
Abstract
Background:
Familial adenomatous polyposis (FAP) is a hereditary colon cancer syndrome that involves multiple extracolonic organs, including the thyroid. Several studies have estimated the rate of thyroid cancer in FAP to occur at five times the rate of the general population, but no current consensus defines screening for thyroid cancer in this cohort. This study seeks to define the features of benign and malignant thyroid disease in FAP patients, to compare thyroid cancer cases found through screening with those found incidentally, and to propose disease surveillance recommendations.
Methods:
Prospective screening for early thyroid cancer detection with thyroid ultrasound (US) was performed on FAP patients at the time of annual colonoscopy since November 2008. Clinical and US data were reviewed to characterize the observed thyroid nodules. Nonscreening-detected cases (NSD) were found through review of the colon cancer registry database.
Results:
Eighteen NSD were found, compared with 15 screening-detected (SD) cases, out of 205 total patients screened (M age=42 years; 55% female). The mean tumor size was larger in the NSD group than the SD group (p=0.04), and they tended to demonstrate more positive lymph nodes and more complications than the SD group. In the screened cohort, at least one thyroid nodule was detected in 106 (51.7%) patients, with 90% of these seen on initial exam. A total of 40/106 (37.7%) patients required fine-needle aspiration biopsy of a dominant nodule (M size=14 mm), and 28/40 (70%) of these were performed at the first US visit. Suspicious US features were present in 16/40 (40%) patients, including five sub-centimeter nodules. Cytology and/or nodule US was abnormal in 15/205 screened patients, leading to surgery and revealing 14 papillary and one medullary thyroid cancer.
Conclusions:
Given the age and sex distribution of the screened cohort, this study reveals a higher-than-expected prevalence of both benign and malignant thyroid disease in the FAP population. Additionally, SD cases seemed to consist of smaller-sized cancers that required less radical therapy compared to NSD cases. Since it was found that the initial US in the screening program accounted for the majority of detected nodules (90%) and biopsies (70%), baseline and subsequent thyroid US surveillance is recommended in all FAP patients.
Introduction:
F
Furthermore, while several studies have investigated the incidence of thyroid carcinomas, there is very limited information on the prevalence of benign thyroid diseases in this population. Herraiz et al. found thyroid nodules in 70% of the men and 83% of the women in their FAP registry who underwent screening thyroid ultrasound (US), which are much higher rates than those found in the general population (11). Two other studies have found rates varying from 38% to 9.1% (12,13). To the authors' knowledge, there have been no published studies on the results of an ongoing prospective thyroid US screening program in this cohort of patients.
Currently, there is no consensus of clinical practice parameters defined for screening or long-term disease follow-up of thyroid cancer in this genetic syndrome. Many management approaches have been suggested, ranging from no screening (4,14,15) to physical exam and thyroid gland palpation only (5). Many agree that some type of surveillance is necessary, but do not specify the extent or frequency (16,17). Ultrasonography has been proposed as one such method of screening (6,8,11). It is important to note that many of these studies are based on an older set of data, and also do not take into account the increased incidence of benign disease. As improvements in the management of the primary colonic disease in FAP lead to a more normal life expectancy, it is increasingly important to determine the best clinical management of the extracolonic manifestations (1,18). This study aims to characterize both benign and malignant thyroid disease in the FAP patients from the authors' institution's colon cancer registry, and to clarify the necessity for thyroid carcinoma screening and long-term follow-up. The hypothesis is that there will be a greater prevalence of benign thyroid diseases and thyroid cancer in patients in the database compared to the general population, and that these patients may benefit from regular US screening in order to avoid thyroid cancer morbidity and/or mortality.
Materials and Methods
The Jagelman Hereditary Colon Cancer registry was established in 1979 and is currently the world's largest retrospectively and prospectively maintained colon cancer registry. FAP patients comprise the majority of the registry's patient population. Patients are referred from within the hospital system, from outside hospitals, or are self-referred. All probands confirmed to have a genetic syndrome either through clinical criteria and/or through genetic testing are then consented to be included in the registry, and information about family members is collected (and confirmed through consent as appropriate). Patient and kindred information is maintained and actively entered into the electronic database, Cologene, on a daily basis by dedicated registry personnel.
Patients included in this study were confirmed to have FAP either by direct germline APC testing, or by fulfillment of established clinical criteria for the syndrome, including diffuse colonic adenomatous polyposis, presence of extracolonic manifestations of FAP (e.g., fundic gland polyps, duodenal adenomas, ampullary adenomas, desmoids tumors or osteomas), and a family history of FAP. This cohort was queried for thyroid cancer, and their medical records and reports as well as registry records were reviewed as available.
A prospective thyroid US screening program was started for FAP patients in 2008. The time period included in this analysis was November 2008 to November 2012. All FAP patients older than 16 years of age who underwent regular gastrointestinal screening and disease follow-up at the authors' institution were referred for thyroid screening US performed by endocrine surgeons. Patients were solicited for personal and family history of both benign and malignant thyroid disease. US were performed with ALOKAα-7 and 400, each with a high-resolution 7.5–13 mHz linear or curvilinear transducer (ALOKA Co., Ltd., Wallingford, CT). Nodule biopsy was performed according to standard American Thyroid Association guidelines: nodules ≥1 cm in size were sampled, and sub-centimeter nodules were only sampled if there was presence of suspicious sonographic features (e.g., microcalcifications, hypervascularity, etc.) (19). This was felt to be appropriate, as polyposis is cited as one of the pertinent historical factors predicting thyroid malignancy, alongside a history of childhood head and neck radiation, a family history of thyroid carcinoma, a thyroid cancer syndrome, and several other known factors (19). If patients did not have nodules or suspicious findings on exam, they were recommended to return for repeat screening in one year or longer as per the discretion of the clinician. Patients with suspicious or borderline nodules were surveyed more frequently within a year, also per the discretion of the clinician. At a weekly patient care conference, or ad hoc in clinic, any US findings that were unusual were discussed within the group to reach a consensus recommendation for management.
Registry and medical records were reviewed for demographic information (e.g., date of birth, sex), age at thyroid cancer surgery, age at FAP diagnosis, modality of FAP diagnosis, date of most recent follow-up, presence of extracolonic manifestations, and, if applicable, number of US screenings and descriptions of all nodules found. Specifically, number, size, location, and US characteristics of nodules were recorded for all patients. All of the above information was collected from a combination of archival paper medical records, electronic medical records, and Cologene.
Statistical analysis
In order to calculate incidence-related statistics, screened patients with confirmed FAP status who developed thyroid cancer during the period of observation were counted as observed cases. Person-years of observation (PYO) were counted from birth to age of death, most recent follow-up, or cancer development. These data were compared to Surveillance, Epidemiology, and End Results (SEER) data for years 2000–2010, which was the most recent available time range. For age-adjusted analysis, 18 age brackets were used, and sex and race were combined for each age bracket. The expected number of cases was calculated by the number of PYOs multiplied by the SEER incidence rates for each age bracket.
Period prevalence is the epidemiological term best suited for describing the thyroid cancer cases found through our screening program, which included both “existent” cases as well as “incident” cases that developed over the course of screening.
Tests for significance involving comparisons between screening-detected (SD) and nonscreening-detected (NSD) cases were performed using 2×2 contingency tables and Fisher's exact test for categorical variables. For continuous variables, such as age and size of tumor, the Mann–Whitney U-test was used.
This study was approved by the Institutional Review Board of the Cleveland Clinic.
Results
Retrospective review of FAP registry: NSD thyroid cancer cases
There are approximately 880 FAP kindreds in the Jagelman registry, as found through Cologene. Eighteen historical, or NSD, cases were found through a review of this cohort, and were confirmed through paper and/or electronic medical records of their thyroid cancer, as well as their FAP status. The mean age of FAP diagnosis was 20 years old (median 19.5 years), and 16/18 patients were female (89%). Six of the 18 (33%) were documented to have thyroid-related findings on physical exam, including either an enlarged gland or a palpable neck mass. Seven of the 18 (39%) were symptomatic, presenting with difficulty swallowing, difficulty breathing, rapidly enlarging goiter or self-discovered neck mass, and thyroid tenderness.
The mean age of thyroid cancer surgery was 26 years old (median 24 years; range 15–39 years). Thirteen patients underwent total thyroidectomies, two underwent subtotal thyroidectomies, and four of these required lymph node dissections. The remaining three cases underwent lobectomies, and two of these cases required reoperation, one of which also required lymph node dissection. All of these patients had papillary thyroid cancer (PTC) on surgical pathology, but only one case was specifically documented as being the cribriform-morular variant. The mean primary tumor size was 2.4 cm. Of the records that indicated laterality of disease on pathology, 8/14 (57%) were bilateral; of those that indicated multifocality, 7/13 (53%) were found to have multiple foci. All five patients who underwent lymph node dissections were found to have positive lymph nodes. Thirteen of 18 (72%) underwent radioactive iodine ablation after surgery. Since all patients were younger than 45 years of age, all had stage I cancer, except one patient who developed distant metastases (stage II). In fact, 3/18 (17%) patients experienced complications, including vocal cord paralysis, tracheostomy for local invasion, and acute postoperative hematoma requiring temporary tracheostomy. One patient developed local recurrence, and another developed distant metastases and eventually died from her disease. The mean length of follow-up for this group was 83 months.
Prospective thyroid cancer screening program: benign nodules and workup
A total of 205 patients were screened since the inception of the thyroid US screening program with at least one screening visit. The mean age of all screened individuals was 42 years old, and 93/205 (42%) were male. Ninety-nine patients (47.8%) were never found to have evidence of nodules during their period of follow-up. One hundred and six patients (51.7%) were found to have nodules detected on US screening, and all but 10 of these patients (47.6%) were found to have them on first-time screen. US findings in these 10 patients (4.9% of entire screened cohort) that developed after an initial normal US were sub-centimeter colloid/cystic changes that did not require biopsy. One patient was found to have compressive symptoms from goiter, and underwent a total thyroidectomy for this indication and was not found to have cancer on final pathology. Another screened patient had a history of head/neck radiation in addition to a positive FAP status, so this individual opted for a total thyroidectomy as well. The final pathology showed sub-centimeter foci of PTC.
Of those found to have nodules, 40 patients fulfilled biopsy criteria and underwent fine needle aspiration (FNA) at least once, and a total of 44 FNA biopsies were performed. Twenty-nine of these biopsies were performed on the first US screening, and the rest were performed at subsequent visits. All of the nodules biopsied during a subsequent visit were due to increase in size to >1 cm, or development of suspicious sonographic features (see Table 1). Thirty-eight were biopsied as they were >1 cm, and 11 of these also had suspicious sonographic characteristics. The remaining six biopsies were sub-centimeter nodules that were indicated due to suspicious sonographic features (see Fig. 1). The average size of nodules at the time of biopsy was 1.35 cm. Fifteen of the 40 patients had cytology that required surgery. Of the noncancerous cytologies, only two were nondiagnostic. Repeat biopsies for both showed a negative pathology: one describing a benign follicular nodule, and the other showed benign findings with Hürthle cell features as compatible with Hashimoto's thyroiditis. There were no reports of atypia of undetermined significance (AUS) or follicular lesions of undetermined significance (FLUS) in this group.
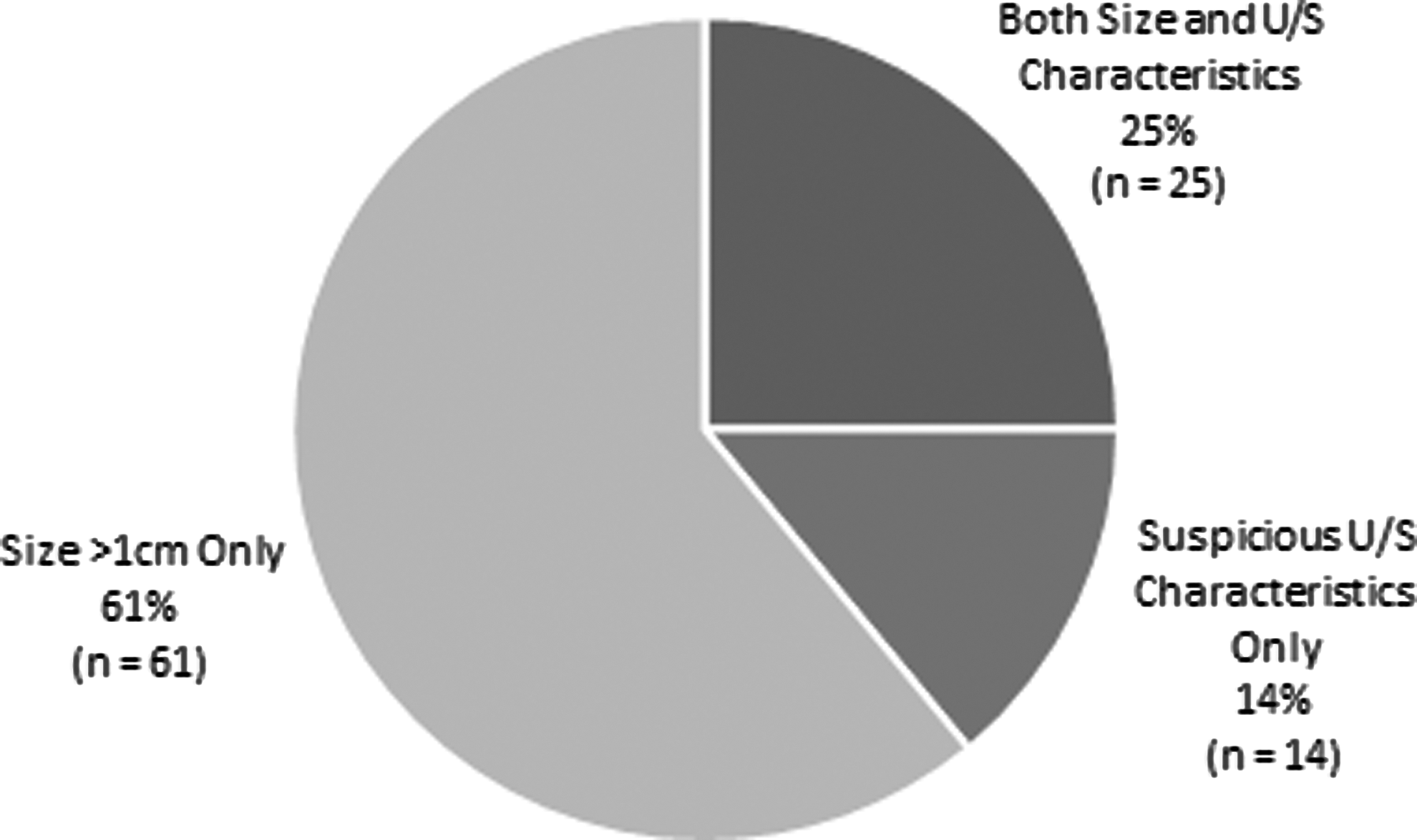
Indications for biopsy of nodules appreciated on ultrasound (US). The main indication for biopsy of nodules in the screened cohort was size >1 cm. Six sub-centimeter nodules were biopsied for suspicious US characteristics only.
The majority of nodules detected in the screening cohort were found on the first ultrasound (US) screening visit. Most of the nodules that required biopsy were also found on first-time screening.
For the aforementioned 15 patients with cytology necessitating surgery, all were found to be positive for cancer on final pathology. Figure 2 shows the mode of recognition and reason for surgery for all 15 of these thyroid cancer cases. Fourteen cases underwent surgery because of FNA findings, and one case was operated due to compressive symptoms and the size of the thyroid gland and was found to have cancer on final pathology. Five of these SD cases were specifically found to be the cribriform-morular variant of PTC (36% of SD papillary cases). Figure 3 shows a summary of the breakdown for the nodule workup for the entire screening cohort.
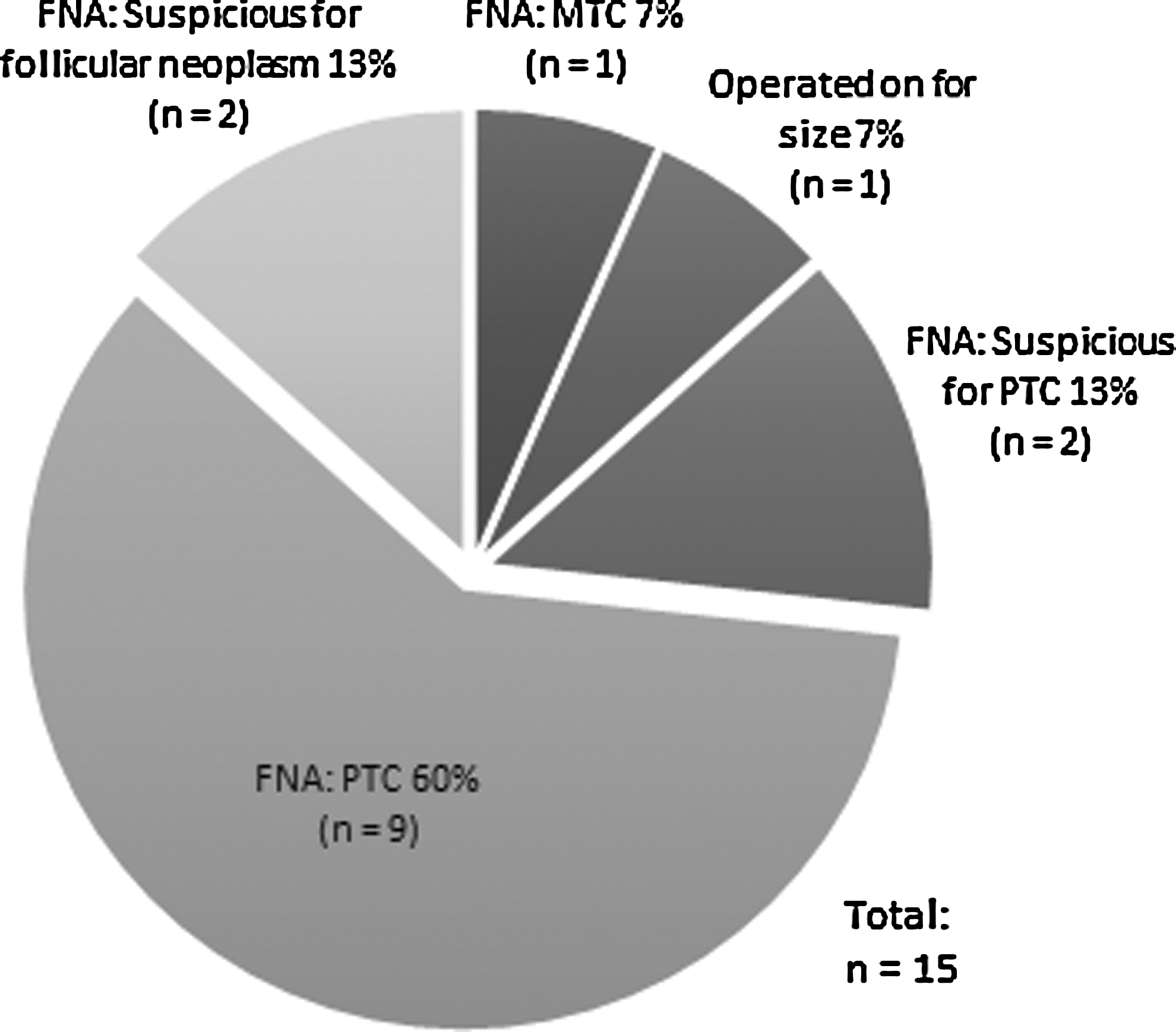
Mode of recognition of screening-detected thyroid cancer cases. Shown here are the 15 patients who were ultimately found to have thyroid cancer on final pathology, and their indication for surgery. The main mode of recognition was fine-needle aspiration biopsy.
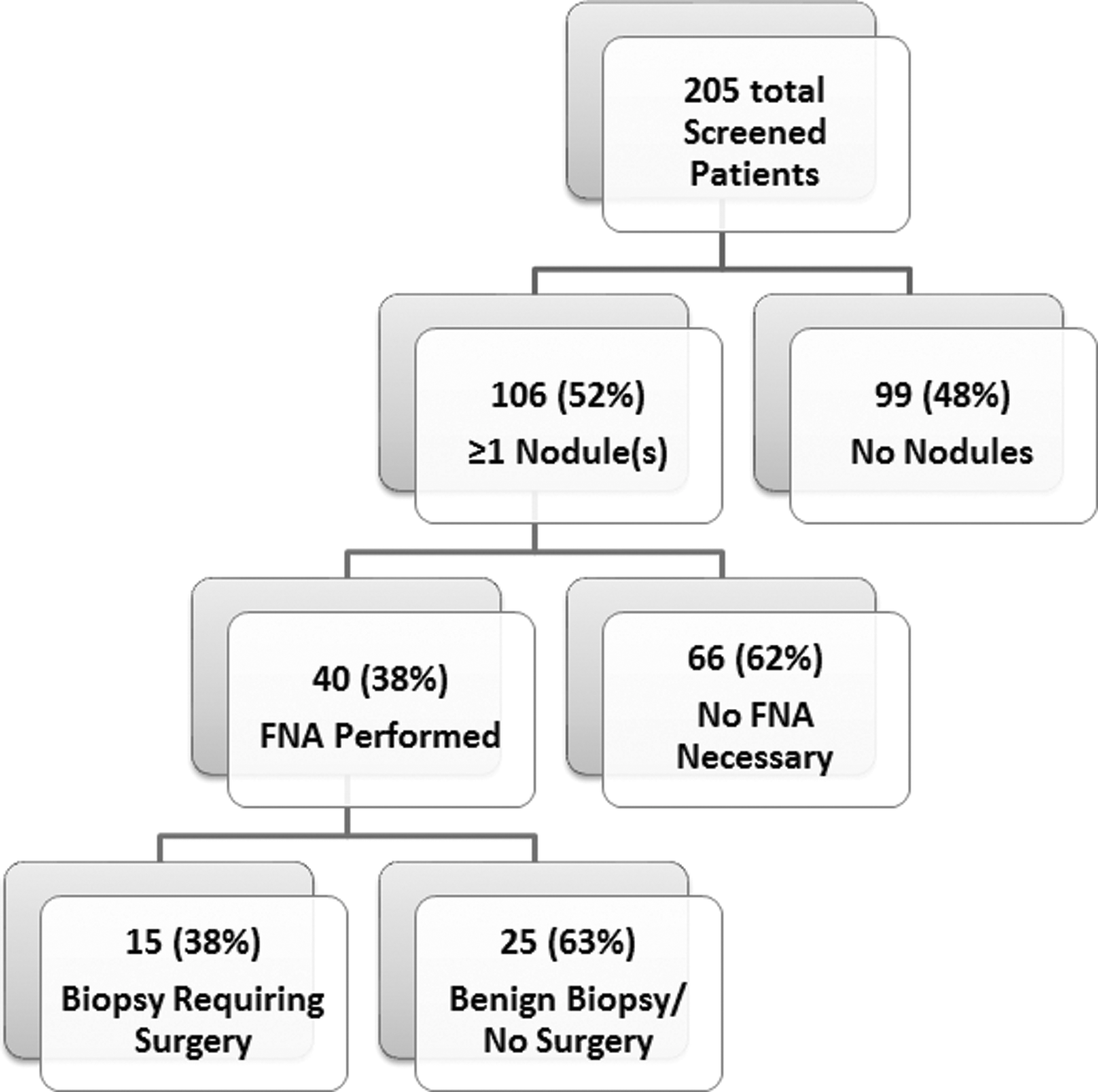
Nodule workup summary for screened cohort.
In total, 16 patients had thyroid disease (7.8%), including hypothyroidism, Graves' disease, and thyroiditis. Only two of these individuals were newly diagnosed through these screening visits; the remaining had known thyroid conditions.
SD thyroid cancer cases
These 15 cases constitute the SD cases, which were compared to the NSD cases. Mean age of thyroid surgery was 44 years (range 22–71 years), and 12/15 patient were female (80%). Only 2/15 (13%) of patients had a palpable mass on physical exam. Five of the 15 (33%) were symptomatic, but this was only upon specific soliciting of symptoms by the clinician; these were not presenting symptoms or chief complaints.
All but one patient underwent total thyroidectomy, three of these with lymph node dissection. One patient underwent a lobectomy, but final surgical pathology provided an indication for completion thyroidectomy. There were 14 cases of PTC, and five (36%) of these were identified as the cribriform-morular variant. The remaining case was a medullary thyroid cancer. The mean primary tumor size was 1.1 cm. Eight of the 15 cases (53%) were bilateral, and 11/15 (73%) were multicentric. Nine of 15 (60%) underwent radioactive iodine ablation after surgery. Twelve patients were stage I, one was stage II, one stage III, and one stage IV. No patients in this group experienced complications from the surgery. During a mean follow-up time of 17 months, there have been no recurrences or deaths in this screened group.
Relative risk of thyroid cancer for FAP patients
The period prevalence of thyroid cancer as found through this screening program was 15/206 (7.3%). A total of 206 patients were screened for a total of 7940 person-years. The absolute risk of thyroid cancer in FAP as found by thyroid screening was therefore 15 cases per 7940 PYO, or 189 cases per 100,000 PYO. This is compared to the age-adjusted incidence rate of 1.23 per 100,000 PYO for the general population (based on the most recent available SEER data for 2000–2010), taking into account this study's distribution of PYOs. The relative risk is calculated by the observed/expected ratio, 188/1.23, or 153. This statistic compares the risk of thyroid cancer in FAP patients as detected through the screening program with the risk of thyroid cancer in the general population.
Comparison of NSD cases with SD cases
Both groups demonstrated the same pattern of extra-intestinal manifestations (EIMs). The three most common EIMs seen were duodenal/gastric polyps (12/18 in NSD vs. 10/15 in SD), desmoid tumors (9/18 in NSD vs. 6/15 in SD), and osteomas (8/18 in NSD vs. 4/15 in SD). In terms of FAP diagnosis, in the NSD group, 12 were diagnosed clinically, and six underwent genetic testing. This is compared to the SD group, where 11 were tested to be APC-positive, and only four were diagnosed clinically. This likely reflects the recent increasing availability and usage of genetic diagnostic and confirmatory testing. There was, however, a different pattern of timing of FAP diagnosis and timing of thyroid cancer diagnosis. In the NSD group, two patients were found to have thyroid cancer before their diagnosis of FAP, and four other patients had their thyroid cancer and FAP diagnosed concurrently. This is compared to the SD group, where only one case of thyroid cancer and FAP was diagnosed concurrently. The rest of the cases were found to have thyroid cancer subsequent to their FAP diagnosis, as can be expected of a cohort undergoing screening. The singular case of concurrent diagnosis in a screening-cohort patient was due to the patient being referred to her first screening thyroid US appointment after discussion with colorectal colleagues, and she was found to have a 1.3 cm nodule that was found to reflect a PTC on cytology.
In order to compare SD cases with NSD cases, Fisher's exact test and the Mann–Whitney U-test were used to calculate significant differences. No differences were found between the two groups for sex (p=0.64), but age differed significantly between the two groups (p=0.0004). No differences were found for presence of symptoms (p=1) or palpable mass on exam (p=0.2419). There were no differences in rates of papillary pathology (p=0.4545), bilaterality (p=1), or multicentricity (p=0.4328) between the two groups.
In terms of severity of disease and treatment, the size of the primary tumor differed significantly between SD and NSD (p=0.04). The number of patients with positive lymph nodes between the two groups approached significance. Of note, pathology records were incomplete for two NSD cases and made no mention of lymph node positivity, and therefore they were excluded from the denominator for this finding (p=0.0691). The rate of complications also did not differ (p=0.2330), nor did the rate of recurrence/metastases (p=0.4886). The two groups were also comparable in terms of radioactive iodine ablation treatment (p=0.4875; see Table 2 for a comparison of TNM staging between SD and NSD cases). There also seemed to be no difference between the five SD cribriform-morular variant cases compared with the one NSD cribriform-morular variant case: the mean primary tumor size for the SD cribriform-morular variant was 1.36 cm compared with 1.3 cm for the NSD cribriform-morular variant case. None in either cribriform-morular variant group showed evidence of positive lymph nodes or metastases or recurrence (over a mean follow-up time of 14 months for SD, and a follow-up time of 69 months for NSD); none experienced complications.
SD, screening detected; NSD, non-screening detected.
Discussion
In the retrospective review of the database, 18 historical, or NSD, cases were found. Through the prospective screening program, a higher prevalence of thyroid cancer (7.3%) was found compared with those reported by other studies in the past (7,9,13). Under the screening program, FAP patients are 153 times more likely as someone in the general population to be found to have thyroid cancer. While the calculation grouped together male and female FAP patients, it is similar to the results of another study that reported female FAP patients as having 100–160 times the risk of a healthy individual (4,15). Van der Linde et al. calculated a relative risk of 23, but this was only with a sample of four FAP patients (5). Additionally, a higher rate of benign thyroid nodules (52%) than was expected was found for a cohort of this age distribution (M age=42 years). While benign thyroid nodules are common in the general population, with estimates ranging from 27% to 67%, the screened cohort seemed to have a greater prevalence (20,21). This was consistent with the existing literature on benign thyroid nodules observed on US in FAP patients (11,12). Overall, this evidence suggests that both thyroid cancer and benign thyroid disease in the FAP population may have been underreported in the older literature. Studies in the past relied on soliciting patient medical history and/or review of medical records in order to count cases of thyroid cancer. In contrast, for this study, all FAP patients were proactively screened, which allows for a more accurate report on the presence of thyroid disease in this specific population. The results of this study provide a more accurate epidemiologic characterization of thyroid disease in FAP than previous descriptions.
In order to determine the necessity of screening and appropriate long-term disease follow-up, SD cases were compared with NSD cases. While no difference in the sex ratio was found, there was a significant difference in age between the two groups. This is to be expected, given that screening will actively detect disease that may be indolent, slow-growing, or asymptomatic. There was no difference found between SD and NSD in terms of presence of symptoms or palpable mass on exam. This comparability of symptoms in both groups may be due in part to patients in the screening program being actively solicited for thyroid-related symptoms. There was no differentiation made between patients who agreed upon being specifically asked, compared with those who self-reported. For the SD cases, the mode of recognition of thyroid cancer and indication for surgery was reliant on FNA biopsies, which were very predictive of the final pathology.
In terms of pathology and foci of disease, the similarity between the two groups supports the fact that SD and NSD cases both consisted of the same clinical entity. The results are consistent with the literature, which also reports that the majority of thyroid cancer cases in this clinical setting are multicentric and bilateral (8). One notable point of difference between SD and NSD cases is the rate of reported cribriform-morular variant of papillary pathology in SD compared with NSD. This is a rare subtype estimated to comprise only 0.16% of all papillary cancers, but it is estimated to occur in one-fourth to one-third of all FAP-associated papillary cases (22,23). Consistent with this, this variant accounted for 36% of papillary cases in the SD group, and importantly, all cribriform-morular variant cases presented as PTC on initial FNA cytology. In comparison, only one case in the NSD group was specifically described as being a papillary cribriform-morular variant. The disparity between the rate of this pathologic variant in the SD compared with NSD groups is likely due to the fact that this particular pattern of histological characteristics was only named by Cameselle-Teijeiro and Chan in 1999, and 11 out of 18 NSD cases occurred before 1999 (24). Also, since the majority of the NSD cases were not performed at the authors' institution, it is not guaranteed that a rare subtype is recognized and part of standard reporting elsewhere.
Interestingly, FNA cytology in the screened/biopsied patients did not result in the finding of AUS or FLUS in any of the cases. This is unusual, as it differs from the distribution of Bethesda categories typical for the general population. The results do not provide the ability to explain why this is the case, except that all of the pathologists are experienced thyroid cytologists and the majority of these FAP cases were evaluated by multiple staff from the multidisciplinary tumor board. It is hypothesized that the disease pattern in the nodules detected demonstrates greater numbers of abnormalities than analogous disease in the general population. Regardless, this is an area of ongoing investigation as more information is collected regarding both new and follow-up FAP patients undergoing thyroid US. Now that this discrepancy in the distribution of pathologic diagnoses is apparent, vigilance is needed for any biopsies in this cohort that could be interpreted as AUS or FLUS.
Another point of interest in this study was the one patient with medullary thyroid cancer and FAP. To the authors' knowledge, there has been only one published case of medullary thyroid cancer in the setting of FAP (25). These authors proposed that either one genetic syndrome could be predisposing toward the other, or there is one underlying defect that predisposed toward both (25). There are currently no proposed molecular mechanisms for the intersection of these two genetic diseases. In the present patient, the medullary thyroid cancer was found to be 1.5 cm in greatest dimension, and was unilateral (left lobe). It was confirmed to be medullary with CAM 5.2, CEA, and calcitonin immunostains, which were all positive. The rest of the left thyroid lobe showed a focal mild increase in C-cells, and the right lobe was normal.
The mean tumor size was significantly larger in the NSD group (2.4 cm vs. 1.1 cm; p=0.04), and while positive lymph nodes approached significance, none of the other indicators of disease severity statistically differed (complications, rate of recurrence, and radioactive iodine ablation). This study is limited by the small sample sizes for both SD and NSD, which is simply a feature of this clinical entity. More importantly, surgical outcomes, thresholds for neck dissections, and guidelines for radioactive iodine ablation may vary from institution to institution, and this further precludes differences for these aspects of SD and NSD cases from being confirmed. However, a complication rate of 3/18 (including tracheostomy, hematoma, and vocal cord paralysis), recurrence in two cases, and one mortality does raise concern about the severity of disease when left to present itself. In general, screening in FAP seems to diagnose smaller-sized cancers that tend to require less radical therapy.
One aspect of the data that has not matured yet is the follow-up for both negative US and negative biopsies. Only patients with negative initial screening thyroid US and/or negative biopsies for a maximum of 48 months have been able to be observed to date. During this time, no patients who were initially found to have negative screens have presented with the disease on subsequent screening visits; that is, no false negatives have been found. Having a better estimation of the false negative rate in this cohort is an important goal of continued data collection. Continued follow-up will be important in allowing for more definitive conclusions in the future about possible differences in outcomes.
Some have argued that the increase in incidence of thyroid cancer in the past few decades may be in part due to changes in the diagnostic approach, leading to an increased detection of the disease (26,27). Some sources have pointed out that the increased incidence is mostly attributed to the discovery of subclinical cancers (27). Screening thyroid US would naturally be anticipated to discover cancers at a stage that may not garner clinical significance yet. Indeed, one of the main objectives of any screening program is to discover cancers at an earlier, more manageable stage. This may lead to a higher estimated prevalence of thyroid cancer in FAP than what was previously reported. Nonetheless, there are not enough data to conclude whether these subclinical thyroid cancers should be addressed, monitored, or ignored in this specific patient population, as they cannot be assumed to confer the same level of risk as their parallel entity in the general population. Regardless of the possibility of overestimation of thyroid cancer prevalence given more sensitive screening modalities, or more frequent use of these modalities, it remains important to follow these cases to characterize their disease trajectory and outcome.
Genetic disease registries collect pooled patient data, and with such information, surveillance protocols and disease management guidelines can be determined. A positive feature of this study is the large database that was mined, which is currently the largest, prospectively maintained registry in the world for FAP and other genetic colon cancer syndromes. Using this database, FAP status could be confirmed in all of the cases, both SD and NSD. This could not be done in some of the other published studies in the literature, which could have led to a dilution of the true rate of thyroid cancer in FAP as reported. The authors are also not aware of any other published studies on a prospective thyroid US screening program in this specific cohort. The value of this current analysis of the large registry is that it provides clear, objective findings to propose clinically reasonable and practical screening strategies to detect thyroid disease. The authors continue to study this clinical entity and do statistical modeling to determine whether US screening will ultimately improve mortality or morbidity from thyroid cancer in FAP patients.
The initial US was responsible for 91% of all detected nodules and 66% of biopsies, so at least one baseline thyroid US is recommended for all FAP patients, with sampling of nodules as per standard biopsy guidelines. Per the institutional policy of gastrointestinal colleagues at the authors' center for hereditary neoplasia, screening for patients suspected of having the FAP syndrome or having known relatives with FAP begins at age 16 with colonoscopy and genetic workup. Having a multidisciplinary team potentiates coordinated care, and therefore an initial screening thyroid US is suggested at the same visit. The frequency of screening thereafter will require data from longer follow-up periods and future analysis of the screening program cohort.
In an observational study, Wilding et al. measured the life expectancy of FAP patients before and after the establishment of a registry, and were able to show that the life expectancy increased from 56.7 years to 70.6 years (28). The authors attributed this increase to registry patients having access to improved, targeted care and regular colorectal/GI screening. While a direct causal relationship between registries and improved patient outcomes cannot be claimed, it is logical that patients who have access to optimized disease strategies, or who are managed based on current, evidence-based research, experience improved outcomes. With better management of their primary colonic disease, helped by regular endoscopic screening, FAP patients are enjoying longer, more normal life expectancies. More attention needs to be paid toward the extracolonic manifestations of this disease, and since both benign and malignant thyroid disease have been found to occur at a higher incidence in this group, screening in this cohort requires careful consideration. As shown, history and physical exam are insufficient means for detecting cancer. US is a noninvasive, inexpensive, fast, and effective modality for finding thyroid nodules, and provides some degree of risk stratification based on presence of some sonographic characteristics. Together with FNA, which was found to be reliably predictive of final surgical pathology in our group, these are feasible screening tools for both surveillance of thyroid nodules and cancer screening in FAP patients.
It is hoped that this summary of data from a large registry and with prospectively acquired clinical observations adds to the growing literature on the topic of FAP-related thyroid cancer risks and best management practices. It should be remembered that patients with FAP undergo lifelong surveillance for multiple medical conditions arising from this hereditary cancer syndrome. Unlike US screening in generally healthy populations that may represent undesirable detection of incidentalomas, the focus of US screening in FAP patients is to detect thyroid cancer—for which they are at higher risk—at a stage where earlier diagnosis may lead to appropriate treatment with fewer surgical complications. In this context, longitudinal thyroid US screening appears to be a logical and thoughtful clinical practice matched to the complexity of medical needs in the FAP patient population. While the current study does not suggest this practice be viewed as a clinical guidelines statement, it does encourage practitioners who routinely care for FAP patients to consider the benefits of this approach. Data from the ongoing large registry, and publications to date from other institutions, highlight the relevance of a multispecialty consensus statement on the care of FAP patients, and that the timing of this might be on the horizon.
Footnotes
Acknowledgments
The authors would like to thank Dr. Deborah Chute and Dr. John Kirwan for their expert input and manuscript review. This study was supported in part by a Medical Student Research Initiation Grant from the American Society of Colon and Rectal Surgeons.
Author Disclosure Statement
No competing financial interests exist.