
Abstract
Background:
Treatment options for patients with advanced or metastatic medullary thyroid cancer (MTC) have, in recent years, expanded with the approval of two tyrosine kinase inhibitors (TKIs): vandetanib and cabozantinib. Other agents, including TKIs, are under clinical investigation for MTC. Although patients treated with TKIs are at risk of developing dermatologic adverse events (AE), these untoward events may be mitigated through AE-driven algorithms.
Summary:
AE-driven algorithms combine effective nonpharmaceutical and pharmaceutical treatment modalities implemented by a multidisciplinary effort that incorporates nursing interventions, patient education, and referrals to pain-management specialists, podiatrists, and dermatologists, as appropriate. Effective AE prevention and management reduce the need for dose interruptions and modifications, allowing patients the opportunity to derive the maximal benefit from TKI therapy, while maintaining quality of life.
Conclusions:
Optimal use of targeted therapies in the treatment of MTC depends on careful patient selection, interdisciplinary communication, and patient education and encouragement to enhance compliance and safety, optimize consistent dosing, and maximize the use of effective therapies.
Introduction
T
The five-year relative survival rate for patients with MTC by stage at diagnosis is 98% for stages I and II, 73% for stage III, and 40% for stage IV (3). Lower clinical stage and younger age (<40 years) at diagnosis are strong independent predictors for improved survival (4).
Patients with MTC are susceptible to the development of early metastatic disease. For example, 50–55% of patients with MTC develop local metastases to the lymph nodes, and 20% have metastatic disease to the lung, liver, or bone at diagnosis (6,7).
The main goals of treatment for patients with metastatic disease are optimizing survival and quality of life (QoL). Currently, there is no curative systemic therapy for patients with MTC, and treatment options for patients with recurrent or persistent disease are limited (2,8). Vandetanib is an oral small-molecule multitargeted tyrosine kinase inhibitor (TKI) of the product of the Rearranged during Transfection (RET) gene, vascular endothelial growth factor receptor (VEGFR), and epidermal growth factor receptor (EGFR) signaling pathways (9,10). Another small-molecule TKI, cabozantinib, also inhibits multiple tyrosine kinases, including RET, VEGFR2, as well as mesenchymal-epithelial transition factor (MET) (11,12). The U.S. Food and Drug Administration (FDA) approved vandetanib and cabozantinib for the treatment of advanced MTC in 2011 and 2012 respectively (12,13). Vandetanib also received marketing approval for MTC in Europe and Canada. Cabozantinib has recently been approved for treatment of MTC by the European Medicines Agency for this indication (14). Other TKIs are under clinical investigation for MTC (15), some of which are currently marketed for other indications. TKIs have varying profiles of potential pharmacologic targets that include subtypes of VEGFR and EGFR, as well as other proto-oncogene targets (Table 1) (12,13,15 –21).
EGFR, epidermal growth factor receptor; HFSR, hand-foot skin reaction; MTC, medullary thyroid cancer; NR, not reported; NS, not specified; RET, Rearranged during Transfection; TKI, tyrosine kinase inhibitor; VEGFR, vascular endothelial growth factor receptor.
The present article focuses on the assessment and management of TKI-associated dermatologic events in patients with MTC. The rationale and data to support the use of TKIs in MTC, the dermatologic adverse events (AEs) associated with this treatment, and recommendations for prevention, management, nursing assessments, and patient education are described.
Review
Rationale for using TKIs in MTC
In the early 1990s, investigators found that mutations in the RET proto-oncogene are linked to the development of MEN2A, MEN2B, and FMTC (22 –25). Somatic mutations in RET are also common in sporadic MTC (26) and correlate with the risk of having lymph-node metastases at diagnosis, persistent disease, and shorter survival (27).
The RET gene encodes a transmembrane receptor tyrosine kinase that has important roles in cell growth, differentiation, and survival (5). The RET receptor is recognized by the persephin, artemin, and neurturin ligands that belong to the glial cell-derived neurotrophic factor family. The RET receptor is expressed by noradrenergic and dopaminergic neurons, thyroid C cells, and adrenal medulla. Gain of function or activating mutations in the RET gene are the primary cause of all hereditary MTC cases and between 25% and 50% of sporadic cases (5).
The vascular endothelial growth factor A (VEGF-A) and its VEGFRs, which have major roles in angiogenesis in normal tissues and malignant tumors, may also be involved in the development and maintenance of sporadic and hereditary MTC (28). VEGF-A and several VEGFRs are overexpressed in MTC biopsy specimens (28,29). In addition, VEGFR2 and EGFR are overexpressed in some metastases, while they are not expressed within the primary tumor, suggesting a role for these receptors in the progression of MTC (30). In preclinical studies using human thyroid tumor cell lines, high VEGF expression correlated with increased tumorigenic potential (31). Increased expression of MET has been observed in some MTC tumors (11,32).
Members of the RAS family of low-molecular weight GTP-binding proteins are important downstream mediators of effects occurring through these tyrosine kinases (33). RAS proteins are essential mediators in a variety of pathways that regulate normal and malignant cell proliferation (33). The RAS pathway, particularly through downstream effects at the RET receptor, has been implicated in MTC (34). In addition, a recent study in which the exomes of 17 sporadic MTCs were sequenced and compared with corresponding findings in an independent cohort of 40 sporadic and hereditary MTCs revealed that approximately 90% of MTCs have mutations in either RET or RAS (35). These mutations were found to be mutually exclusive, and few other types of mutations were identified.
In a phase III randomized double-blind study, vandetanib treatment (300 mg, administered orally, once daily) (13) compared with placebo significantly prolonged progression-free survival (PFS) in patients with symptomatic or progressive locally advanced or metastatic MTC (hazard ratio [HR] 0.46; 95% confidence interval [CI 0.31–0.69]; p<0.001) (18). Patients treated with vandetanib also showed improved objective response rates, disease control rates, and calcitonin and carcinoembryonic antigen biochemical response rates. Overall survival data are not yet available. The most common all-grade AEs (occurring at a frequency of ≥5%) reported for the vandetanib and placebo groups respectively were diarrhea (57% vs. 27%), rash (53% vs. 12%), dermatitis acneiform/acne (35% vs. 7%), nausea (33% vs. 16%), hypertension (33% vs. 5%), fatigue (24% vs. 23%), headache (26% vs. 9%), upper respiratory infection (23% vs. 16%), decreased appetite (21% vs. 12%), and abdominal pain (21% vs. 11%) (13). The study protocol mandated dose reduction from 300 mg/d to 200 mg/d for a grade 3 or 4 dermatologic AE (as well as for grade 3 or 4 gastrointestinal AEs and QTc prolongation) and another reduction to 100 mg/d if an additional grade 3 or 4 AE occurred (18).
Another phase III, double-blind, placebo-controlled study evaluated cabozantinib (140 mg, administered orally, once daily) compared with placebo in patients with actively progressive MTC within 14 months of screening (19). Median PFS was 11.2 months and 4.0 months in the cabozantinib and placebo arms respectively (HR 0.28; [CI 0.19–0.40]; p<0.0001) (12). An improvement in partial response rate was also observed in the group receiving cabozantinib compared with those receiving placebo. No statistically significant difference in overall survival was seen at the planned interim analysis. The most common all-grade AEs in the cabozantinib arm compared with the placebo arm were diarrhea (63% vs. 33%), stomatitis (51% vs. 6%), palmar-plantar erythrodysesthesia syndrome (i.e., hand-foot skin reaction [HFSR]; 50% vs. 2%), decreased weight (48% vs. 10%), decreased appetite (46% vs. 16%), nausea (43% vs. 21%), fatigue (41% vs. 28%), oral pain (36% vs. 6%), hair color changes (34% vs. 1%), dysgeusia (34% vs. 6%), hypertension (33% vs. 4%), constipation (27% vs. 6%), abdominal pain (27% vs. 13%), vomiting (24% vs. 2%), asthenia (21% vs. 15%), and dysphonia (20% vs. 9%) (12).
Dermatologic AEs associated with TKIs
Dermatologic AEs have been well characterized for TKIs that target the VEGFR or EGFR pathways. Patients treated with TKIs may experience cutaneous AEs such as rash, erythema, pruritus, acneiform rash, paronychia, telangiectasia, alopecia, changes in hair growth or pigmentation, skin discoloration, xerosis (dryness), and HFSR (36,37). Incidence and severity of dermatologic AEs vary across the specific targeted therapies used and prescribed doses. While the factors that determine the profile of AEs have not been fully elucidated, risk factors that may be associated with skin reactions subsequent to EGFR inhibition include age, smoking status, and exposure to ionizing and ultraviolet (UV) radiation (e.g., sunlight) (38).
Putative mechanisms
The EGFR, which is thought to play an important role in the proliferation of the basal epidermal layer, is expressed at high levels in the basal and suprabasal layers of the skin, and in the outer layers of hair follicles (37). In experimental systems, inhibition of EGFR signaling in keratinocytes causes growth arrest, initiation of differentiation, and apoptosis. In patients treated with EGFR inhibitors, histologic analysis of the skin has revealed marked downregulation of phosphorylated EGFR and decreased proliferation and premature differentiation of basal keratinocytes (37). Thus, skin AEs associated with EGFR-inhibitor treatment are likely to be linked to the overall inhibition of EGFR signaling in basal keratinocytes, leading to alterations in keratinocyte survival, proliferation, differentiation, migration, and attachment (37,39). EGFR inhibition can also cause an inflammatory response by triggering the release of cytokines and the resultant recruitment and activation of neutrophils, monocytes, and lymphocytes (39). Inflammation is a secondary but important contributor to the development of these dermatologic AEs (39). The pathogenic mechanism for the development of HFSR is thought to involve combined inhibition of the VEGFR and platelet-derived growth factor receptor (PDGFR) proangiogenic pathways, possibly preventing the proper implementation of vascular repair mechanisms in these high-pressure areas (36).
Types of skin AEs linked to specific drugs
Table 1 lists the incidence of dermatologic AEs associated with the TKIs vandetanib, sunitinib, sorafenib, and cabozantinib in clinical trials of patients with locally advanced or metastatic MTC (12,13,15 –21). Table 2 presents a grading scale on the severity of these AEs provided in the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE) (40).
National Cancer Institute Common Terminology Criteria for Adverse Events (40).
ADL, activities of daily living; AEs, adverse events; BSA, body surface area; CTCAE, National Cancer Institute's Common Terminology Criteria for Adverse Events; IV, intravenous; NSAIDs, nonsteroidal anti-inflammatory drugs.
In the placebo-controlled phase III study of patients with MTC, dermatologic AEs of vandetanib were, in decreasing order of incidence, rash, dermatitis acneiform or acne, dry skin, photosensitivity reactions, pruritus, and nail abnormalities (Table 1) (13). Severe skin reactions, such as Stevens–Johnson syndrome, were rare, although some led to death or permanent treatment discontinuation (13). A systematic review and meta-analysis of nine studies of single-agent vandetanib in 2961 patients found a 46.1% incidence of all-grade skin rash and 3.5% high-grade skin rash (41). The same analysis reported that, when compared with controls in randomized studies, patients treated with vandetanib had a 2.43 relative risk ([CI 1.37–4.29]; p=0.002) of developing an all-grade rash. An analysis of the skin toxic effects observed in three clinical trials of patients receiving vandetanib for the treatment of advanced MTC revealed two additional dermatologic AEs: photodistributed erythematous eruptions and skin pigmentation changes (e.g., appearance of gray-blue macules on the face, scalp, or trunk) (42). Discontinuation of therapy was associated with rapid improvement in almost all patients with skin phototoxic effects, and reinitiation of therapy at a lower dose accompanied by strict photoprotection measures was successful in preventing a recurrence of this AE (42). A gradual disappearance of pigmented macules over a three- to six-month period was noted upon treatment discontinuation (42).
Dermatologic AEs associated with cabozantinib treatment in patients with MTC from the placebo-controlled phase III study were, in descending order, HFSR, hair color changes, rash, dry skin, alopecia, erythema, and hyperkeratosis (Table 1) (12).
Data from trials in MTC represent relatively small numbers of patients. Hence, the occurrence and incidence of these skin reactions may not be representative of experience in the overall population of patients treated with TKIs for all forms of cancer.
In registration studies for sunitinib, rash (29%), HFSR (29%), skin discoloration (25%), dry skin (23%), and hair color changes (20%) were among the most common AEs experienced by patients with renal cell carcinomas. Similar dermatologic AEs were reported in patients with gastrointestinal stromal tumors or pancreatic neuroendocrine tumors (43). Warning notices or precautions for dermatologic AEs are not listed in the manufacturer's prescribing information.
In patients with renal cell cancer and hepatocellular cancer, HFSR and rash are the most common dermatologic AEs associated with sorafenib treatment. They are usually grade 1 or 2 according to the National Cancer Institute's CTCAE grading scale and typically occur during the first six weeks of treatment (40,44). In registration studies of sorafenib in patients with hepatocellular carcinoma and renal cell carcinoma, up to about 1% of patients had to permanently discontinue treatment due to HFSR. In the sorafenib prescribing information for dermatologic events reported from multiple clinical trials, erythema occurred in ≥10% of patients, and exfoliative dermatitis, acne, and flushing in 1% to ≤10% of patients (44).
Photographs of representative patients exhibiting some of the skin reactions associated with TKI therapy are shown in Figure 1.
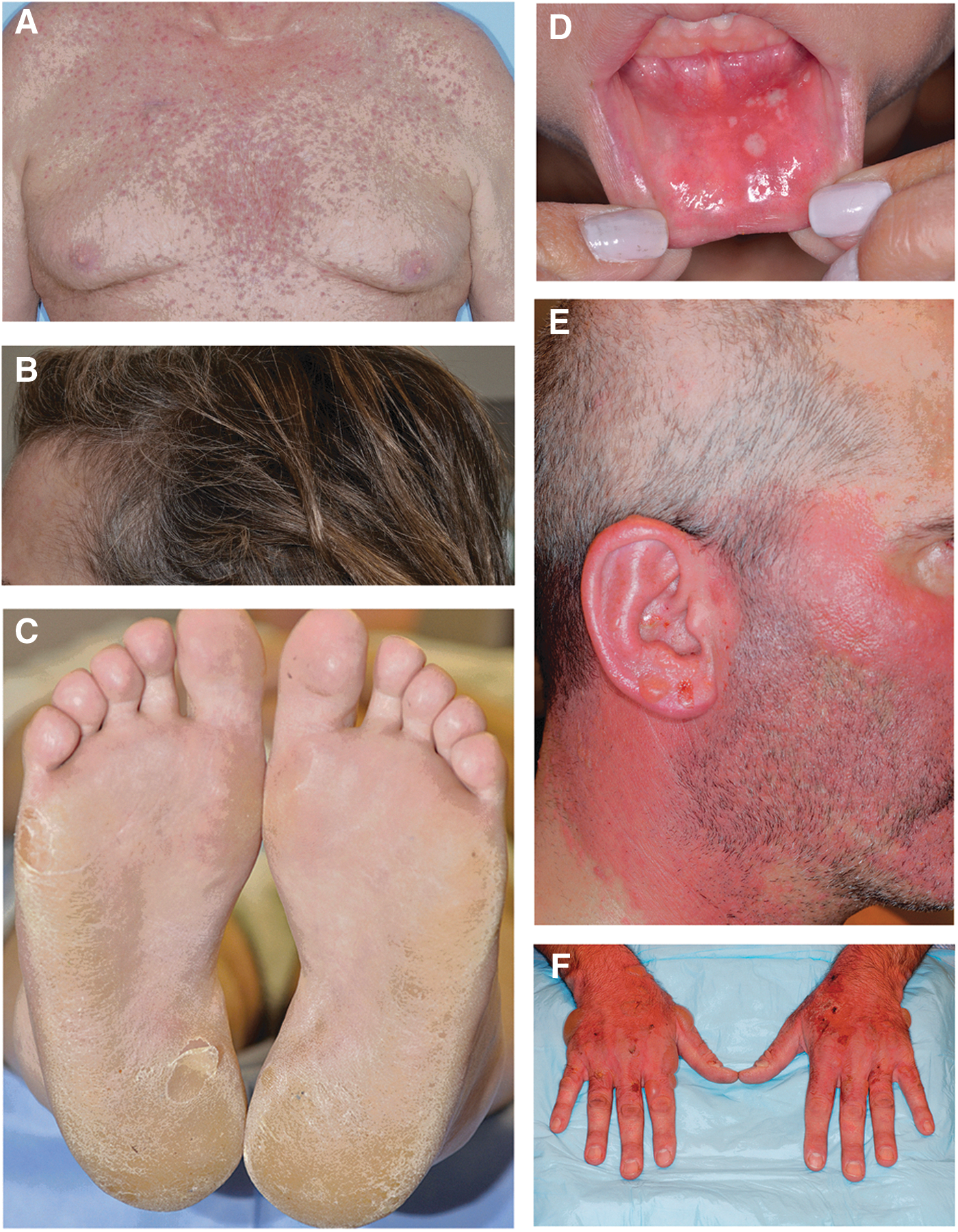
Photographs of representative patients exhibiting skin reactions associated with tyrosine kinase inhibitor (TKI) therapy.
Impact of dermatologic events on QoL
Dermatologic events can cause physical discomfort such as pain, burning, and increased skin sensitivity (45). These symptoms can affect a patient's ability to perform activities of daily living such as eating, grooming, exercise, and work. The effects of EGFR inhibitor-induced dermatologic AEs on QoL (46), including xerosis, rash, pruritus, and paronychia, resulted in decreased QoL, with rash having the highest impact. Younger patients reported decreased overall QoL compared with older patients for the same AEs (46).
Symptoms from ineffectively managed dermatologic AEs may also cause depression, frustration, worry, and withdrawal from certain social activities, thereby affecting a patient's physical, functional, emotional, and social well-being (45). Moreover, HFSR results in decreased QoL due to the associated symptoms of pain and tenderness (47).
Although data are limited, it is important to note the financial impact of managing dermatologic AEs to the economic burden of cancer care. Assessment and management may involve ongoing long-term care from multiple healthcare professionals over multiple visits to the clinic or office.
Management
Guidelines and recommendations
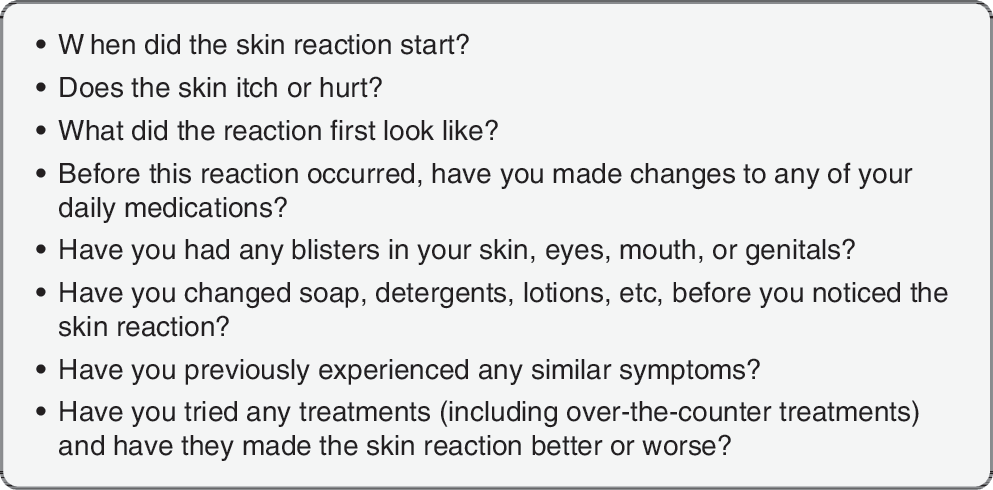
Prior to starting an oncology patient on any type of treatment, a thorough medical history must be taken to document the patient's history of cancer treatments and past skin disorders, their current medication profile, and presence of current skin disorders or symptoms (48). Patients with skin symptoms should be asked specific questions regarding the location, onset, duration, relieving factors, severity, and history of medications (Fig. 2) (49,50).
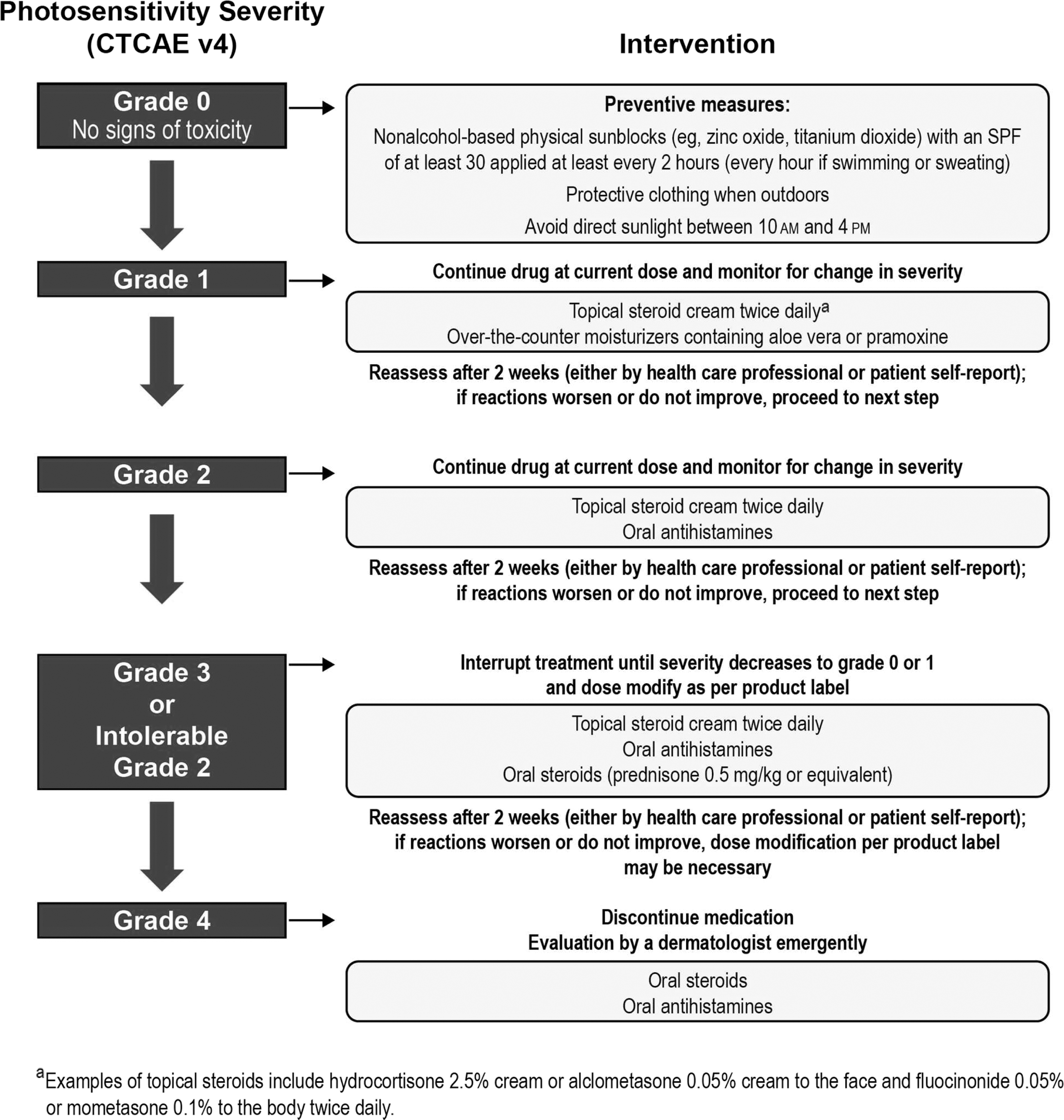
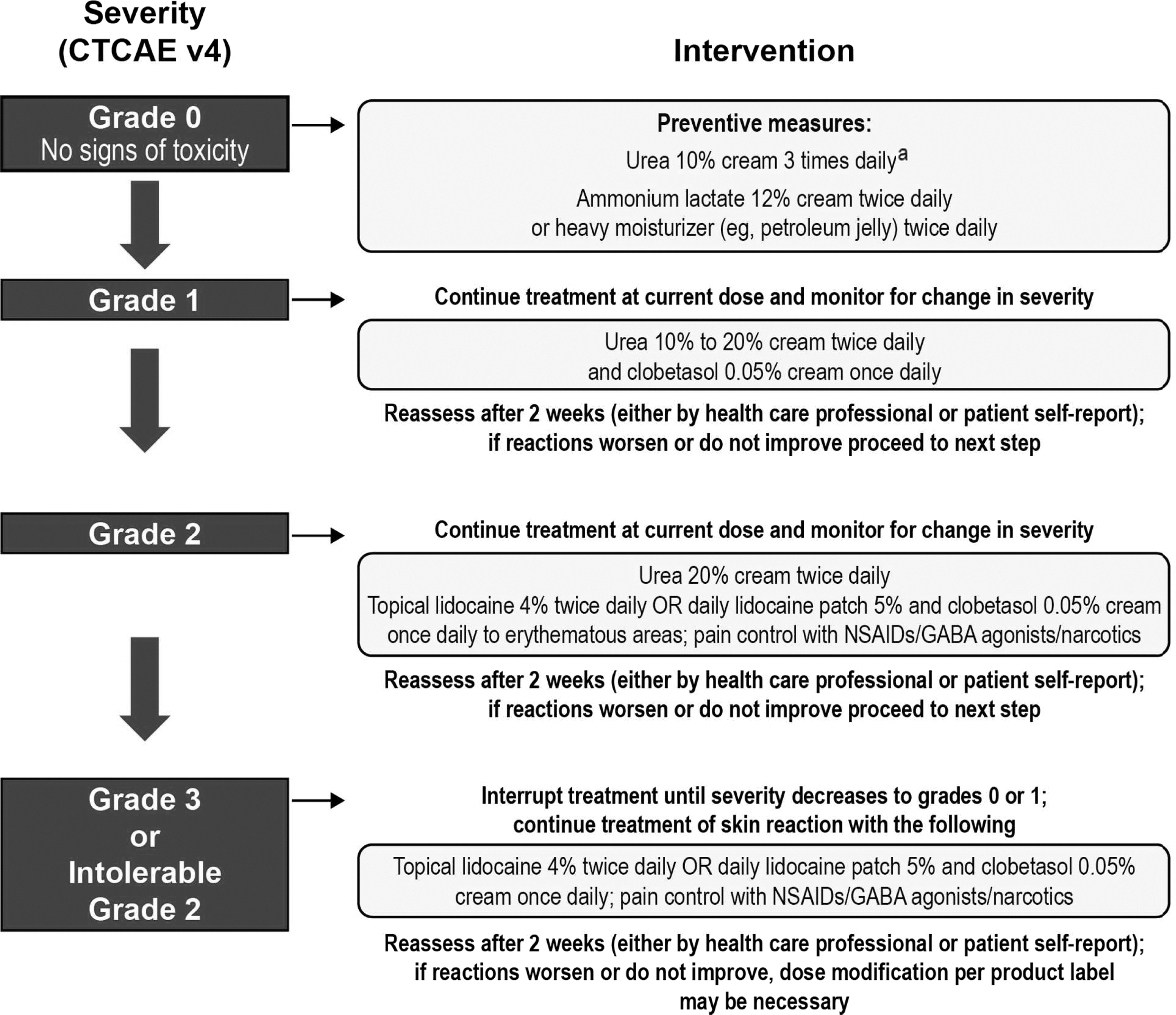
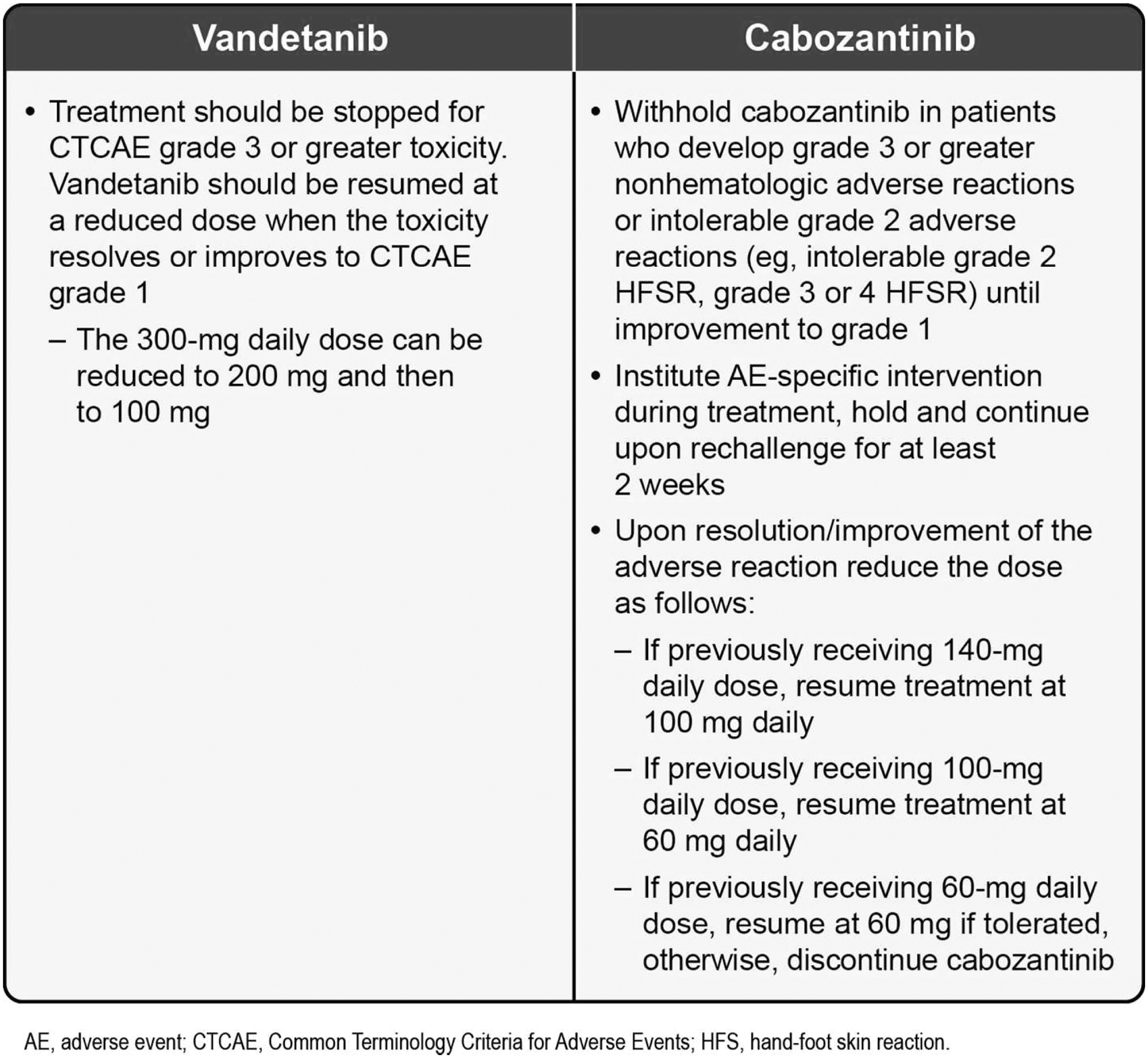
Various recommendations exist for the management of TKI-associated dermatologic AEs (36,38,51 –54). Figures 3 (51 –53), 4 (55), 5 (38), and 6 (12,13) also provide specific guidance. There have not been any prospective randomized trials to evaluate the best management strategies for these dermatologic AEs in patients with MTC. Recommendations are based on the evaluation of existing data and clinical experience (36). An important message from all these publications is the need for practitioners to develop and consistently implement effective algorithms for AE management (see Figs. 3 –5 for examples of effective algorithms for management of photosensitivity, HFSR, and acneiform rash, respectively). Careful management is critical in allowing the patient to gain the most benefit from therapy by avoiding or limiting dose interruptions and modifications (36). However, these considerations must be balanced with the important goal of maintaining patients' QoL by minimizing the negative effects of debilitating AEs, particularly dermatologic AEs. In the case of serious drug-related dermatologic AEs, dose reductions, modifications, or interruptions might be necessary, as recommended by the product prescribing information. For example, in the cabozantinib prescribing information, dose interruptions are recommended for patients experiencing intolerable grade 2, grade 3, or higher grade skin toxicities, and some patients may require dose modifications at treatment reinitiation. These recommendations are described in Figure 6 (12,13).

Intervention algorithm for acneiform rash (38). Published in Balagula Y 2011 Int J Dermatol
Preventive measures
Results from a randomized study in 95 patients with metastatic colorectal cancer undergoing treatment with the EGFR monoclonal antibody inhibitor panitumumab suggest that preventive therapy may be more effective than reactive therapy in the management of dermatologic AEs with EGFR inhibitors (56). Patients in this study were randomized to pre-emptive treatment, consisting of skin moisturizers, sunscreen, topical steroid, and doxycycline, or reactive treatment begun after dermatologic AE development. The primary objective of the study was to assess the difference in the incidence of protocol-defined grade ≥2 skin AEs between the two groups during the six-week dermatologic treatment period. An approximate 50% reduction in skin AEs was observed in the pre-emptive versus reactive groups (56). Another study has demonstrated the effectiveness of prophylaxis in reducing the incidence or severity of grade ≤2 skin toxicities linked to treatment with the anti-EGFR monoclonal antibody cetuximab in patients with metastatic colorectal cancer (56,57).
Of 868 patients treated with sorafenib for hepatocellular carcinoma, a reduction was seen in the incidence of all-grade HFSR (56% in treatment arm vs. 73.6% in controls; p<0.0001), and a 2.5-fold increase in the median time-to-first onset of HFSR (84 days in the treatment arm vs. 34 days in controls; p<0.001), with the preventive daily use of urea-based cream (58). Figures 4 (55) and 5 (38) provide recommendations for the prevention of HFSR and acneiform rash respectively.
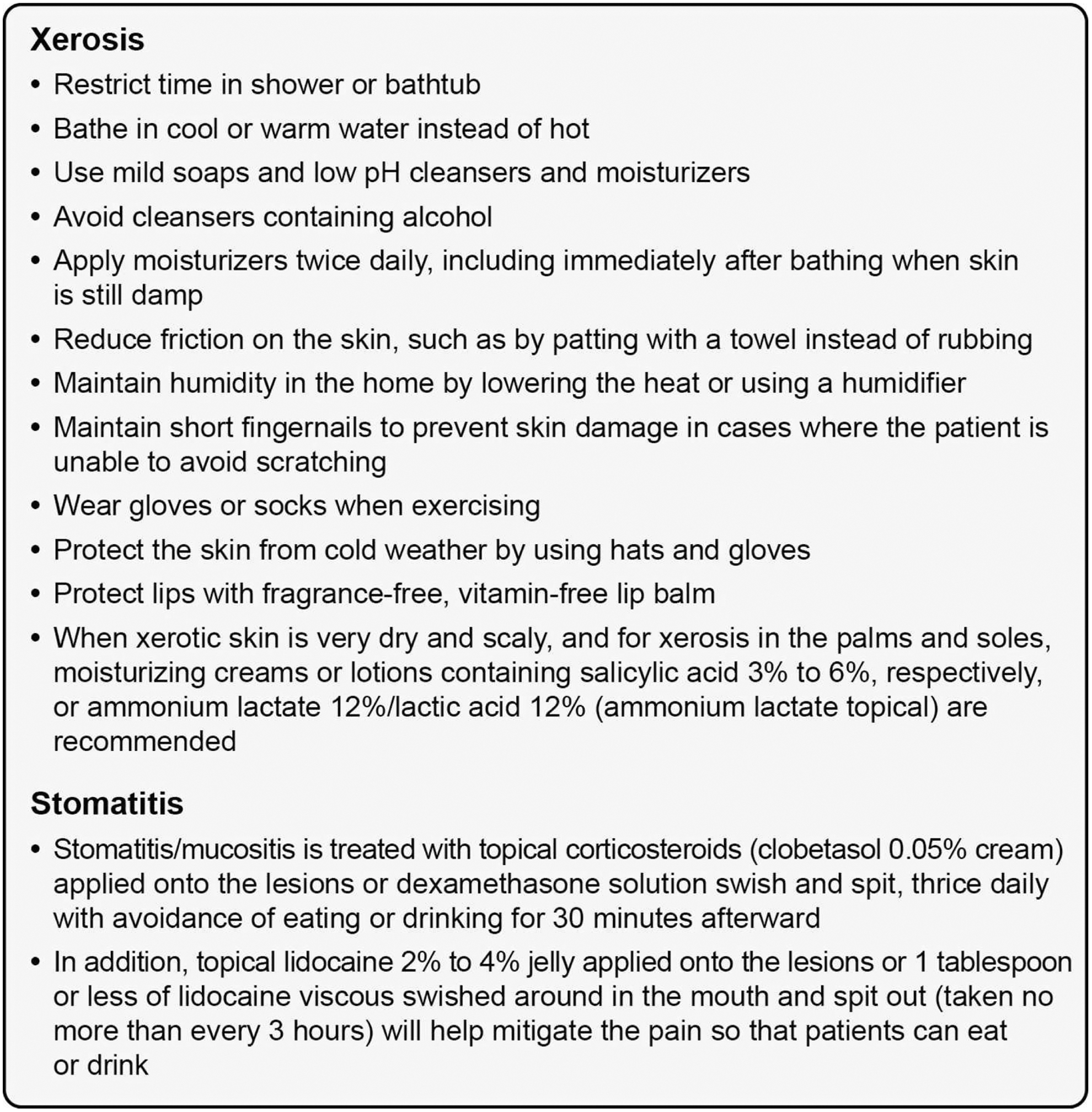
Stomatitis from targeted therapies is characterized by well-defined round plaques <0.5 cm in diameter affecting the lips, tongue, and oral mucosa (59,60). The lesions are very painful and may impair the ability to eat, drink, or speak (59,61). These aphthous-stomatitis–like lesions are treated with topical corticosteroids (e.g., clobetasol 0.05% cream) applied onto the lesions or dexamethasone solution swish and spit, taken three times daily with avoidance of eating or drinking for 30 minutes afterward (59,61). In addition, topical lidocaine 2–4% jelly applied onto the lesions, or one tablespoon or less of lidocaine viscous swished around in the mouth and spat out (taken no more than every 3 h), will help mitigate the pain so that patients can eat or drink (38).
General supportive measures
Supportive measures should include advice for patients on how to manage dry skin. A thick alcohol-free emollient (e.g., Vanicream®, Pharmaceutical Specialties, Inc., Rochester, MN; Eucerin®, Beiersdorf AG, Hamburg, Germany) is recommended for moisturizing dry areas of the body (62,63). When xerotic skin is very dry and scaly, and for xerosis in the palms and soles, moisturizing creams or lotions containing salicylic acid 3–6%, respectively, or ammonium lactate 12%/lactic acid 12% (ammonium lactate topical) are recommended. Figure 7 (49,59,61,64,65) provides measures that may be helpful in preventing and managing xerosis and stomatitis.
Patient education
Patient and caregiver education is extremely important for the prevention, early recognition, and management of dermatologic AEs. It is recommended that this education start at the beginning and be reinforced throughout treatment by dermatology and oncology specialists. A patient-appropriate guide can be provided describing the common side effects experienced with a particular TKI. Specific instructions on when to call a doctor's office to discuss onset or exacerbation of symptoms should also be provided. Patients should keep documentation of the location, onset, symptoms/quality, treatment, and self-evaluation of all their AEs and bring concomitant medications to the clinic so the healthcare team can determine if they may be causing or worsening AEs. For example, topical and oral retinoids may lead to dryness and may worsen burning or irritation of skin rashes caused by EGFR inhibitors (51).
Nurses have an important role in patient education related to dermatologic AEs. Both healthcare providers and patients may view nurses as spending more time with patients and giving more in-depth treatment instructions than other professionals (66). Therefore, to prevent alteration of anticancer treatment administration and produce optimal results for patient care, nurses must understand the basis of side effects, impact on QoL, and pre-emptive measures, and must be able to provide optimal psychosocial support.
According to one survey, prior to treatment initiation, cancer survivors considered skin irritation and dry skin to be minor concerns compared with AEs such as a weaker immune system, hair loss, and fatigue (67). However, after undergoing treatment, most patients reported that dry skin and skin irritation were important concerns that heavily impacted their lives. Most respondents said that skin AEs were worse than expected, indicating they had either underestimated the potential impact of dermatologic AEs prior to initiation of therapy or had not been sufficiently informed. These data emphasize the importance of patient education.
Conversations with your patients
Conversations between the treatment team and patients should enhance patients' control over disease management. The cause, course, treatment, and management of disease side effects should be discussed (68). Emotional and informational support for patients with cancer is likely to have a beneficial impact on psychological adjustment (68). Such educational interventions may also help increase patient self-esteem and outlook, especially when management strategies are implemented effectively. More data are needed on the psychological needs of patients with dermatologic AEs linked to treatment with targeted therapies to improve the accuracy of assessments and to develop even more effective patient education (69). Oncology nurses provide an easily accessible sounding board for patients to express their psychological as well as physical concerns (70). Therefore, in addition to educating patients on interventions to ease the physical impact of the AEs, nurses can help determine when referral for psychosocial counseling is appropriate.
Patient education on specific topics: protection from UV radiation
Thick application of sunscreen and wearing protective clothing whenever possible should be emphasized, since UV radiation can trigger rash and photosensitivity in patients treated with vandetanib and sorafenib (44,51). Nonalcohol-based physical sunblocks (e.g., zinc oxide, titanium dioxide) with a sun protection factor of 30 that inhibit both UVA and UVB radiation are recommended because they are effective and cause less irritation than other types of sunscreen. To provide the best sun protection, patients should also be advised to be in the shade between 10:00
Patient education on specific topics: typical timing for development of acneiform rash and HFSR
It is critical to inform patients that both the acneiform rash and HFSR typically develop within the first eight weeks of therapy (71). Knowing that these events peak in severity during this time ensures close follow-up and care during this time, while reassuring patients that they will not endure these toxicities during the entire duration of their therapy.
Summary and Conclusions
The treatment options available for patients with metastatic MTC have been expanded with the FDA approval of vandetanib and cabozantinib. Other TKIs are under clinical investigation for MTC, including some currently marketed for other indications. Patients treated with TKIs are at risk of developing dermatologic AEs, a common type of AE associated with this class of agents. The risk of developing these dermatologic AEs can be reduced and their impact may be diminished through development and implementation of preventive and management algorithms. These algorithms combine nonpharmaceutical and pharmaceutical treatment modalities that are best implemented by a multidisciplinary effort, incorporating nursing interventions, patient education, and referrals to pain-management and dermatologic specialists, as appropriate. Effective AE prevention and management reduces dose interruptions and modifications, enabling patients to derive the most benefit from anticancer therapy, while maintaining a good QoL. Effective management of targeted therapies in the treatment of MTC strongly relies on patient education, interdisciplinary communication, and encouragement to minimize interruption of otherwise effective treatment.
Footnotes
Acknowledgments
We thank Monica Nicosia, PhD, and Antoinette Campo from SCI Scientific Communications & Information (SCI), and Jennifer Steeber, PhD, and Susan Moench, PhD, PA-C, formerly of SCI, who provided medical writing support funded by AstraZeneca LP.
Author Disclosure Statement
Mario E. Lacouture is a consultant for AstraZeneca. Richard T. Kloos is an employee and stockholder in Veracyte, Inc. The remaining authors have no competing financial interests.