
Abstract
Background:
Well-differentiated thyroid carcinoma in children and adolescents is a rare disease with favorable prognosis despite regional and distant metastasis at presentation in many patients. Treatment recommendations are varied and there is little consensus on follow-up guidelines for these patients.
Methods:
Medical records of patients less than 22 years of age treated at our institution were reviewed. One hundred twelve patients treated between 1969 and 2009 were selected for further analysis. Effects of patient and tumor characteristics on progression-free survival (PFS) were evaluated along with the predictive value of whole-body 131I scintigraphy in the follow-up setting.
Results:
Overall survival at 20 years and 30 years was 100% and 94.4%, respectively. PFS at 10, 20, and 30 years was 71%, 62%, and 55%, respectively. Although male patients and younger patients presented with more advanced disease, sex, and age at diagnosis had no effect on risk of PFS. Additionally, neither the presence of vascular invasion, capsular extension, positive margins, nor soft tissue invasion had an effect on PFS. Mean time to recurrence in patients who underwent immediate postoperative 131I therapy was 3.8 years compared to 14.1 years in patients who either never received 131I therapy or were treated in the salvage setting (p<0.0001). Negative posttreatment whole-body 131I scintigraphy was strongly predictive for decreased risk of recurrence, especially in patients with three consecutive negative scans.
Conclusions:
Pediatric patients are more likely to present with advanced disease and for this reason, the majority of patients treated at our institution receive postoperative 131I. Long-term surveillance is required in this population because of the risk of late recurrences. Whole-body 131I scintigraphy is useful for risk stratification; after three consecutive negative scans, the risk of recurrence is low.
Introduction
T
The appropriate initial management and follow-up for these young patients who have an excellent survival but require life-long surveillance is controversial. Surgical removal of the thyroid is performed on nearly all patients, however, cervical lymphadenectomy and postoperative treatment with 131I are variably used (4 –7). Posttreatment surveillance guidelines are not standardized, although it is known that these patients are at risk of recurrence for decades after diagnosis. Posttreatment surveillance imaging may help further characterize risk groups and guide individual treatment recommendations. In order to better understand the treatment approach and prognostic factors for thyroid cancer in children and adolescents, we retrospectively evaluated our institutional experience with patients diagnosed and treated for DTC before the age of 22 years.
Materials and Methods
Patients
Patients less than 22 years of age diagnosed with well-differentiated carcinoma of the thyroid were evaluated in this study. Patients with papillary carcinoma and its variants including follicular variant of papillary carcinoma, follicular carcinoma, and Hürthle cell carcinoma were included. Patients with medullary thyroid cancer were excluded. A total of 112 patients meeting these criteria were evaluated at the Mallinckrodt Institute of Radiology at Washington University School of Medicine between 1969 and 2009. Data were obtained by review of the medical record and/or by direct communication with the patient or parents. This retrospective study was performed under a protocol approved by the Washington University Institutional Review Board (protocol number 201010705), with waiver of consent.
Treatment and follow-up
All patients were treated with curative intent and underwent surgical resection. Surgical treatment was total thyroidectomy in 102 (91.1%), subtotal thyroidectomy in 3 (2.7%), and lobectomy in 7 (6.3%). Cervical lymphadenectomy was performed in 70% of patients, consisting of excision in 49% and modified radical neck dissection in 21%. The remaining 33 (30%) had no surgical removal of neck lymph nodes. Postoperative 131I was administered to 92 patients (82%). The administered activity of 131I given as initial treatment was determined based on our treatment guidelines, which utilize the standard guidelines for adult patients incorporating reductions based on the weight of the child (8,9). Our standard adult treatment recommendations included an administered activity of 25–50 mCi of 131I for patients who have residual normal thyroid tissue remaining resulting in minimal thyrotropin (TSH) elevation. Patients with no lymph node involvement receive 100 mCi, while lymph node-positive patients receive 150 mCi. Patients with distant metastatic disease receive 250 mCi, unless the disease includes bulky or diffuse lung involvement, in which case the dose is reduced to 50–100 mCi. For children, dose adjustments are made on a per kilogram basis using the doses described above for a standard 70-kg person.
Administered activity of 131I ranged from 25 mCi (0.93 GBq) to 270 mCi (10.0 GBq). 131I administrations were repeated for patients with persistently positive posttreatment whole-body 131I scintigraphy. At least one repeat administration of 131I was given to 45 patients (40%). Twenty patients did not receive 131I, 47 received a single administration, 26 received two, 11 received three, 4 received four, 2 received five, and 2 received six. For those patients treated with 131I, cumulative administered activity ranged from 25 mCi (0.93 GBq) to 970 mCi (35.89 GBq). Posttreatment surveillance consisted of physical examination and laboratory studies, including TSH, thyroglobulin, triiodothyronine, and free thyroxine for all patients. Beginning in the 1990s, thyroglobulin levels and thyroglobulin antibodies were monitored for all patients.
Whole-body 131I scintigraphy was performed in 74% of patients. Whole-body 131I scintigraphy was performed using an 131I dosage of 70 μCi/kg (with a maximum dosage of 5 mCi in pediatric patients). Prior to administration, patients were prepared either by withdrawal of replacement thyroid hormone or, since 1997, by thyrogen administration. Thyroid withdrawal for approximately 3 weeks was typical, after which TSH was measured and 131I given if TSH exceeded 30 μIU/mL. Thyrogen was administered on each of 2 consecutive days followed by administration of 131I on the third day. Diagnostic whole-body 131I scintigraphy was performed 48 hours after radiopharmaceutical administration using gamma cameras fitted with high-energy collimators. Typically, both anterior and posterior whole-body scans were performed, along with additional anterior, posterior, and both lateral spot images of the head and neck region. It has been our policy to perform whole-body 131I scintigraphy yearly after thyroid ablation for the first 2 years followed by a third scan 5 years after ablation if the prior scans showed no evidence of disease.
Data on the number of negative follow-up scans for each patient were collected. For analysis, patients were categorized as having persistently positive scans, one negative scan, two negative scans, or three or more negative scans. Disease recurrence was defined as new site(s) of disease on whole-body 131I scintigraphy after any number of negative 131I scans or pathologically proven recurrence in subjects where the presence of disease was suggested on physical examination. Additionally, an elevated thyroglobulin level was designated as disease recurrence, at which time further imaging, including whole-body 131I scintigraphy, ultrasonography, or 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) were performed to determine the site of recurrence. For patients with persistently positive whole-body 131I scintigraphy, progression was defined as new recurrent disease on physical examination or new areas of uptake on 131I scintigraphy.
Variables
Information regarding margin status, vascular invasion, capsular involvement, and soft tissue invasion were available for all but one patient. Extent of disease at presentation was known for all patients and was recorded as disease confined to the thyroid, involvement of the cervical lymph nodes, or pulmonary metastatic disease. Additionally, the number of consecutive negative whole-body 131I scans was evaluated with respect to risk of recurrence. Variables analyzed for effect on progression-free survival (PFS) included age at diagnosis, sex, race/ethnicity, tumor extension, vascular invasion, extent of disease, extent of surgery, and treatment with 131I. PFS curves were generated using the Kaplan-Meier method with statistical significance assessed by the log-rank method. χ2 analysis was used for comparison of age groups. t Tests were used for comparison of data with continuous variables, while χ2 tests were used for dichotomous data.
Results
Patient and tumor characteristics
Patient and tumor characteristics are shown in Table 1. Age at diagnosis ranged from 4.2 to 21.9 years with a median of 17.7 years. All patients had a minimum of 5 years of follow-up (median follow-up, 18.1 years; range, 5.0–42.8). All but four patients had either lymph node involvement or tumor size greater than 1.0 cm. Pathologic findings included thyroid capsular invasion in 61%, vascular invasion in 39%, soft tissue invasion in 30%, positive margins in 31%, and bilateral thyroid involvement in 31%. Overall, 35% of patients presented with disease confined to the thyroid, 55% had disease involving the cervical lymph nodes, and 10% had pulmonary metastatic disease. Male patients were more likely to present with metastatic disease to the lungs (21.7% versus 6.7%, p=0.031).
AJCC, American Joint Committee on Cancer.
Recurrence Characteristics and Salvage Therapy
Overall survival at 20 years and 30 years was 100% and was 94.4%, respectively, with only 1 death in the cohort (Fig. 1). One patient died of congenital heart disease 37 years after diagnosis. At the time of last follow-up, 117 patients were alive with no evidence of disease and 4 patients were alive with persistent thyroid carcinoma. Median age at last follow-up was 34.7 years (range, 11.9–63.5 years). Forty patients (36%) have experienced recurrent disease. Patterns of failure consisted of recurrence in the thyroid bed alone in 7, in cervical lymph nodes in 24, and pulmonary metastatic disease in 6. Of the 40 patients who experienced recurrent disease, treatment at the time of relapse was surgery in 9, surgery and 131I therapy in 15, 131I therapy alone in 15, and unknown therapy in 1.
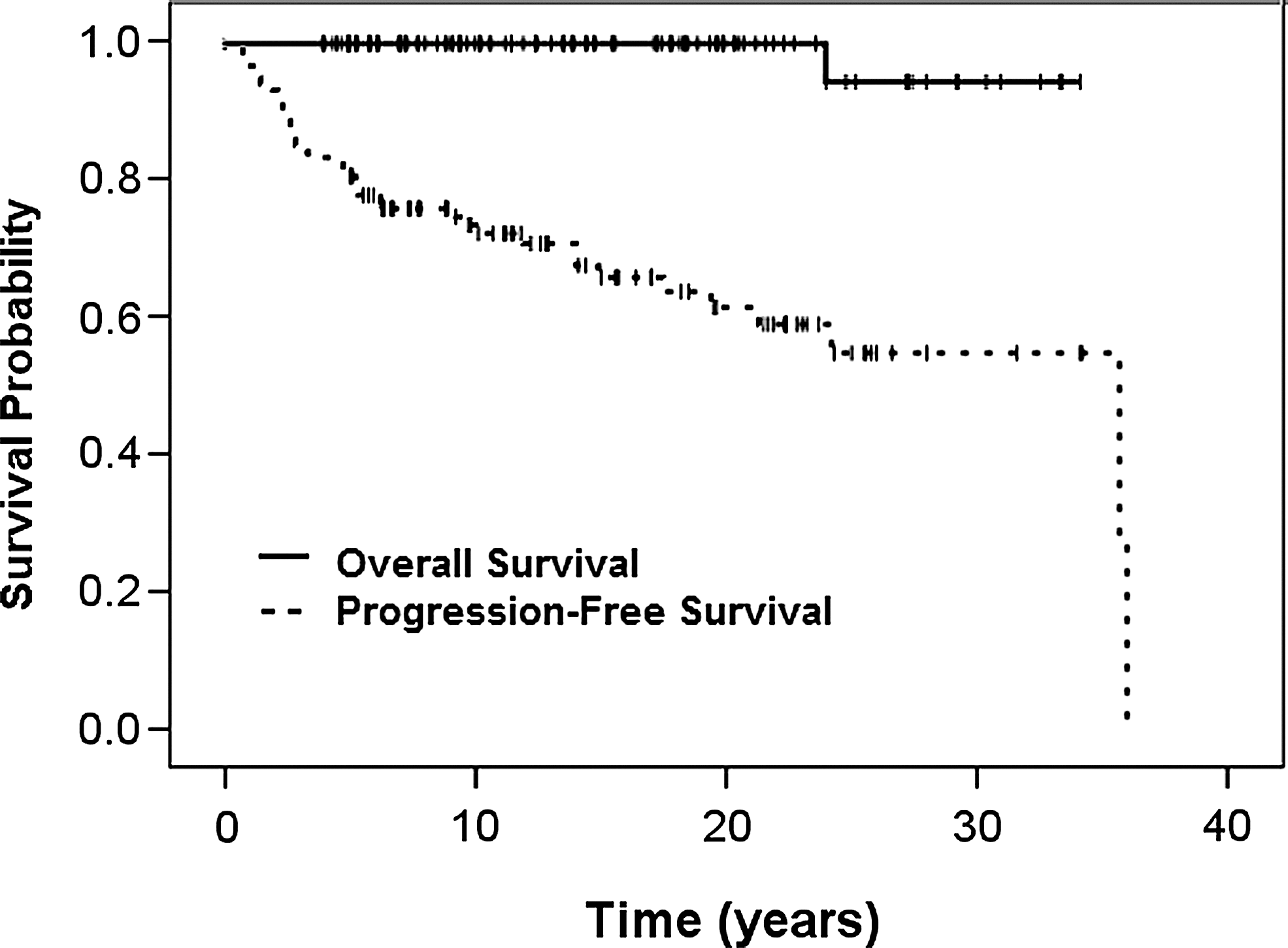
Kaplan-Meier curves of overall survival and progression-free survival for all patients (n=113).
The time to first recurrence ranged from 8 months to 36 years (mean 8.3 years, Fig. 2). The majority of recurrences occurred prior to 10 years. However, there was a significant difference in time to recurrence depending on whether or not the patient received initial 131I therapy. Mean time to recurrence in patients who underwent immediate postoperative 131I therapy was 3.8 years compared to 14.1 years in patients who either never received 131I therapy or were treated in the salvage setting (p<0.0001). No patients treated with 131I failed after 20 years of follow-up, whereas 25% of the recurrences in patients not treated with 131I failed after 20 years, with 2 recurrences after 35 years.

Time to first recurrence in years. The percentage of patients experiencing recurrence in each time frame is on the y-axis.
Prognostic factors
PFS at 10 years, 20 years, and 30 years was 72.2%, 63.0% and 45%, respectively (Fig. 1). Although male patients and younger patients presented with more advanced disease, sex and age at diagnosis had no affect on risk of progression. Additionally, neither the presence of vascular invasion, capsular extension, positive margins nor soft-tissue invasion had an effect on PFS. Patients with tumor in both lobes of the thyroid had worse PFS than those with unilateral disease (p=0.043). The recurrence rates were 22% in patients with disease confined to the thyroid, 42% in patients with cervical lymph node involvement, and 46% in patients with pulmonary metastases (p=0.103). There was a trend toward improved PFS in patients with disease confined to the thyroid but this did not reach statistical significance (p=0.079). Extent of local surgery was total thyroidectomy for 90% of the patients. We were unable to demonstrate any detriment in PFS for patients who underwent subtotal thyroidectomy or lobectomy. We were also unable to correlate removal of cervical lymph nodes with risk of recurrence. For patients treated with postoperative 131I, PFS was 70% at both 10 and 20 years of follow-up. For patients treated with surgery alone, 10- and 20-year PFS was 56.4% and 12.8%, respectively.
Tumor characteristics and outcome were also analyzed for patients stratified by age. Comparing patients less than 16 years of age to patients between the age of 16 and 21 years of age there was no difference in race/ethnicity or sex. However, the younger patients were significantly less likely to have disease confined to the thyroid gland (17.6% versus 42.3%, p=0.012). Lung metastases were present in 18% of patients less than 16 years of age compared to 6% of the older patients (p=0.066). Additionally, younger patients were more likely to have vascular invasion and soft tissue invasion (p=0.018 and 0.006, respectively). However, there was no difference in PFS or overall survival based on age.
Follow-up whole-body 131I scintigraphy and thyroglobulin levels
To determine the predictive value of surveillance whole-body 131I scintigraphy in this pediatric population, we evaluated recurrence risk as a function of consecutive negative scans. A total of 84 patients (75%) underwent whole-body 131I scintigraphy. Persistently positive scans occurred in 18 (21%) patients. There were 49 patients with one negative scan or two consecutive negative scans. Within this group, 11 patients (22.4%) experienced a recurrence. Recurrence was identified with positive whole-body 131I scintigraphy with or without elevated thyroglobulin levels in 10 patients (91%). No recurrences occurred in patients who had three consecutive negative scans. Patients with three consecutive negative scans experienced an improved PFS (p=0.048, Fig. 3).
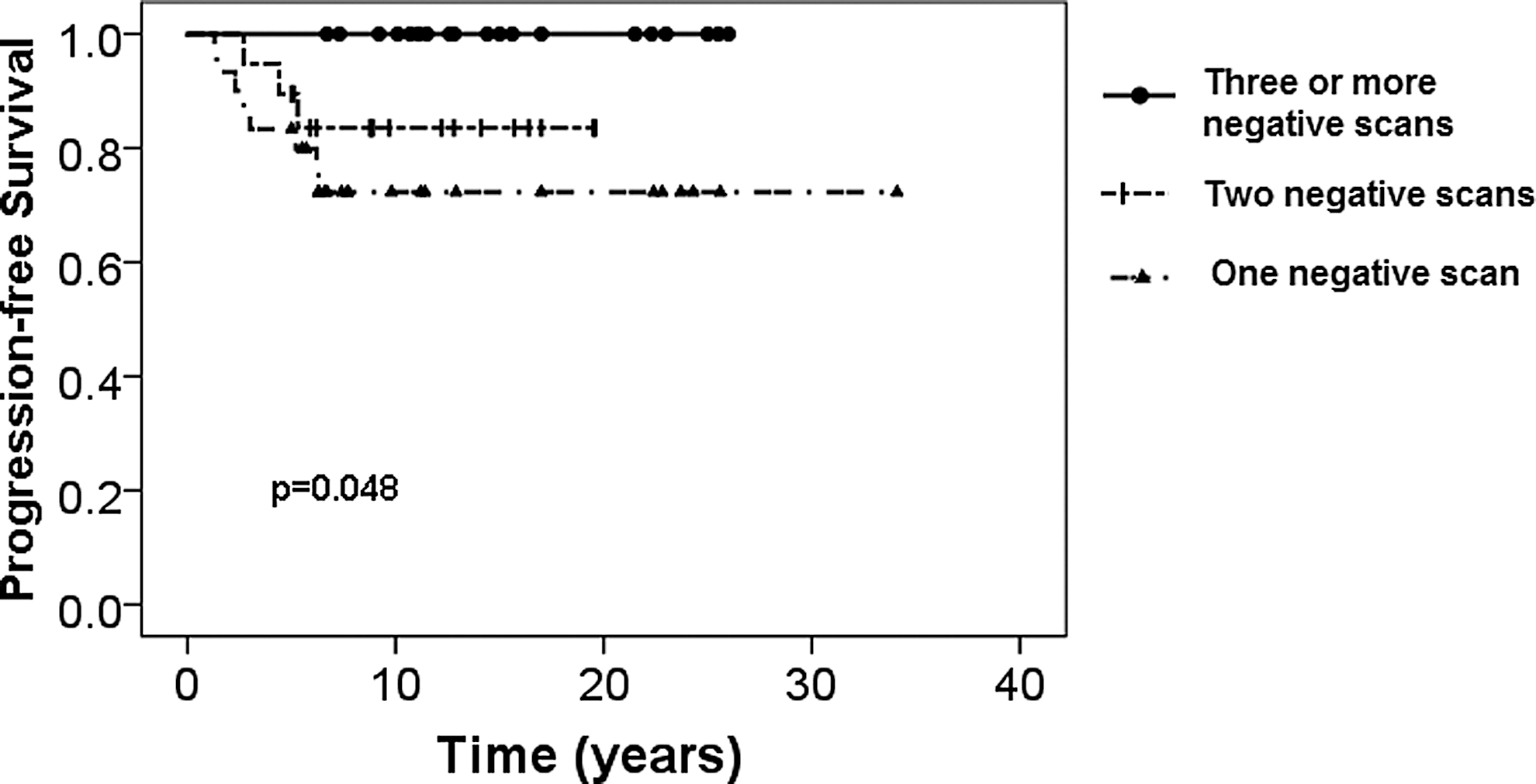
Progression-free survival stratified by number of consecutive negative whole-body 131I scans.
Most recurrences were accompanied by an increase in serum thyroglobulin. However, 11 of 52 patients (21%) tested positive for thyroglobulin antibodies, thus rendering their thyroglobulin results unreliable. We indentified 3 patients who achieved negative serum thyroglobulin levels in the absence of thyroglobulin antibodies and who then developed recurrent disease. Recurrence was detected by whole-body 131I scintigraphy in all of these patients. Additionally, 1 patient had an elevated thyroglobulin level with no evidence of disease on whole-body 131I scintigraphy. This patient's disease was identified by FDG-PET.
Discussion
Well-differentiated thyroid cancer is often regarded as a distinct disease in children compared to DTC in adults. Although younger patients are more likely to present with regional and distant disease, overall survival is excellent as reported in several series (1,4 –6,10 –12). No randomized trial data exist to guide treatment recommendations for pediatric patients. Nearly all patients undergo surgical removal of the thyroid, although removal of cervical lymph nodes and use of postoperative 131I therapy vary. Additionally, risk factors associated with recurrence differ among published reports and there are few data on the use of imaging studies for predicting risk of relapse (13 –16).
Patient and tumor characteristics of our cohort are similar to those in previous studies. We find the majority of patients are females, with male patients and younger patients presenting with more advanced disease. Overall survival at 20 and 30 years was 100% and 94.4%, respectively. No patients died of thyroid cancer. Previous studies, including prior data from our institution, have demonstrated worse PFS in younger patients, those with positive margins, and patients with more advanced disease (5,6). Extent of disease, age, sex, and positive margins had no significant effect on PFS. We postulate this difference is attributable to treatment with 131I, since 97% of patients after 2000 received 131I. Patients who received postoperative 131I experienced an improved PFS compared with patients treated by surgery alone. However, comparison of these treatment approaches is limited as some patients treated with surgery alone at our institution were not evaluated at the Mallinckrodt Institute of Radiology and were not included in analysis.
There was a noted difference in the time of recurrence based on treatment with 131I (Fig. 2). Although patients treated with postoperative radioactive iodine were at a decreased risk of relapse, the risk of failure during the first 5–10 years of follow-up was very similar between the treatment groups. The difference in risk of recurrence reflects the greater likelihood of late relapse in patients initially treated with surgery alone. There was only one failure after 10 years in the group of patients treated with radioactive iodine. In contrast, 25% of the failures in patients who did not receive initial 131I therapy occurred after 20 years. This finding may be the result of obtaining routine whole-body 131I scintigraphy in patients who underwent postoperative radioactive iodine therapy. In the patients treated with surgery alone, only one patient was followed with whole-body 131I scintigraphy prior to recurrence. However, 90% of patients treated with radioactive iodine underwent at least one 131I scan in the follow-up setting. Therefore, these patients were more likely to receive repeat radioactive iodine therapy for persistent disease and more likely to demonstrate subsequent negative 131I results, leading to a reduced risk of recurrence decades later.
Given the risk of recurrence many years after diagnosis, long-term follow-up and surveillance are important for these patients. However, what constitutes appropriate and cost-effective follow-up of these patients remains controversial. This is especially true for younger children for whom clinical data are even more limited. Regarding our cohort, it is important to note that the majority of our patients (70%) were over the age of 15 years. Our data suggest that patients treated with surgery alone can experience recurrent disease at 20 and even 30 years after initial therapy. This leads to the desire to develop follow-up testing that can help further delineate risk of recurrence. In conjunction with adequate suppression of TSH, measurement of thyroglobulin levels, and physical examination, our practice includes the use of whole-body 131I scintigraphy in the follow-up setting. Previous data from our institution have shown the predictive value of whole-body 131I scintigraphy (16). In 76 patients between the ages of 12 and 74 years, whole-body 131I scintigraphy was performed at years 1 and 2 and then every 3–5 years after primary treatment for their disease. There was a lower predictive value for relapse-free survival after a single negative scan compared to that after two negative scans (91% versus 97%, p=0.0197). In our current pediatric cohort, patients with persistently positive scans are at significant risk of progression. However, in patients with three consecutive negative scans no recurrences were observed.
Our current follow-up regimen consists of yearly whole-body 131I scintigraphy until two negative studies are obtained. Patients are then followed by yearly physical examination and serum thyroglobulin measurements with whole-body 131I scintigraphy repeated in 3–5 years. Alternatively, current recommendations suggest that patients are followed with routine serum thyroglobulin and neck ultrasonography with whole-body 131I scintigraphy reserved for those patients with abnormal serum thyroglobulin levels.
Optimal duration of complete suppression of TSH for these patients is unknown. Medical compliance, especially in adolescents, can be a problem with potential to increase risk of recurrence. However, concerns have been raised about the long-term effects of high levels of thyroid hormone in children because of effects on growth and learning ability (7). Further research on the effects of subclinical hyperthyroidism is needed.
Our data demonstrate excellent overall survival even for those patients with recurrent disease. This is in contrast to adult patients over the age of 45 in whom recurrence is often associated with poor survival (17). For those patients who developed recurrent disease, the majority were treated with 131I, with or without additional surgery. Pediatric patients tend to present with more advanced disease and for this reason, the majority of patients treated at our institution have postoperative 131I therapy. Development of recurrent disease more than 25 years after diagnosis was seen in patients treated with surgery alone and demonstrates the importance of long-term follow-up. Our clinical practice incorporates serial imaging with whole-body 131I scintigraphy as we observed no recurrences after three consecutive negative scans.
Footnotes
Author Disclosure Statement
No competing financial interests exist.