
Abstract
Background:
The current systems of healthcare delivery in the United States suffer from problems that often leave patients with inadequate quality of care. In their report entitled “Crossing the Quality Chasm,” the Institute of Medicine (IOM) identified reasons for poor and/or inconsistent quality of healthcare delivery and provided recommendations to improve it. The purpose of this review is to describe features of an innovative web-based program called the Thyroid Cancer Care Collaborative (TCCC) and see how it addresses IOM recommendations to improve the quality of healthcare delivery.
Summary:
The TCCC addresses the three actionable IOM recommendations directed at healthcare organizations and clinicians to redesign the care process. It does so by exploiting information technology (IT) in ways suggested by the IOM, and it fits within a set of 10 rules provided by the IOM. Some features of the TCCC include: (i) automated disease staging based on three validated scoring systems; (ii) highly illustrated educational videos on all aspects of thyroid cancer care; (iii) personalized clinical decision-making modules for clinicians and physicians; (iv) portability of data to share among treating physicians; (v) virtual tumor boards, “ask the expert,” and frequently asked questions modules; (vi) physician workflow integration; and (vii) data for comprehensive analysis to answer difficult questions in thyroid cancer management.
Conclusion:
The TCCC has the potential to improve thyroid cancer care delivery and offers several benefits to patients, clinicians, and researchers. The TCCC is a valuable example of how IOM initiatives can improve the healthcare system.
Introduction
Q
The current systems of healthcare delivery in the United States suffer from a number of major problems that leave patients with inconsistent and, in many cases, poor quality healthcare. In most cases, poor quality care occurs because of fundamental shortcomings in the organization of care, not because of failures in goodwill or effort (3).
In their landmark report entitled “Crossing the Quality Chasm: A New Health System for the 21st Century,” the Institute of Medicine (IOM) analyzed the state of the U.S. healthcare system, identified four fundamental reasons for poor and/or inconsistent quality of care, and provided 13 recommendations by which to improve it (3). It is remarkable how applicable the IOM analysis is to the specific case of thyroid cancer. Thyroid cancer has been identified as one of seven cancer types that have increased in incidence over the past decade (4), and its requirement for lifelong patient surveillance poses a challenge for both the patient and the overburdened healthcare system.
Herein, we describe an innovative web-based program called the Thyroid Cancer Care Collaborative (TCCC) created by key opinion leaders in thyroid cancer from across the United States with the aim of improving the quality of thyroid cancer care. The TCCC was designed and developed to be a comprehensive online program for patients, clinicians, and researchers to report and store all data related to a patient's thyroid cancer care. The TCCC is an implementation tool, not a clinical practice guideline (CPG), clinical algorithm, or other bona fide white paper. The TCCC meets the strictest standards for compliance with the Health Insurance Portability and Accountability Act (HIPAA). In addition to being an online repository of clinical information, the TCCC provides education and evidence-based clinical decision-making support services to patients and physicians within the framework of both the American Thyroid Association (ATA) and National Comprehensive Cancer Network (NCCN) CPGs for thyroid cancer (5,6). The TCCC also promises to serve as a valuable resource for large-scale clinical research, which is vital for making progress in the management of thyroid cancer.
The objectives of this paper are to use the IOM conclusions to discuss why we often have poor quality thyroid cancer care, describe the TCCC, and show how it uses information technology (IT) to improve potentially the quality of care, and see how the TCCC addresses the recommendations made by the IOM to improve the quality of healthcare delivery.
Review
Why do we have inadequate quality in thyroid cancer care delivery?
The IOM identified four fundamental reasons for inadequate quality of healthcare in the United States. While these IOM conclusions relate to the United States healthcare system in general, they are remarkably applicable to the specific case of comprehensive thyroid cancer care management.
1. The growing complexity of science and technology
Over the past few decades, there has been an explosion in basic science and epidemiologic information in all fields of healthcare (7). Thyroid cancer is certainly no exception to this trend; the number of PubMed indexed articles on the phrase “thyroid cancer” has steadily increased every year from 630 in 1982 to more than 2700 in 2012 (Fig. 1).
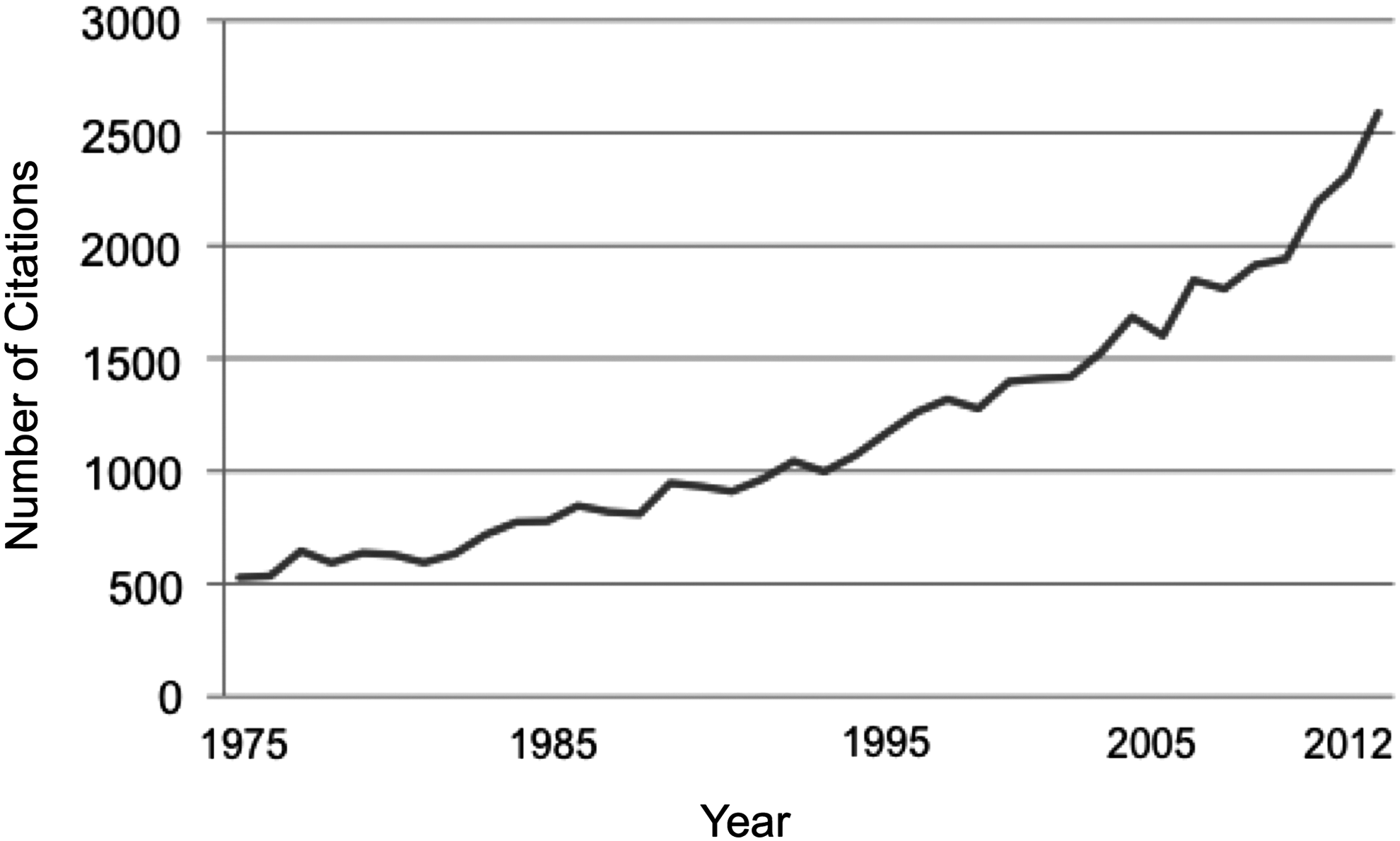
Number of PubMed indexed citations on the term “Thyroid Cancer” from 1975 to 2012 is evidence of the quickly and consistently expanding knowledge base in the science of thyroid cancer. The difficulty in synthesizing and applying the growing complexity of science and technology is one of four Institute of Medicine (IOM) reasons for poor quality healthcare delivery.
As the IOM explicates, an unaided human cannot act effectively on this huge volume of clinically relevant scientific literature and retain all of the information necessary for sound, evidence-based practice. So, how can we apply the latest evidence to every patient every time and continuously analyze data from thyroid cancer patients across the country treated in different settings over a long period of time to improve our understanding of effective practices?
One option would be to shift the care of all thyroid cancer patients to a select number of regional academic medical centers, where subspecialists presumably keep abreast of the latest literature and have the patient volume to support a comprehensive program. However, the staggering number of patients newly diagnosed with thyroid cancer in the United States (currently estimated at more than 60,000 new cases per year for 2013) (8) is a logistical and economic obstacle to this approach. Furthermore, divergent institutional cultures and infrastructural constraints have presently deterred effective interinstitutional collaboration within our healthcare system, conferring a rational pessimism that this option is viable. Another option is to bring durable white paper instruments, such as CPGs and clinical algorithms, to point-of-service of practitioners who treat thyroid cancer. Unfortunately, despite the best efforts of sponsoring professional societies (e.g., the ATA, the American Association of Clinical Endocrinologists, the NCCN), implementation of CPGs remains an overt shortcoming. Thus, the paradigm of standardized care can remain, but to be effective, it must include an actual implementation tool.
2. An increase in the number of patients with chronic conditions
Thyroid cancer is not self-limiting, and the consequences of treatment and monitoring for recurrence lasts longer than three months. Therefore, thyroid cancer can be considered a chronic condition. Just as the estimated number of Americans with one or more chronic conditions has grown at an alarming rate over the past 20 years, so too has the number of patients diagnosed with thyroid cancer. Thyroid cancer has been identified as one of seven cancer types that have increased in incidence over the past decade (4), with incidence rates steadily increasing from 4.9 per 100,000 in 1975 to 13 per 100,000 in 2008 (Fig. 2) (9). The reason for this steady increase cannot be explained completely by earlier and more frequent detection (10).
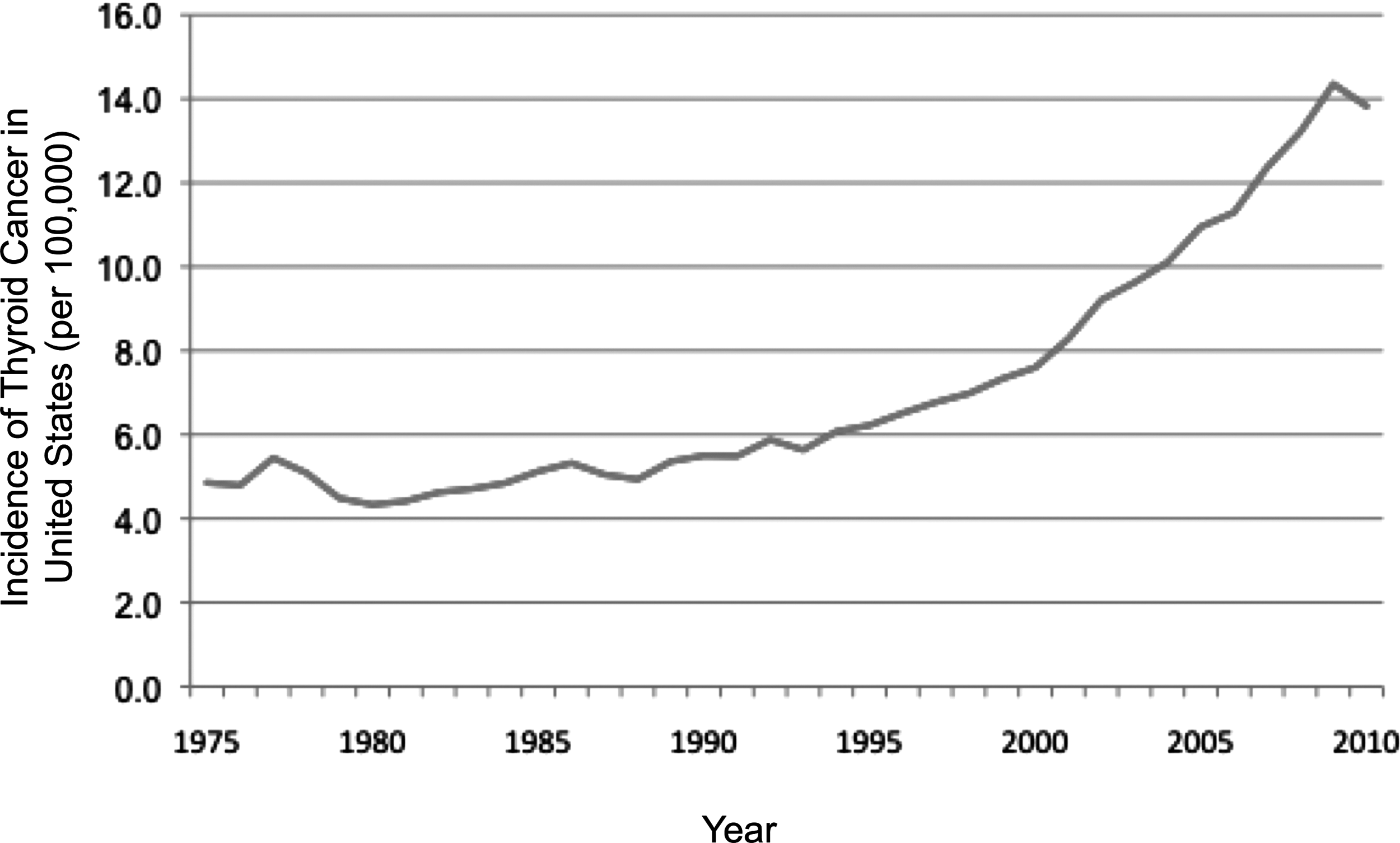
Surveillance, Epidemiology and End Results data showing incidence of thyroid cancer in the United States over time (per 100,000). 9
By almost all definitions, thyroid cancer can be considered a chronic condition. The increase in chronic conditions has been identified as another reason for poor and/or inconsistent quality of healthcare delivery. There are a number of reasons as to why achieving consistent high-quality care and long-term longitudinal follow-up of individual patients with chronic conditions is challenging. First, in contrast to most acute illnesses, high-quality care of chronic conditions requires collaboration between multiple practitioners and continual follow-up over decades. Second, early changes in the status of a chronic condition does not typically manifest with obvious signs and symptoms. Third, over time, patients move locations, change insurance, and/or change doctors. Finally, data are accumulated at various service points with no central data repository.
As with other chronic conditions, there is a tendency to reduce surveillance of thyroid cancer over time following initial treatment. Notwithstanding the low lethality nature of thyroid cancer in the majority of patients, overly complacent follow-up intervals, poor communication within treatment teams, and inadequate management of consequences of treatment (e.g., iatrogenic hypothyroidism) may lead to preventable adverse events over long periods of time. Furthermore, the risk of developing recurrent disease continues throughout a patient's life. Based on long-term follow-up of historical cohorts, even patients with early stage disease can recur as late as 30 years after initial therapy and be associated with significant morbidity (11,12). This makes it imperative that surveillance strategies for thyroid cancer be appropriately tailored for individual risks and then maintained for suitably prolonged periods of time. Routine alerts and other prompts for patients and clinicians must be incorporated into any quality improvement protocol.
3. A poorly organized delivery system
Numerous studies in healthcare have concluded that higher volume is associated with better outcomes (13 –16), but why this occurs is still speculative. It is possible that practitioners and organizations that provide high volume care in specific fields have in place more effective processes, better methods for incorporating knowledge into practice, superior skill, effective multidisciplinary teams, and access to specialized resources. It may not be possible for a practitioner who sees only a handful of thyroid cancer patients each month to establish processes, create consistent teams, and incorporate the latest knowledge quickly and efficiently to every patient, every time.
For the majority of thyroid cancer practitioners in the United States, the communication process chain shown in Figure 3A is probably all too familiar. Telephone calls, faxes, and e-mails go back and forth, office to office, leaving patients and practitioners frustrated. Also, this results in delays in treatment and, in some cases, treatment decisions that are made with an excess of incomplete information. Furthermore, these communications are frequently done in a non-HIPAA compliant manner, and require that the patient be responsible for maintaining their records for dissemination to current and potentially future treating physicians. Consistent with this observation, the IOM observed that physician groups operate independently, often providing care without the benefit of sufficient information on the patient's condition or services provided in other settings.
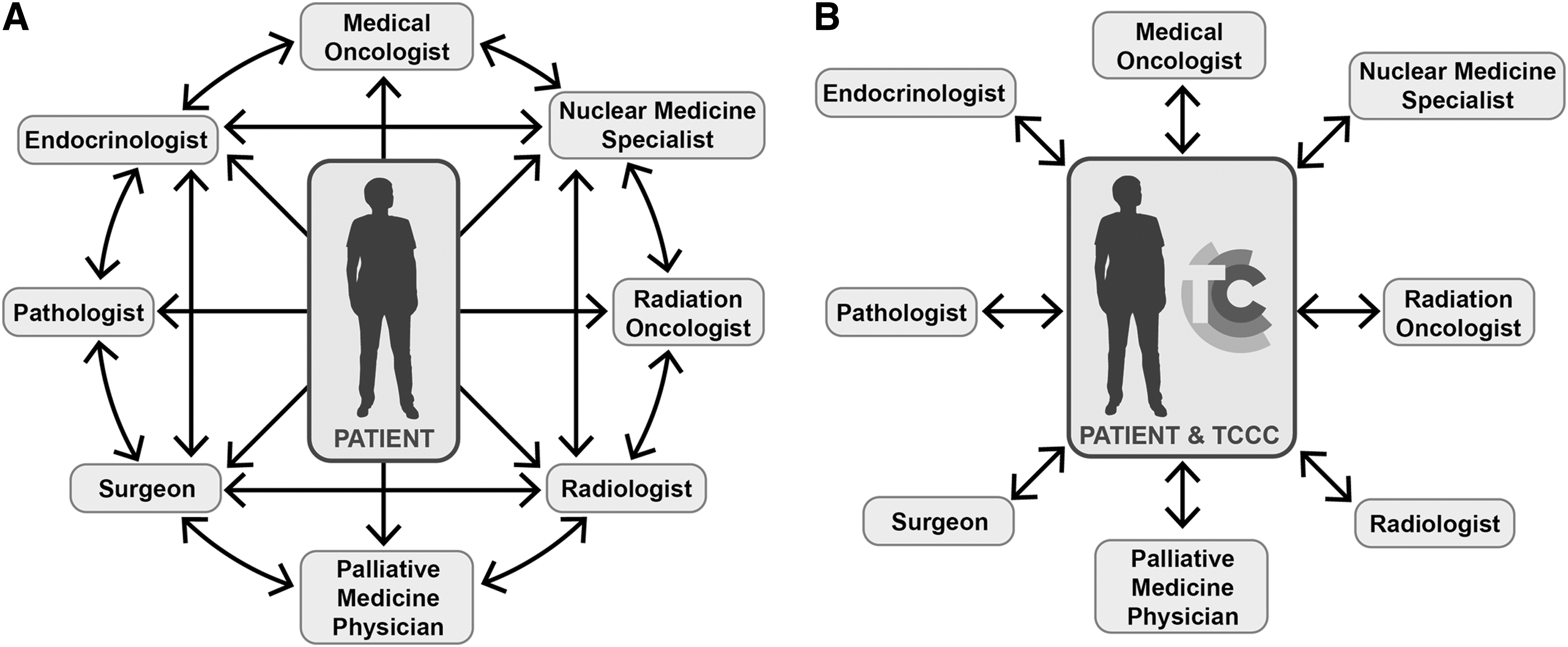
The Thyroid Cancer Care Collaborative (TCCC) will change patient and provider communication from
4. Constraints on exploiting the revolution in IT
Surely, every practitioner who has been frustrated with their health system has dreamed of ways that IT could improve their practice. Unfortunately, there are enormous barriers to entry for IT initiatives, making it difficult to create new applications and facilitate the adoption of even highly successful pioneering applications. The IOM identified technical, organizational, and policy challenges as factors limiting better exploitation of IT in healthcare.
Technical challenges include ensuring the security of personally identifiable information, authenticating data sources, and making tools available for efficiently locating information. Organizational challenges include taking advantage of new standards in communication languages amongst electronic medical records (EMRs) to allow seamless data flow from a variety of health systems' databases to populate data fields accurately. Policy challenges such as finding agreements between providers, payers, and service delivery organizations plague most innovative ideas in healthcare quality improvement.
Addressing problems in quality: the TCCC
One of the major conclusions of the IOM committee was that to initiate change, the healthcare system must develop care processes for conditions that afflict many people. To that end, three years ago, we embarked on an ambitious project to improve the quality of care in one of the most rapidly increasing chronic malignant conditions in the United States—thyroid cancer. With the resources afforded to a nonprofit foundation, independent of any individual practice or medical institution, we assembled a multidisciplinary team of key opinion leaders in thyroid cancer care, and created an online program—the TCCC.
Our mission was to create an innovative program that would improve the quality of thyroid cancer care now and into the future. Our main goals were to: • enhance and facilitate the connectivity of clinicians involved in the care of a particular patient with thyroid cancer; • improve the efficiency of physicians and their support staff; • provide portable information for patients and their physicians in a HIPAA-compliant manner; • empower patients as stakeholders by improving their understanding of the disease and the decisions being made in their care; • create a robust database to support large-scale clinical research; and • develop a cost-effective disease management tool to improve the quality of care.
The TCCC is a patient-centered web-based relational database and information program that integrates an individual's thyroid cancer data into a user-friendly centralized data repository. The database is designed with a simple user interface with separate modules that reflect the various points of care. These include initial presentation, imaging, surgical management, postoperative hospital course, surgical follow-up, pathology and staging, laboratory results, nuclear medicine, post-treatment surveillance, and change in health status.
Substantial investment was made to ensure the TCCC meets all HIPAA guidelines in terms of data security. All data are stored in a HIPAA-compliant hosting facility in an encrypted database, and the program enforces site-wide security (both at the server and browser level) ensuring that no unauthorized users have access to patient data. Furthermore, clinicians may only enter data on patients who have signed an informed consent to be a part of the TCCC, and only clinicians that are part of the care team explicitly chosen by the patient have access to that specific patient's data.
Data entry is performed by the physician at the point of care into the web-based program in the specific module in which they are involved. For example, following an operation, the surgeon would complete the “Surgical Management” module, which takes less than two minutes to complete and will autogenerate a narrative operative report that meets all ATA guidelines for high-quality operative reporting in thyroid cancer (17). For office visits, detailed and highly illustrated patient education and informed consent videos (with the physician available to supplement information and answer questions) will save the physician time and provide an opportunity to enter the specific data points related to their encounter in a rapid point-and-click system. This point-of-service data entry will improve the quality and completeness of data available for research, which is a known disadvantage of retrospective data abstraction methods used in current cancer databases. Accuracy of data entry is high because data are entered at the point of service by the clinical team, automatic alerts are generated for outlying data, and data are immediately available for review by all practitioners involved in the care of the patient. Integration of the TCCC into provider EMRs using a universal language is in active development.
The TCCC provides clinicians with the following services: • instantaneous access to and enhanced communication of results of imaging, laboratory, pathology, and procedural notes related to their patients' diseases; • automated disease staging for mortality based on three validated scoring systems (American Joint Commission on Cancer, AMES, and MACIS) (18
–20); • automated disease staging for recurrence based on the ATA three-tiered scoring system (6); • informed consent videos related to the most common procedures in the treatment of thyroid nodules and thyroid cancer; • patient-personalized clinical decision-making modules (CDMMs) that bring the latest treatment recommendations to point of service delivery for each patient, allowing the aggressiveness of the treatment to be appropriately gauged to the aggressiveness of the individual's clinical condition; • patient disease summary information that is immediately available when the physician logs on to review a specific patient's profile; and • enhanced, facilitated, and time-saving connectivity among treating physicians. The TCCC provides patients with the following services: • portable data related to their thyroid cancer care that can be shared with new physicians; • highly illustrated and easy to understand educational videos on all aspects of thyroid nodules and thyroid cancer, written by leading experts in the field; • access to the same CDMMs as physicians to improve understanding of recommendations being made in their treatment and follow-up; and • availability of “virtual tumor boards,” “ask the expert,” and “frequently asked questions” modules.
For researchers, the TCCC is a repository of detailed information on every aspect of patients' diseases in an easily searchable format. The TCCC has great potential for large-scale data analyses on thyroid cancer because it can follow individual patients throughout the country, over time, with prospectively gathered data that can be easily queried. By creating a database that automatically accumulates data as part of the physician's normal workflow, the likelihood of maintaining replete data sets is greatly enhanced. Research is a cornerstone of the TCCC, and is part of the informed consent presented to all patients at the initial visit. While individual physicians have the ability to query aggregate data about their own patients, multiple-provider or multi-institution data queries using anonymous data require review and approval by a multidisciplinary research committee and either an independent or institution-linked ethics review board. The infrastructure for data queries is otherwise similar to current anonymous multi-institution cancer databases. As more data are collected and analyzed, we hope to reduce the number of recommendations in CPGs and clinical algorithms that are based on expert opinion alone.
How does the TCCC utilize IT to improve quality?
The IOM report said that IT should be a major contributor to improving the delivery of healthcare. The committee provided five ways to exploit IT maximally for quality improvement: (i) access to the medical knowledge base; (ii) computer-aided decision support systems; (iii) collection and sharing of information; (iv) reduction in errors; and (v) enhanced patient and clinician communication.
The TCCC utilizes IT to implement these five initiatives in a comprehensive way. First, the web-based TCCC is continually updated. Therefore, both clinicians and patients have unlimited access to current thyroid cancer information and clinical evidence. Medical information is provided in many formats, including more than 40 professionally narrated and illustrated patient education videos. Patient education videos have been shown to increase patient understanding (21,22), improve patient questioning (21), be a preferred method of disease education for patients (23), reduce clinician and staff education time, and offer a standardized approach to informed consent with the physician available to supplement information and answer questions, thereby offering the possibility of decreased physician liability (24). Using the list of available videos, providers can select which videos they want their patients to watch by creating a playlist. See Table 1 for complete list of Patient Education Video Modules in the TCCC.
These are highly illustrated videos, written by key opinion leaders in thyroid cancer care across the country, and presented in an unbiased fashion.
FNA, fine-needle aspiration; RAI, radioactive iodine; rTSH, recombinant thyroid stimulating hormone.
Second, the TCCC feeds all information from a patient's diagnostic and treatment history directly into a computer-aided decision support system for patients and physicians. It uses the latest evidence not only to alert practitioners when a clinical decision needs to be made, but also to outline the different options for managing a specific decision. The CDMMs are embedded into the system, and augment the physicians' knowledge and experience to apply the latest evidence base consistently. This is particularly important for community physicians or those who see thyroid cancer patients infrequently. The CDMMs that have been created include: • need for remnant ablation; • decision to perform a completion thyroidectomy; • thyrotropin (TSH) suppression therapy: determining target TSH levels; • routine surveillance with labs and imaging based on ATA risk of recurrence; • management of recurrent/persistent metastatic lymph nodes; • restratification of patients based on response to therapy and surveillance recommendations at 24 months; • decision making for external beam radiotherapy; • decision making to retreat with radioactive iodine; • decision to obtain a positron emission tomography/computed tomography scan; • decision making in referral for systemic therapy.
Third, the TCCC automatically feeds data into CDMMs. In addition, all providers are informed when new information or data are available for a patient. Furthermore, the system has all the information to help patients participate in virtual tumor boards and enroll in clinical trials. The TCCC imaging module collects information in such a way as to provide a clear, graphical portrayal of thyroid nodules that are sequentially imaged over time.
Fourth, the TCCC uses technology to minimize errors by ensuring all physicians have more data upon which to make treatment decisions, and by standardizing many treatment decisions based on the best available evidence using CDMMs. Also, automatic patient and provider alerts are sent when a surveillance test or follow-up appointment is due, when a clinical decision needs to be made, and when there is a change in health status that might impact treatment decisions such as level of thyroid suppression. Finally, the system is programmed such that outlying data points are automatically identified and physicians are alerted, thereby improving safety and ensuring accuracy of data entry.
Fifth, the TCCC aims to change the way clinicians communicate with each other by capitalizing on the power of the Internet for immediate, yet HIPAA-compliant, dissemination of information across practice sites and institutions, bypassing the need for shared medical records (Fig. 3B).
How does the TCCC meet the IOM's recommendations for quality improvement?
The IOM report stated that improved performance will require new system designs, and that such systems must serve the needs of patients (to ensure that they are fully informed, retain control, and participate in care delivery whenever possible), facilitate the application of current scientific knowledge, and give clinicians tools to deliver consistent and safe evidence-based care (3).
Of the 13 recommendations made by the IOM to improve the quality of healthcare delivery in the United States, three actionable recommendations were not directed not national agencies or payment and funding sources, but appeared as direct challenges to purchasers, healthcare organizations, and clinicians to redesign healthcare processes (Table 2) (3).
The full text of these recommendations is available in the report. 3 Recommendations in bold represent those that can be seen as a challenge to purchasers, healthcare organizations, and clinicians.
AHRQ, Agency for Healthcare Research and Quality; HHS, Department of Health and Human Services; NQF, National Quality Forum.
In Recommendation 1, the IOM asked these stakeholders to make it their purpose to reduce the burden of illness and improve the health and functioning of our citizens. This was indeed our purpose in the design of the TCCC.
In Recommendation 2, the IOM gave six major aims with regard to healthcare delivery in order to achieve quality improvement. Specifically, they wanted healthcare delivery to be: • Efficient: The TCCC aims to reduce duplicated tests and will result in high-quality data collection by way of synoptic reporting in imaging, pathology, and surgical procedures. • Timely: The TCCC aims to reduce delays in giving and receiving care by eliminating efforts in gathering results from different points of care in disparate health delivery systems. • Effective: The TCCC aims to avoid underuse, overuse, and misuse of healthcare services by providing recommendations based on the best available scientific knowledge. • Safe: The TCCC aims to promote safety by avoiding injuries to patients through a decrease in errors of data collection and treatment recommendations. • Patient-centered: Because patients have access to information, education, and CDMMs, the TCCC aims to provide care that is respectful of patient preferences and includes them in decisions related to their care. Also, the CDMMs use data specific to the patient at hand to provide customized treatment and surveillance recommendations, taking into account an ongoing assessment of response to therapy. • Equitable: The services offered by the TCCC are independent of personal characteristics such as race/ethnicity, geographic location, sex, and socioeconomic status. By empowering patients with quality information in one trusted location on the Internet, the TCCC aims to improve the information flow to patients who might otherwise have restricted access to expert physicians. By giving patients access to “ask the experts” and “virtual tumor boards,” as well as exposure to less common therapies such as external beam radiotherapy and an awareness of open clinical trials, the TCCC can bring tertiary-level care to people all over the country.
In Recommendation 4, the IOM provided a set of 10 rules upon which to base a redesign of healthcare processes. Table 3 summarizes many of the key features of the TCCC, and shows how the program follows the IOM rules (3,25).
CDMMs, Clinical Decision Making Modules; HIPAA, Health Information and Portability and Accountability Act; PET-CT, positron emission tomography/computed tomography.
Summary
The TCCC is an innovative program that utilizes IT to redesign the system of providing care to patients with thyroid cancer. We believe it offers significant quality advantages to patients, practitioners, and researchers involved with thyroid cancer. The TCCC offers care that is patient-centered, efficient, timely, effective, safe, equitable, and cost effective. It addresses the three recommendations and challenges made directly to clinicians by the IOM in their landmark report on quality in healthcare, and thus fits squarely in a larger and overhauled healthcare delivery system. Furthermore, the TCCC is a valuable example of how IOM initiatives can improve the healthcare system.
Conclusion
Three main goals remain with the TCCC. First, through a patient- and clinician-driven approach, we hope to increase participation and penetration steadily into the workflow of physicians who treat patients with thyroid cancer across the United States. Second, we continue to strive to increase the interoperability of the TCCC with existing commonly used electronic medical records to reduce or eliminate the duplication of physician effort in data entry. Third, we would like to open data extraction to researchers to perform comparative effectiveness research and epidemiological analysis to answer important questions to improve the treatment of thyroid cancer. A demonstration of the TCCC can be found online at
Footnotes
Acknowledgment
The authors acknowledge administrative support from the Thyroid Head and Neck Cancer (THANC) Foundation.
Author Disclosure Statement
No competing financial interests exist.