAb IgG, TgAb IgG4/TgAb IgG, TPOAb IgG4/IgG4, and TgAb IgG4/IgG4 in the IgG4-positive HT group were significantly higher. We speculate that the antigens recognized by IgG4 in thyroid specimens might be thyroid components such as thyroglobulin (Tg) and thyroid peroxidase (TPO). A number of IgG4-positive plasma cells were detected in germinal centers, which indicates that IgG4 from IgG4-bearing plasma cells are produced in the thyroid, rather than being transferred from the outside. Since HT is an organ-specific disease, the proportion of serum IgG4 reacting with thyroid-specific antigens might be a small subset of the total IgG4 and IgG. Therefore, the levels of thyroid antigen-specific IgG4, rather than the total IgG4 concentration, might be helpful to differentiate these two different immunophenotypes.
There is growing evidence to suggest that B-cell responses and autoantibody production play an important role in the pathogenesis of HT (18). So far, the lack of effector function of IgG4 and the phenomenon of half-antibody exchange raise complex questions as to whether IgG4 are pathogenic or, alternatively, mediate a counter-regulatory response to the ongoing immunologic disease (19). Since diffuse infiltration of IgG4-positive plasma cells and higher levels of serum TPOAb IgG4 and TgAb IgG4 were found in IgG4-positive HT in our study, we speculate that B-cell-mediated autoimmunity might play a more important role in IgG4-positive HT, and it might be the foundation of this classification using immunohistochemistry for IgG4 and IgG.
There is still controversy over whether HT is a member of the IgG4-RD spectrum. Li et al. first proposed that IgG4-positive HT might represent an IgG4-RD of the thyroid gland (8,20). Deshpande et al. concluded that FVHT belongs to the IgG4-RD spectrum (9). Watanabe et al. proposed that IgG4-related thyroiditis seemed to represent a new disease entity distinct from HT and Riedel's thyroiditis (21). And Stone et al. thought that HT did not appear to be part of the spectrum of IgG4-RD but was only a disease with elevated tissue and serum IgG4 concentrations (22). The diagnostic criteria of IgG4-RD published in 2011 (7) are based primarily on the morphological appearance on biopsy. In our study, IgG4-positive HT was characterized by diffuse lymphoplasmacytic infiltration, more severe degree of fibrosis of thyroid parenchyma with an elevated IgG4-positive plasma cells, and an increased IgG4/IgG ratio in the thyroid. It meets at least one of the three major histopathologic features of IgG4-RD (7). However, the typical storiform-type fibrosis was less common, and there were no reports on obliterative phlebitis in IgG4-positive HT in the current study or the literature (13). Moreover, there were no findings of elevated serum IgG4, no other affected organs could be identified in the patients with IgG4-positive HT in our study, and there are no data on response to glucocorticoid therapy. Therefore, while our study may not provide more evidence to determine whether IgG4-positive HT belongs to IgG4-RD, it confirms that HT can be divided into two different immunophenotypes. Considering the mechanism of B-cell-mediated autoimmunity in IgG4-postive HT and the good therapy response in IgG4-RD, we speculate that glucocorticoid therapy might influence the fibrosis progress in patients with IgG4-positive HT. Therefore, an early diagnosis of IgG4-positive HT might have important clinical implications for therapy in order to prevent progression to thyroid failure. Since surgery is not necessary for most patients affected by HT, it is difficult to make a definite classification before surgery. As a noninvasive marker, thyroid antigen-specific IgG4 might be helpful to discriminate these two different immunophenotypes and guide therapy.
In conclusion, our study indicates that HT could be divided into IgG4-positive and IgG4-negative HT, and that there are differences in age distribution, serologic features, and the degree of fibrosis of thyroid parenchyma between these two groups. Since the mechanism might be different, the levels of IgG4 binding to specific thyroid antigens such as Tg and TPO might be helpful to differentiate them. We speculate that this new classification might have important clinical implications for therapy, and it will provide a new view to investigate the mechanism of HT in the future.
Footnotes
Acknowledgments
This work was supported by Beijing Nova Program (No. 2011011), Program for New Century Excellent Talents in University (NCET-11-0003), and Sector Funds of Ministry of Health (No. 201002002).
Author Disclosure Statement
No competing financial interests exist.