
Abstract
Background:
Spinal metastases (SMs) due to thyroid cancer (TC) are associated with significantly reduced quality of life. The goal of this study is to analyze the clinical manifestations, presentation, and treatments of TC SMs, and to describe specific features of SMs associated with different TC types.
Patients and Methods:
A retrospective analysis of 202 TC SM patients treated at Medstar Washington Hospital Center (37) and collected from the literature (165) was performed.
Results:
The mean age of patients with SMs was 56.9±14.7 years, and the female-to-male ratio was 2.1:1. Of all patients, 29% (28% of follicular thyroid cancer [FTC] and 37% of papillary thyroid cancer [PTC]) had SMs only. Twenty-nine percent of all patients and 54% of patients with single-site SMs had neither bone non-SMs nor solid organ metastases at the time of presentation. Thirty-five percent of patients had SMs as an initial presentation of TC. TC patients presenting with SMs had a lower rate of other bone and visceral involvement compared with patients whose SMs were diagnosed at the time of thyroid surgery or during follow-up (p<0.05). SMs were more often the initial manifestation of FTC (41% vs. 24%), while PTC SMs were more commonly diagnosed after TC diagnosis (76% vs. 59%; p<0.05). PTC SMs were more frequently diagnosed as synchronous (63% vs. 36% in FTC) versus FTC SMs that developed as metachronous metastases (64% vs. 37% in PTC; p<0.01). All FTC SMs developed within 82 (0–372) months and all PTC SMs within 35 (0–144) months (p<0.01). In FTC SMs as TC manifestation, solid organ metastases involvement was less common than in FTC SMs that were found after TC diagnosis (34% vs. 67%; p<0.01); multisite FTC SMs compared to solitary FTC SMs were associated with the development of other bone nonspinal metastases (82% vs. 30%; p<0.01) and solitary organ metastases (65% vs. 41%; p<0.01). These correlations were not observed in PTC SMs. FTC patients often had neural structure compression (myelopathy/radiculopathy; 72% vs. 36% in PTC), while PTC patients frequently were asymptomatic (38% vs. 5% in FTC; p<0.01). FTC SMs more commonly were 131I-avid (p<0.01). FTC patients required surgery more frequently (72% vs. 55% in PTC; p<0.05).
Conclusions:
Our study reveals that a significant part of TC SMs patients have solitary spinal involvement at the time of presentation and may be considered for aggressive treatment with the intention to improve quality of life and survival. FTC SMs and PTC SMs appear to have distinct presentations, behavior, and treatment modalities, and should be categorized separately for treatment and follow-up planning.
Introduction
I
Spinal metastases (SM) are the most common site of TC bone metastases, developing in more than 3% of patients with TC (4). Thyroid SMs differ from the SMs of other primary cancers. Thyroid SMs have the most favorable prognosis, with an average survival of 33.1 months compared to an approximately seven-month survival for patients with SM from primary tumors other than TC (2,5,6). Despite the relatively favorable prognosis, patients with thyroid SMs often have a significantly reduced quality of life, for example pain, neurological problems, and increased mortality (2,4). In most studies, SMs secondary to TC are analyzed within groups of patients with other primary tumors or TC bone metastases, making the singular clinical outcome of TC SMs difficult to assess. There is a lack of research addressing the specific features of SMs originating from different TC types. Most of the literature on TC SMs is based on small sample size publications, such as case reports, case series, or a subset of patients in larger groups of patients with different primary tumors where the numbers of patients with TC metastases is invariably low or SMs are a subset of bone metastases.
The aim of this study was to perform a comprehensive analysis of the clinical manifestations, presentation, and treatment of TC SMs, as well as to describe the specific features of SMs associated with different TC types. Therefore, we retrospectively analyzed 202 patients who suffered SMs secondary to TC, 37 of whom were treated at the Medstar Washington Hospital Center (WHC). The data of the remaining 165 patients were collected from previous publications.
Materials and Methods
We reviewed the Medstar WHC database and identified 37 patients with TC SMs. This study was approved by the Medstar WHC Institutional Review Board. We searched the following databases for studies on TC and SMs using all relevant keyword variations: PubMed, Cochrane Library, Web of Science, Google Scholar, and Science Direct. A total of 56 studies published from 1981 to 2012 were located and systematically analyzed (2,7 –61). Research completed more than 20 years ago was excluded from our study because the methods used at that time for diagnosis and treatment differ from the current approaches, for example computed tomography (CT) was not used for SMs in those days. As a result, data from 202 patients with SMs were collected and analyzed in the present study. Previously published patient data from the University of Groningen (Groningen, The Netherlands) and the Bergonié Institute (Bordeaux, France) published previously were updated, and important information was added for analysis by this study's co-authors (TL and FB).
An analysis of the literature identified two patterns of SMs: the initial presentation of TC as SMs (Group S; “spinal manifestation”), and SMs that were identified at the time or developed after TC diagnosis (Group T; “thyroid manifestation” of TC). According to the time interval from TC diagnosis to the detection of SMs, metastases were classified into two types: synchronous and metachronous. Synchronous metastases were identified as metastases that were apparent at the time of TC presentation or within six months following diagnosis, while metachronous metastases were defined as metastases that had developed more than six months after TC diagnosis.
Because selected manuscripts were published from various clinical departments and different aspects of the SMs were described with missing data and follow-up information, all analyses and calculations of particular characteristics were performed depending on the availability of details about the patients. Chi-square methods, the dispersing method (F), and the Student's method (t-test) were used for the statistical analysis of the cancer-related variables.
Results
General characteristics of thyroid cancer spinal metastases
Demography
Among the 202 patients selected for the study, 41% were males and 59% were female. The patients' mean age at the time of TC presentation was 56.9±14.7 years. In terms of the primary histological classification, 63% of the patients presented with follicular TC (FTC), 28% with papillary TC (PTC), 5% with medullary TC (MTC), 3% with Hürthle cell carcinoma (HCC), and 1% with anaplastic TC (ATC; Fig. 1). The status of the distant metastases other than SMs was available in for 142 patients: 37% had both bone non-SMs and solid organ metastases, 22% had other bone non-SMs, 12% had solid organ metastases, and 29% had neither bone non-SMs nor solid organ metastases. Single-site SMs were found in 49% of the patients, and 51% of the patients had multisite involvement (two or more vertebrae involved). Importantly, 54% of all the TC patients with single-site SMs did not have any other distant metastases. A summary of the patients' demographics, clinical features, histology, and treatments modalities is shown in Table 1. The mean follow-up was 42 months (0–191 months).
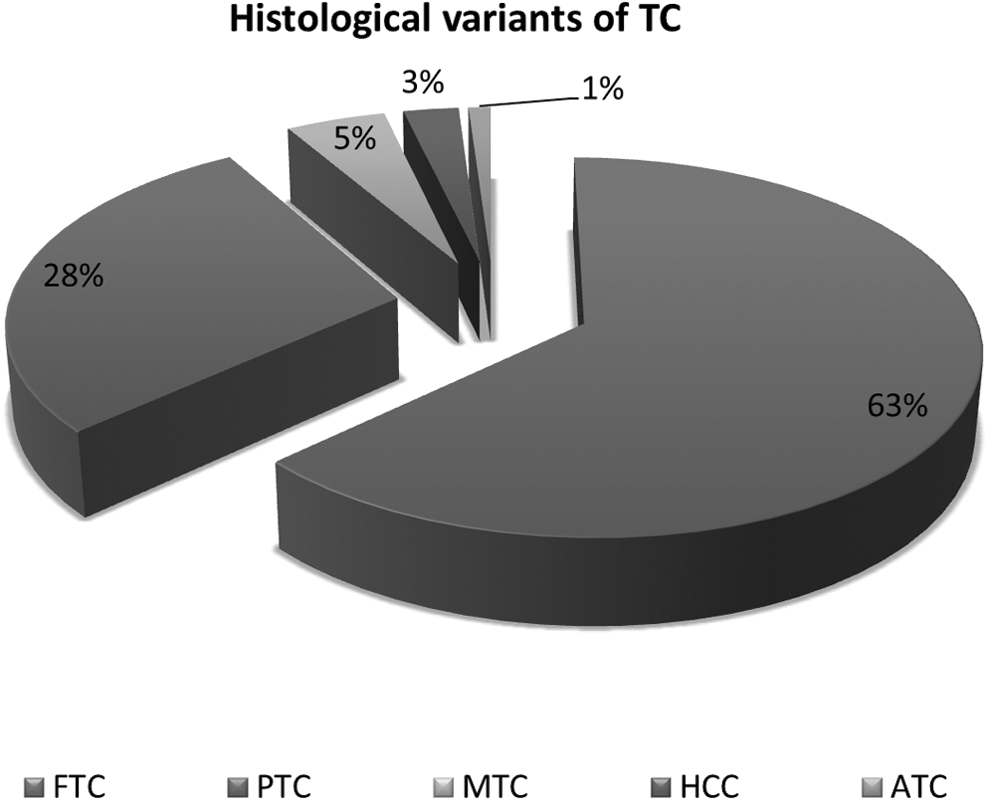
The primary histological classification of thyroid spinal metastases. One hundred and twenty (63%) patients had FTC, 54 (28%) had PTC, 9 (5%) with MTC, 6 (3%) had HCC, and 2 (1%) had ATC (11 patients had tumor of unknown histology).
Clinical presentation
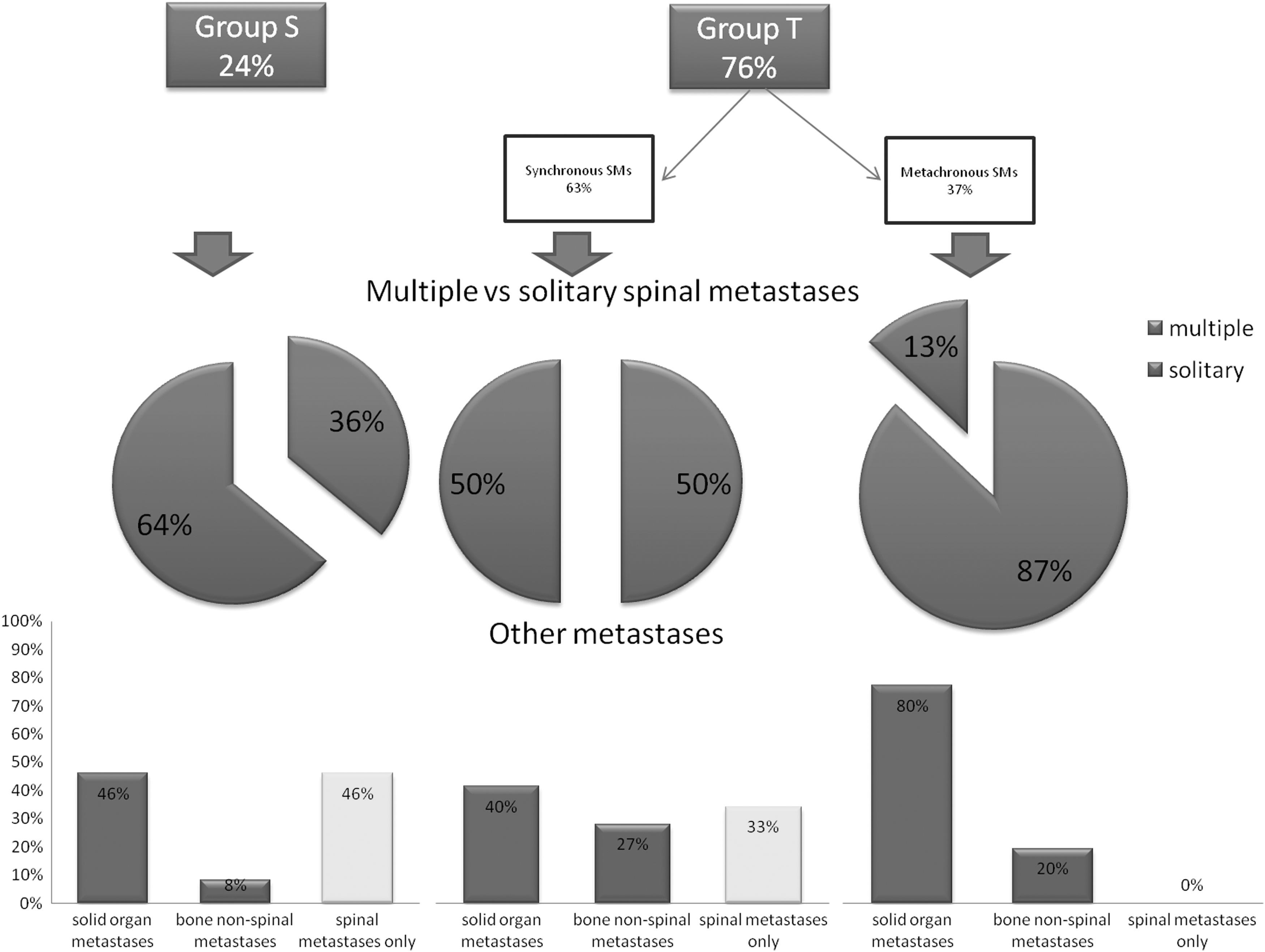
The initial presentation of TC as SMs (Group S) was found in 35% of the patients. SMs that were identified at the time of the initial diagnosis of TC or that developed after TC diagnosis (Group T) were evident in 65% of the patients (Fig. 2).

Schematic illustration of the presentation of spinal metastases secondary to thyroid carcinoma. In our study, about 35% of spinal metastases presented as an initial manifestation of thyroid cancer; 30% of the patients had synchronous metastases, and 35% had metachronous metastases. Follicular thyroid cancer was found to be more common in spinal metastases that manifested thyroid carcinoma, and as metachronous metastases, while papillary thyroid carcinoma was prevalent in synchronous metastases (p<0.05). Spinal metastases that manifested thyroid carcinoma had the highest incidence of solitary lesions (49%), while metachronous metastases had the lowest prevalence at 38%. Patients with spinal metastases that manifested thyroid carcinoma as compared with patients whose spinal metastases were diagnosed at the time of thyroid surgery or during follow-up had the lowest level of solid organ metastases (35.8%) and the highest level of isolated spinal metastases (38%), and 26.2% of the patients had spinal metastases and other bone nonspinal metastases. In total, 50% of the patients with metachronous spinal metastases had accompanying solitary organ metastases; 25% had concomitant bone nonspinal metastases, and only 25% of the patients with spinal metastases had no other distant metastases. The majority of the patients (80%) with metachronous spinal metastases had solitary organ metastases, only 10% of the patients had spinal metastases and other bone nonspinal metastases, and 10% of the patients had isolated spinal metastases (p<0.05).
TC with spinal manifestations (Group S)
Vertebral involvement can occur due to the direct spreading of TC (direct involvement) with a subsequent extension into the spinal canal, or as the indirect (hematogeneous/lymphogeneous) spreading of malignant cells. All three cases of direct spread of TC into the spinal canal occurred in patients with PTC. All had spinal cord compression and died soon after their neurological symptoms manifested.
TC with thyroid manifestations (Group T)
Synchronous metastases were found in 46% of patients in Group T (30% of all TC patients), and metachronous metastases were diagnosed in 54% of patients in Group T (35% of all TC patients). When Group S, Group T synchronous SMs, and Group T metachronous SMs were compared, bone non-SMs and solid organ metastases were less common in Group S and more prevalent in Group T metachronous SMs (p<0.05; Fig. 2).
Diagnosis of SMs
As many as 57% of the patients presented with symptoms of neuronal structure compression, including spinal cord compression (myelopathy with or without root compression) in 45% and root compression (radiculopathy) in only 12% of patients. Back pain was found to be an initial symptom in 28% of patients. The remaining 15% of patients were asymptomatic, and their metastases were found during routine evaluation at the time of the initial diagnosis or at the subsequent follow-up.
The patients were diagnosed with SMs by 131I whole body scan, CT, magnetic resonance imaging (MRI), or positron emission tomography (PET). The 131I uptake by SMs was analyzed in 82 patients. Affected vertebral lesions that could be distinguished from other spinal lesions and which had localization proven via CT and/or MRI were assessed. Overall, 180 lesions were evaluated. Of these, 58% were 131I avid, while 42% were negative.
Treatment of the primary TC
Of 151 patients, 131 (87%) underwent a total thyroidectomy upon TC diagnosis. Eleven (7%) patients initially underwent a hemithyroidectomy for a “benign thyroid tumor” and later underwent total thyroidectomy upon being diagnosed with TC due to the manifestation of SMs. Nine (6%) patients with SMs did not receive any thyroid surgery due to, for example, patient refusal or high operative risk. 131I ablation was performed in 94% of the patients with differentiated TC.
Treatment of the SMs
Information about the treatment for SMs in 183 of the TC patients was available for analysis. Of those, 67% received surgery, 24% nonsurgical treatment, 4% radiosurgery, and 5% of the patients did not undergo any of these therapies. Radical surgical treatment, that is, total removal of the metastatic lesions in the patients with single isolated SMs, was performed in 16 (13%) of the patients. Embolization was used in 72 cases (39%), with preoperative embolization before radical or palliative surgery in 55 (76%) of those patients. It was the only treatment in 17 (24%) patients. Radiotherapy was the leading treatment for the patients who received nonsurgical therapy; it was applied in 39 (87%) of 45 patients. Of the surgical patients, 48 (39%) also received external radiation.
Tumor type-specific data
FTC
Among the 120 patients with FTC, 66% were females and 34% were males. Their mean age was 56.7±14.4 years. Of those patients, 48% had solitary SMs and 52% multiple SMs. The distribution of the metastatic lesions followed the localization of the radiculomedullary arteries that supply the spinal cord (Fig. 3A and B). Patients with both bone non-SMs and solid organ metastases, as well as patients with bone non-SMs, were more common among the multisite SMs group. The patients who did not have solid organ metastases and bone non-SMs were more prevalent in the solitary SM group (p<0.01). Thus, multiple SMs of the FTC were associated with significant metastatic involvement of the solid organs and bones. The FTC Group S comprised 41% of the patients, and 59% of the patients were included in the FTC Group T (Fig. 4). The mean follow-up in this group was 50 months (0–191 months); 59 months for the patients with solitary SMs and 47 months for the patients with multiple PTC SMs.

Distribution of spinal metastases originated from follicular and papillary thyroid carcinomas.

Spinal metastases from follicular thyroid carcinoma. The initial presentation of follicular thyroid carcinoma as spinal metastases (Group S) was found in 45% of all the patients in our study. In this group, 49% of the patients had single-site spinal metastases, and 51% had multiple spinal metastases; a total of 29% of the patients had solid organ metastases, 29% had only bone nonspinal metastases, and 42% had neither bone nonspinal metastases nor solid organ metastases. Spinal metastases that were identified at the time or developed after TC diagnosis (Group T) comprised 55% of all the patients with follicular thyroid cancer. In this group, synchronous metastases were found in 36% of the patients: 53% of them had multiple spinal involvement, 50% had solid organ metastases, 30% had only bone nonspinal metastases, and 20% had neither bone nonspinal metastases nor solid organ metastases. Metachronous metastases were found in 64% of the patients in Group T. The majority of the patients (63%) had multilevel spinal involvement: 82% had solid organ metastases, only 9% had bone nonspinal metastases, and 9% had neither bone nonspinal metastases nor solid organ metastases.
FTC Group S
None of the FTC patients presented with direct expansion of their tumors to the spine. However, 49% of the patients had solitary SMs and 51% multiple lesions. Bone non-SMs were more common (p<0.05) in patients with multisite SMs compared to solitary SMs. There was a trend (p=0.67) for multisite SMs to be associated with solid organ metastases. Importantly, 68% of the patients with single-site SM in the FTC Group S did not have any other distant metastases.
FTC Group T
In Group T, 36% of the patients had synchronous metastases, and 64% of the patients developed metachronous metastases within 127.8±94.6 months (12–372 months) after TC was diagnosed. Solitary SMs were found in 47% of the patients, and 53% of the patients had multiple SMs. Patients with multiple SMs had a significantly higher risk of developing both bone non-SMs (p<0.01) and solid organ metastases (p<0.01). Of the patients with single-site SM in the FTC Group T, 38% did not have any other distant metastases.
FTC Group S versus FTC Group T
When we compared the FTC Group S with the FTC Group T, solid organ metastases were found to be more common in the latter (p<0.01). The development of bone non-SMs was not significantly different between the groups.
Appearance of distant FTC metastases
Among the 64 patients available for analysis, 52 (81%) patients had the first distant metastasis localized in the bones (including the spine). In nine (14%) patients, bone and solid organ metastases developed at the same time, and in three (5%) patients, distant metastases manifested with solid organ metastases. This means that, altogether, solid organ metastases were diagnosed as the first distant metastases in 19% of the patients, while 95% of the patients had bone metastases (Fig. 5).
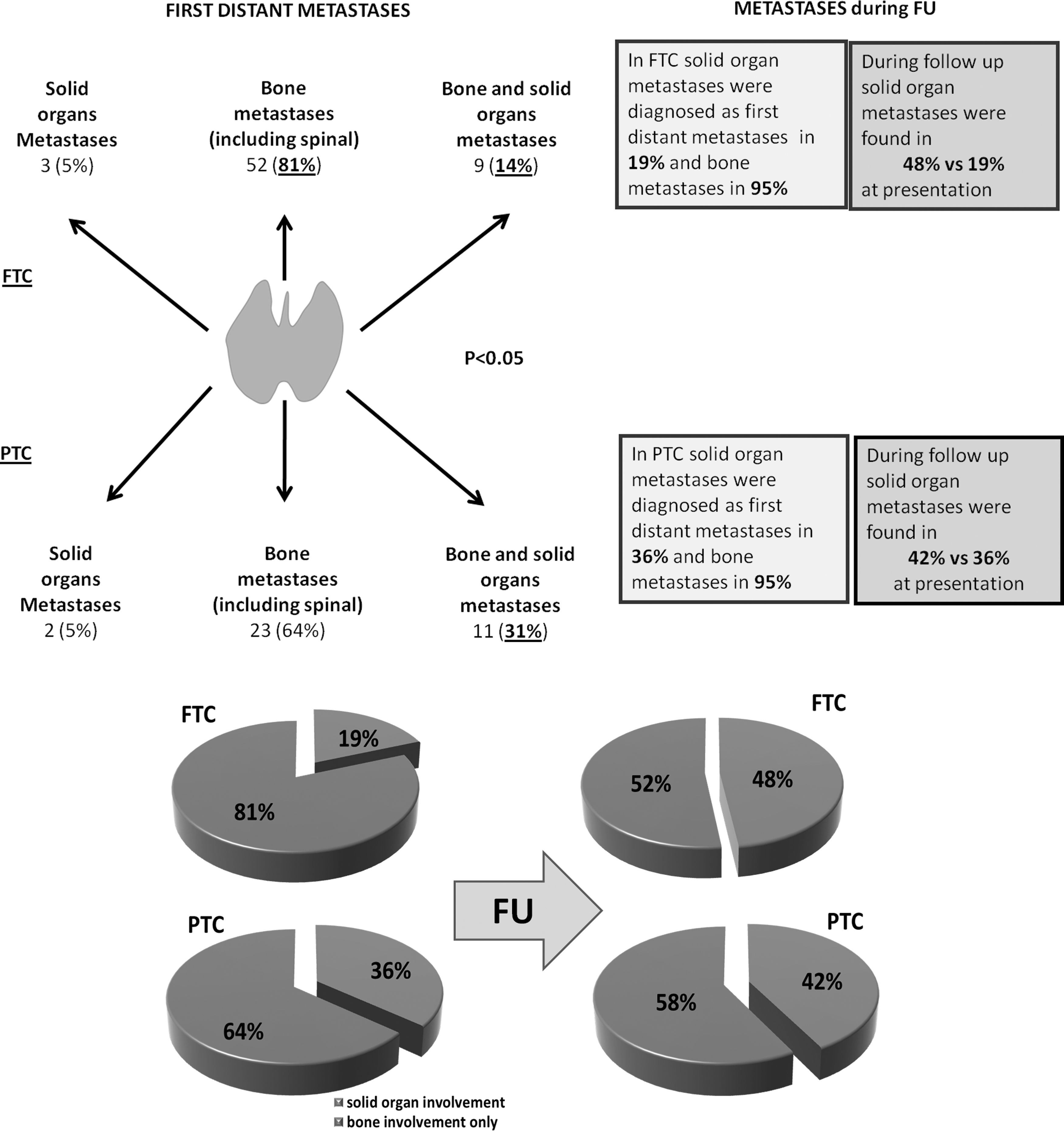
Schematic illustration of characteristics of spinal metastases due to the follicular thyroid cancer and papillary thyroid cancer. In follicular thyroid cancer, 81% of the patients had the first distant metastasis localized in the bones (including the spine); 14% of the patients had the initial distant metastases in bone and solid organs; and in 5% of the patients, the first distant metastases were found in solid organ. In other words, in follicular thyroid cancer, solid organ metastases were diagnosed as the first distant metastases in 19% of the patients, with a subsequent increase to 48% during follow-up, while 95% of the patients had bone metastases. Even though all the patients had thyroidectomy following the initial TC diagnosis, the number of solid organ metastases increased over time. Of the patients with papillary thyroid cancer, in 64% of the patients, the first distant metastasis in the bone; 31% of the patients had the initial metastases localized in the bone and solid organs; and in 5%, the first distant metastases were found in solid organ. This means that solid organ metastases as the first distant metastases were found in 36% patients, and this number progressed to 42%, while 95% of the patients had bone metastases. It seems that little if no solid metastatic progression was seen.
Our analysis revealed a group of patients who had undergone a hemithyroidectomy for a putative thyroid tumor but had developed SMs years later. It is speculated that those patients had minimally invasive FTC that was not diagnosed at the time of surgery. This group consisted of 10 patients, all of whom were females. They had a mean age of 36.4±0.4 years, which meant that they were younger than all the other FTC patients (p<0.001). These metastases also developed later (221.7±138 months) than the other FTC metachronous metastases (101.5±68.4 months; p<0.001). Upon diagnosis of SMs, all the patients underwent total thyroidectomies and radioiodine therapy.
Clinical presentation and treatment
The majority of the patients (72%) presented with symptoms of neuronal structure compression: either myelopathy (57%) or radiculopathy (15%). Back pain was the initial symptom in 23% of the patients. Only 5% of the patients were asymptomatic. In 66%, the SMs lesions were 131I avid, while in 34%, they were not. Surgery was performed for 72% of the patients, and nonsurgical treatments were provided for 18%. Radiosurgery was used for 2% of the patients, and 5% received no treatment.
PTC
Of the 54 patients with PTC, 55% were male and 45% female. The mean age was 57.8±13.9 years with a trend showing the males to be older than the females (61±10.0 years vs. 54.5±17 years respectively; p=0.066). Within the PTC group, 46% of the patients had solitary SMs with 54% having multiple SMs. All the PTC patients with solitary SMs were significantly older than those with multiple lesions (64±11.7 years vs. 51.4±14 years respectively; p<0.001). Among the patients with PTC solitary SMs, 53% did not have any other metastases. Only 24% of the PTC patients had SMs on presentation of TC (the PTC Group S), while the other 76% were found to have SMs at the time of TC diagnosis or after TC was diagnosed (the PTC Group T; Fig. 6). The mean follow-up for the PTC patients was 38 months (0–139 months), 34 months for the patients with solitary SMs, and 48 months for those with multiple PTC SMs.
Spinal metastases from the papillary thyroid carcinoma. The initial presentation of papillary thyroid carcinoma as spinal metastases (Group S) was found in 24% of all the patients. In this group, 64% of the patients had single-site metastases and 36% had multilevel spinal involvement; 46% of the patients had solid organ metastases, 8% had other bone nonspinal metastases, and 46% had neither bone nonspinal metastases nor solid organ metastases. The majority of the patients with papillary thyroid cancer (76%) constituted Group T, whose spinal metastases were found at the time or developed after TC diagnosis. In this group, synchronous metastases were found in 63% of the patients: half of them had multiple spinal involvement, 40% had solid organ metastases, 27% had other bone nonspinal metastases, and 33% had neither bone nonspinal metastases nor solid organ metastases. Metachroneous metastases were found in 37% of the patients of Group T. The majority of the patients in this group (87%) had multilevel spinal involvement, 80% had solid organ metastases, and only 20% had other bone nonspinal metastases.
PTC Group S
The mean age of the 10 patients in the PTC Group S was 63±14 years. There was no significant difference in the distribution of the bone non-SMs and solid organ metastases between the patients with solitary and multiple SMs. Three of the 10 patients had direct expansion of their tumors to the spine. Those three patients were significantly older than those in the PTC Group T (68±7.4 years vs. 55±15.3 years respectively; p=0.03). Importantly, 67% of the patients with single-site SMs in the PTC Group S did not have any other distant metastases.
PTC Group T
In PTC Group T, 76% of the patients were found to have SMs at the time of TC diagnosis or to have developed SMs after TC diagnosis. Synchronous SMs were found in 20 (63%) patients, and metachronous SMs were evident in 12 (37%) patients within 34 months (0.5–144 months) after TC surgery. Among the patients with single-site SMs in FTC Group T, 43% did not have any other distant metastases.
PTC Group S versus PTC Group T
There were no significant differences in the distribution of bone non-SMs and solid organ metastases between the patients of PTC Group S and PTC Group T.
Appearance of distant PTC metastases
Among the 36 patients available for analysis, 64% had initial distant bone metastases, 31% presented with bone and solid organ metastases at the same time, and 5% had initial solid organ metastases. This means that, altogether, solid organ metastases were diagnosed as first distant metastases in 36% of the patients, while 95% of the patients had bone metastases (Fig. 4).
Clinical presentation and treatments
A total of 28% of the patients presented with myelopathy (with or without radiculopathy), 9% with radiculopathy only, 25% of the patients had back pain as an initial symptom, and 38% of the patients were asymptomatic. Of the patients with PTC lesions, 43% were 131I avid, while 57% did not show an uptake of radioiodine. Information regarding treatment was available for 47 patients. Surgery was performed for 55% of the patients, nonsurgical treatments were provided for 28%, radiosurgery was used for 11% of the patients, and 6% did not receive any therapy.
FTC versus PTC
A comparative analysis of the patients with FTC and PTC revealed specific features (Table 2). Among the patients with FTC, females predominated (66%), while for PTC, males were in the majority (55%; p<0.02). SMs were a presenting symptom in FTC patients (41%) more often, while PTC SMs were more commonly identified after TC had been diagnosed (76%; p<0.05). Among the Group T patients, PTC presented more frequently with synchronous metastases (63%), while FTC was associated with metachronous metastases (64%; p<0.01). The mean period until establishing a diagnosis of SMs after the initial TC diagnosis in Group T was 82±37.4 months for FTC and 35±17.2 months for PTC (p<0.01).
In the FTC Group S, solid organ metastases were less common than in FTC Group T (p<0.01). Multisite FTC SMs were more frequently associated with the development of other bone non-SMs compared to solitary SMs (p<0.01), although there were no such associations for PTC.
First FTC distant metastases were diagnosed more often within bone, but initial solid organ metastases and bone metastases at the same time were found more commonly in patients with PTC (p<0.05).
In the patients with FTC, solid organ metastases were diagnosed as the first distant metastasis in 19% of the patients and progressed to 48% on follow-up, while 95% of the patients had bone metastases. Among the PTC patients, 36% had solid organ metastases as the first distant metastases, and this increased to 42% on follow-up, while 95% of the patients had bone metastases (p<0.05; Fig. 5).
The FTC patients presented with SMs with myelopathy or radiculopathy, while those patients with PTC either showed evidence of back pain or were asymptomatic (p<0.01).
The patients with FTC vertebral lesions took up 131I more often than those with PTC SMs (p<0.01). Surgery was performed significantly more frequently for patients with FTC SMs, while nonsurgical treatment was more commonly used for patients with PTC SMs (p<0.05).
MTC, HTC, and ATC
Of all the patients in the cohort, nine patients had MTC, six had HCC, and two had ATC. A summary of the patients' data is shown in Table 1. Because of their rarity, a comparative statistical analysis was not feasible.
Discussion
The first description of TC SMs was provided by Max Runge in Virchov's Archive in March 1876. He described a 41-year-old woman with severe neck pain who progressed to paralysis and death. An autopsy revealed a C1–C2 tumor compressing the spinal cord that histologically resembled thyroid tissue (62). Seven months later, Cohnheim published Simple Colloid Goiter with Metastases. He described the post-mortem examination of a patient with multiple tumors in the lungs, bronchial glands, spine, and femur, which resembled goiter, with nodules of the same appearance in the thyroid gland. Cohnheim noted that this growth could not be regarded as cancerous, and it was described as “benign metastasizing goiter” (63). In 1926, Simpson thoroughly reviewed 77 reported cases (including 25 with vertebral involvement) along with three of his own cases. He concluded that these entire osseous lesions, which resembled normal thyroid tissue, were actually metastases from an original thyroid cancer. Since the initial publication by Max Rouge in 1876, to our knowledge, no specific review devoted to the comprehensive analysis of SMs has been published.
Demographics of TC SMs
The relative incidence of PTC is higher (80%) than that of FTC (15%), but bone metastases are more frequent in patients with FTC compared to those with PTC at 7–28% and 1–7% respectively (64 –68). As in other studies, we found SMs to be more common in FTC than PTC patients (64,69). Moreover, patients with FTC are usually older at the time of initial thyroid surgery (70). However, the mean age of the patients from our groups with SMs at PTC and FTC diagnosis were 57.8±14 years and 56.7±14.4 years respectively, without differences in histological type, indicating that SMs may be a later event in patients with PTC. This age difference is consistent with other studies and may be attributed to a more aggressive form of TC that is associated with metastatic disease and reduced survival (64,71 –75).
Our male cohort constituted 41% of the patients. Other studies also showed a significant proportion of males with TC bone metastases (35–67%) compared to the male–female ratio seen in TC where females predominate. In contrast to those with FTC, among the patients with PTC, males predominated, which may indicate that sex is a risk factor for the development of PTC SMs. Furthermore, the males with PTC tended to be older than the females.
The most common mechanism for FTC metastatic spread is via a hematogenous route compared to the lymphatic spread of PTC (76). The propensity for axial skeleton SMs is thought to be secondary to blood flow distribution. Moreover, bone is a large repository for growth factors, which may assist in the propensity for bone seeding (68). We have demonstrated that the distribution of the FTC SMs matches the localization of the medullary segmental arteries (77,78).
Given that solitary SMs are found in roughly half the patients with SMs, perhaps a quarter of PTC and FTC patients with SMs can be considered for radical spinal surgery or radiosurgery to ensure the complete removal/destruction of metastatic tumor tissue with the intention of improving quality of life and potentially increasing survival. Certainly, patients with thyroid SMs are always at risk for additional bone or lung metastases in later years. Therefore, radical surgery or the radiosurgery of isolated SMs cannot be considered as curative treatments. However, utilizing these methods for patients with solitary thyroid SMs may potentially significantly prolong progression-free survival rates.
Moreover, those patients with TC who manifest with single-site SMs have a significantly lower probability of solid organ metastases compared to those who had SMs at the time of TC diagnosis or who developed TC during follow-up. The patients may initially present to a number of different medical specialties, such as neurology, orthopedics, neurosurgery, or general medicine (20). After an initial vertebral biopsy of the affected vertebra and confirmation of thyroid SMs, comprehensive imaging for the identification of other asymptomatic metastatic sites is important. For patients with SMs without bone non-SMs and solid organ metastases, radical treatment, that is, radiosurgery for localized vertebral lesions and total en-bloc spondylectomy for extended vertebral metastases, can be used. It seems that in the confirmed cases of thyroid SMs, when urgent surgery is required, the radical spinal surgery technique is preferable, since such patients have a relatively high chance of not having solid organ metastases.
Appearance of distant TC metastases
As previously shown, in terms of FTC, solid organ metastases were diagnosed as the first distant metastases in 19% of the patients in our study, with a subsequent increase to 48% during follow-up, while 95% of the patients had bone metastases. Even though all the patients had TC removal following the initial diagnosis of the disease, the number of solid organ metastases increased over time. In the case of PTC, 36% of the patients had solid organ metastases as the first distant metastases, and this number progressed to 42%, while 95% of the patients had bone metastases. It seems that little if no solid metastatic progression is seen. A large study on bone metastases—not only on spinal metastasis—is required to clarify metastatic progression.
Clinical presentation and treatments
Among all the patients with SMs, nearly 35% had an initial presentation of TC, whereas 65% were identified after TC diagnosis. According to our data, the FTC patients with SMs as an initial presentation had a significantly lower rate of solid organ involvement compared to Group T. The same was not evident for PTC patients. Accordingly, the patients with FTC had less advanced disease, and there was no age difference in comparison to the PTC patients. Bernier et al. also showed that patients who had signs of bone metastases as initial symptoms of TC had significantly higher survival rates (79).
In our study, SMs after TC diagnosis were almost equally divided between synchronous (46%) and metachronous metastases (54%). A similar distribution (50%/50%) was found by Zetting et al. for all bone metastases (1). To assess the distribution of SMs from FTC and PTC in this subgroup more precisely, we analyzed the synchronous and metachronous metastases in the patients in our study separately. The mean time for developing SMs in these patients was 35.3 months for PTC and 82.1 months for FTC. PTC often presented with synchronous metastases, while FTC mostly presented with metachronous metastases up to 372 months following the initial TC diagnosis. A heightened index of suspicion is a key element in the early evaluation and diagnosis of any patient with a history of TC.
Within our patient population, we identified a cohort of 10 women with FTC who had been operated on many years prior for seemingly benign thyroid lesions, and these patients later developed SMs. We can speculate that these patients had undiagnosed FTC microcarcinomas at the time of their original surgeries. These patients were considerably younger than the other FTC patients (36.4±0.4 years vs. 56.7±14.4 years respectively) and their metastases developed significantly later than those with other FTC metachronous metastases (221.7±138 months vs. 101.5±68.4 months respectively). With respect to the clinical presentation of thyroid SMs, the most commonly reported spinal symptoms were signs of direct neural structure compression, including myelo- and radiculopathy (67% of the patients), and back pain (28%). The patients with FTC presented with SMs accompanied by symptoms of neural structure compression, while the PTC patients were more likely to present with back pain or to be asymptomatic.
In our study, only 57.8% of all TC lesions were 131I avid, while other studies showed the range to be 43–73% (74,79,80). In our analysis, 65.8% of the FTC and 42.9% of the PTC vertebral lesions were 131I avid. However, the effect and significance of radioiodine therapy on SMs and its contribution is difficult to assess based on the existing literature. Our data may be biased because only lesions that we could clearly distinguish on scans were evaluated. Two-thirds (66.7%) of the patients in our study underwent surgery. Because FTC presented with symptoms of neural structure compression more often, surgery was used significantly more frequently for FTC than PTC patients. Radiosurgery, which has been shown to control tumor growth and palliate tumor-induced back pain, was used in 4.9% of the patients. External radiation was applied in 87% of the patients who received conservative treatment.
Conclusions
1. A significant proportion of TC patients with single-level SMs do not have any other distant metastases and may be considered for radical treatment.
2. Patients with SMs due to FTC who manifest TC have a better prognosis than those who develop SMs after TC diagnosis.
3. TC SMs may occur up to 372 months after the original TC diagnosis, which emphasizes the need for the long-term follow-up of patients with TC.
4. SMs originating from FTC and PTC appear to have distinct presentations, behaviors, and treatment modalities and should be categorized separately for treatment and follow-up planning.
5. The treatment of SMs requires a multidisciplinary approach that includes endocrine medical and surgical specialists, radiologists, and oncologists, in order to implement radical treatment methods (such as 131I, total en bloc spondylectomy, and radiosurgery) if possible.
Footnotes
Acknowledgment
We are grateful to Valentin M. Dotsenko, MD, PhD, for his help in statistical analysis.
Author Disclosure Statement
No competing financial interests exist.