
Abstract
Background:
Survivors of childhood cancer (SCC) who have received radiotherapy to the head, neck, and upper thorax are at higher risk of developing subsequent thyroid malignancies. As part of the post treatment long-term follow-up protocol, the current Children's Oncology Group guideline recommends surveillance by annual palpation; however, thyroid nodules are difficult to detect by physical examinations alone, and potentially malignancy-harboring nodules may be undetected. Since thyroid ultrasound is a sensitive and noninvasive procedure, it was incorporated in our institutional follow-up protocol. The aim of this study was to examine the outcome of ultrasound screening in this high-risk population. The following describes our experience from 2007 to 2013.
Methods:
A retrospective chart review was conducted on survivors enrolled in our follow-up program. SCC who have received direct or scattered radiation to the thyroid gland, and who were ≥10 years from the diagnosis of primary childhood cancer were considered to be at-risk.
Results:
Seventy-eight survivors met the inclusion criteria and were screened. Thyroid ultrasound detected thyroid nodule(s) in 46 patients (59%), 17 of which had nodule(s) between 5 and 10 mm (22%), and 15 patients had nodules ≥10 mm (19%). Fourteen patients (18%) underwent fine-needle aspiration biopsy. Six patients (8%) underwent surgery, and 5 (6%) had confirmed papillary carcinoma. At the time of the first ultrasound, thyroid nodules of various sizes were found. However, over time, these nodules demonstrated slow growth rates.
Conclusions:
Incorporation of thyroid ultrasound into routine follow-up of high-risk SCC may aid in the detection of thyroid malignancies that are not clinically apparent. The use of ultrasound allows detailed characterization of the thyroid nodule and reliable monitoring of nodule progression. In SCC without suspicious nodule(s), it may be reasonable to perform screening ultrasounds less frequently due to the slow growth rate of thyroid nodules. However, in those with suspicious features, surgical work-up resulted in the removal of a high number of malignancies, with few unnecessary surgeries and complications.
Introduction
I
To address the increased risk of thyroid malignancies in the SCC population, the Children's Oncology Group guidelines have recommended annual thyroid palpation for at-risk SCC (10). Although a convenient and non-invasive practice, thyroid palpation has low sensitivity, and may miss potentially malignancy-harboring nodules (11,12). Conversely, guidelines from major thyroid organizations in both North America and Europe are in agreement that more definitive tests may be needed in postirradiated patients (13). The American Thyroid Association (ATA), the European Thyroid Association, the American Association of Clinical Endocrinology, and the Associazione Medici Endocrinologi have advocated for closer monitoring of postirradiated patients with ultrasound (13). In particular, the ATA guidelines indicate that nodules ≥5 mm in a postradiation patient warrant high enough suspicion for additional investigations such as a fine-needle aspiration (FNA) biopsy (14,15). Therefore, there is conflict in the current literature on the best management and follow-up strategy of SCC for subsequent thyroid malignancies. Considering the high-risk nature of this population, testing beyond manual palpation may be beneficial.
Thyroid ultrasound is the gold standard of detecting thyroid nodules and malignancies. It provides detailed descriptions of thyroid nodules and is an important part of the diagnostic process. However, ultrasounds are not used as a routine screening procedure in the general population due to concerns for high rates of false positive findings and potentially unnecessary interventions in individuals with nonmalignant nodules. In the general population, thyroid nodules are very common. The prevalence is estimated to be 4–7% by palpation, and can be up to 19–67% by ultrasound depending on the age of the studied populations (16). Yet the prevalence of malignancy-harboring nodules remains relatively lower; approximately only 5% of all nodules may contain malignant neoplasms (17). Although some debates exist in the interpretation of thyroid cancer epidemiology, the general consensus is that ultrasound screening in the general population is unnecessary (18,19). Nonetheless, given the much higher risk for thyroid cancer in SCC populations, the use of ultrasound in the long-term follow-up remains a controversial clinical decision. There is little evidence regarding the natural history and screening outcome of thyroid malignancies in the SCC population to support or oppose its use.
Since the best practice of thyroid surveillance in the SCC population is unclear, our institution at the Children's Hospital, London Health Sciences Centre, incorporated routine thyroid ultrasound screening into our long-term follow-up “aftercare” program in 2007. Aiming to optimize the follow-up care, the goal of this study was to assess the outcomes and effectiveness of the use of ultrasound. The following is a description of our six-year experience.
Materials and Methods
A retrospective chart review was conducted on patients who are currently enrolled in the Pediatric Oncology Aftercare Program at the Children's Hospital in London, Ontario. This ongoing program provides long term monitoring for at-risk SCC for pediatric cancer–related late effects. For the monitoring of subsequent thyroid malignancies, a multidisciplinary team of nurses, pediatric oncologists, and otolaryngologists are involved in the work up process (Fig. 1). In 2007, we began screening with thyroid ultrasounds. Findings of a nodule containing suspicious features such as large size with one dimension measured ≥10 mm, poorly defined margins, irregular shape, microcalcifications, hypoechogenicity, solid or mixed solid/cystic structure, presence of vascularity as detected with Doppler flow, and/or pathologic lymph nodes were referred to an otolaryngologist for FNA and cytological analysis (13). Decisions for additional investigation and/or continued observation were made with the consideration of physicians' recommendations and the patient's preferences. SCC with no nodule or SCC with nodule(s) containing no worrisome features were followed with periodic ultrasounds at the discretion of the primary oncologist in the Aftercare Clinic.
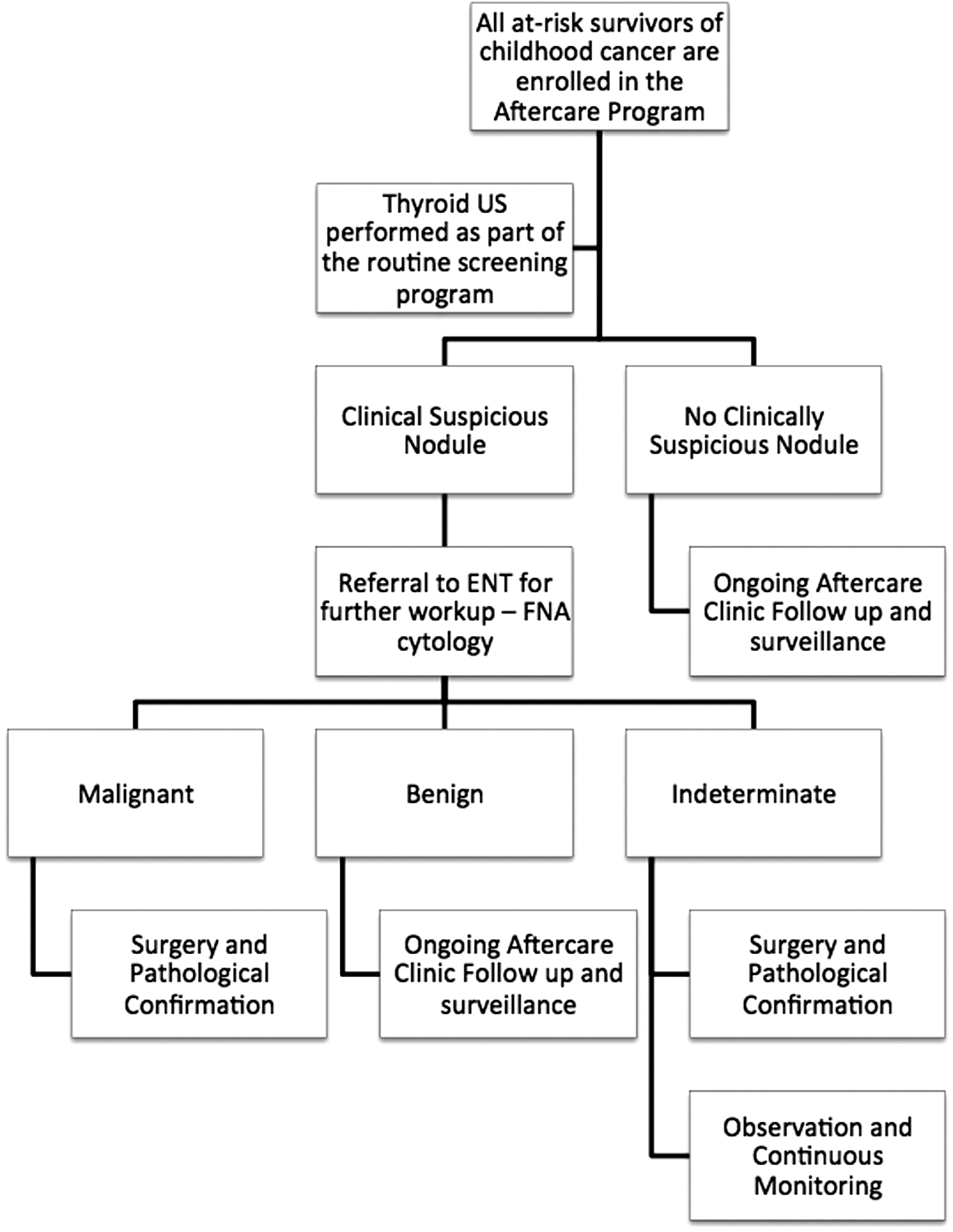
The long-term follow-up protocol for the monitoring of subsequent thyroid malignancy at the Children's Hospital, London, Ontario. At-risk survivors of childhood cancers (SCC) were screened with thyroid ultrasound. Individuals with suspicious findings were referred to an otolaryngologist for fine-needle aspiration biopsy. Individuals with indeterminate cytology can elect to have surgical work up or continued monitoring with additional ultrasounds.
Data collection
Patient information was gathered from hospital charts, including clinic notes, ultrasound reports, pathology reports, and the Aftercare Clinic database. The SCC were followed from the time of Aftercare enrollment to either the time of pathological confirmation of thyroid malignancy, or the most recent ultrasound screen. Statistical analyses were done using SAS statistical software to assess (1) the relationship between duration since radiation and ultrasound outcome, and (2) the progression of thyroid nodules over time. The institutional ethics review board at London Health Sciences Centre approved this study.
Patients
Several studies have defined thyroid malignancy risk differently. The current literature suggests the risk for subsequent thyroid malignancies peaks between 10 and 19 years following radiation exposure (4). Therefore, in our Aftercare program, SCC are considered to be at-risk if they were (1) treated with ionizing radiation while <19 years of age; (2) had radiation to the thyroid gland directly (spinal, mantle, neck, and total body radiation) or through scattered radiation (cranial, chest, and mediastinum); and (3) have been in remission for at least 10 years since the primary malignancy diagnosis. SCC were excluded if the patient was lost to follow-up or if the patient was diagnosed with thyroid malignancy within 10 years of primary malignancy diagnosis.
Radiation dosimetry
The radiation dosage was calculated by a radiation oncologist. The radiation received by the thyroid gland was estimated based on the patient's radiation history, including examination of port films, two-dimensional or three-dimensional dose calculations, and daily treatment records. As a general rule of estimation, the amount of radiation received by the thyroid gland was 100% of the documented dosage for mantle, neck, mediastinum, and total body radiation fields; approximately 80% of the indicated dosage for cranial-spinal radiations, and approximately 5% of the indicated dosage for cranial radiation. Due to the inherent limitation of patient records, other sources of external radiation such as computed tomography (CT) scans were not included in the calculation of total radiation received by the patient.
Statistical analysis
Statistical analysis was done by an independent statistician. Descriptive statistical analysis was done on the SCC demographics, primary malignancies, and treatments. Spearman rank correlation was used to examine the correlation between the size and number of thyroid nodules, and the duration between the first ultrasound and radiation therapy. A signed rank test was used to examine whether there was a significant nodule growth over time, and Kruskal-Wallis test was conducted to test difference in growth rate between nodules of different sizes. A p-value of ≤0.05 was considered to be statistically significant.
Results
A total of 100 SCC registered in the Aftercare program were eligible for the study based on the inclusion criteria. Of these patients, 23 were excluded from analysis according to exclusion criteria. In the remaining 78 SCC, thyroid nodules were detected in 43 survivors (55%). Thirty-two (41%) survivors had nodules ≥5 mm. In this group, 14 (8%) survivors underwent FNA cytology examination, while the rest elected to have serial ultrasound monitoring. On the cytology report, there was 1 case of papillary carcinoma, 11 cases of indeterminate cytology, and 2 cases of insufficient sampling. Surgery was performed in the 1 papillary carcinoma case, 4 out of 11 indeterminate cases, and 1 of the 2 insufficient sampling cases. The overall result showed 5 cases of papillary carcinoma, an overall 6% of all cases reviewed, 16% of those with high risk nodules (≥5 mm), and 36% of those who underwent FNA (Fig. 2).
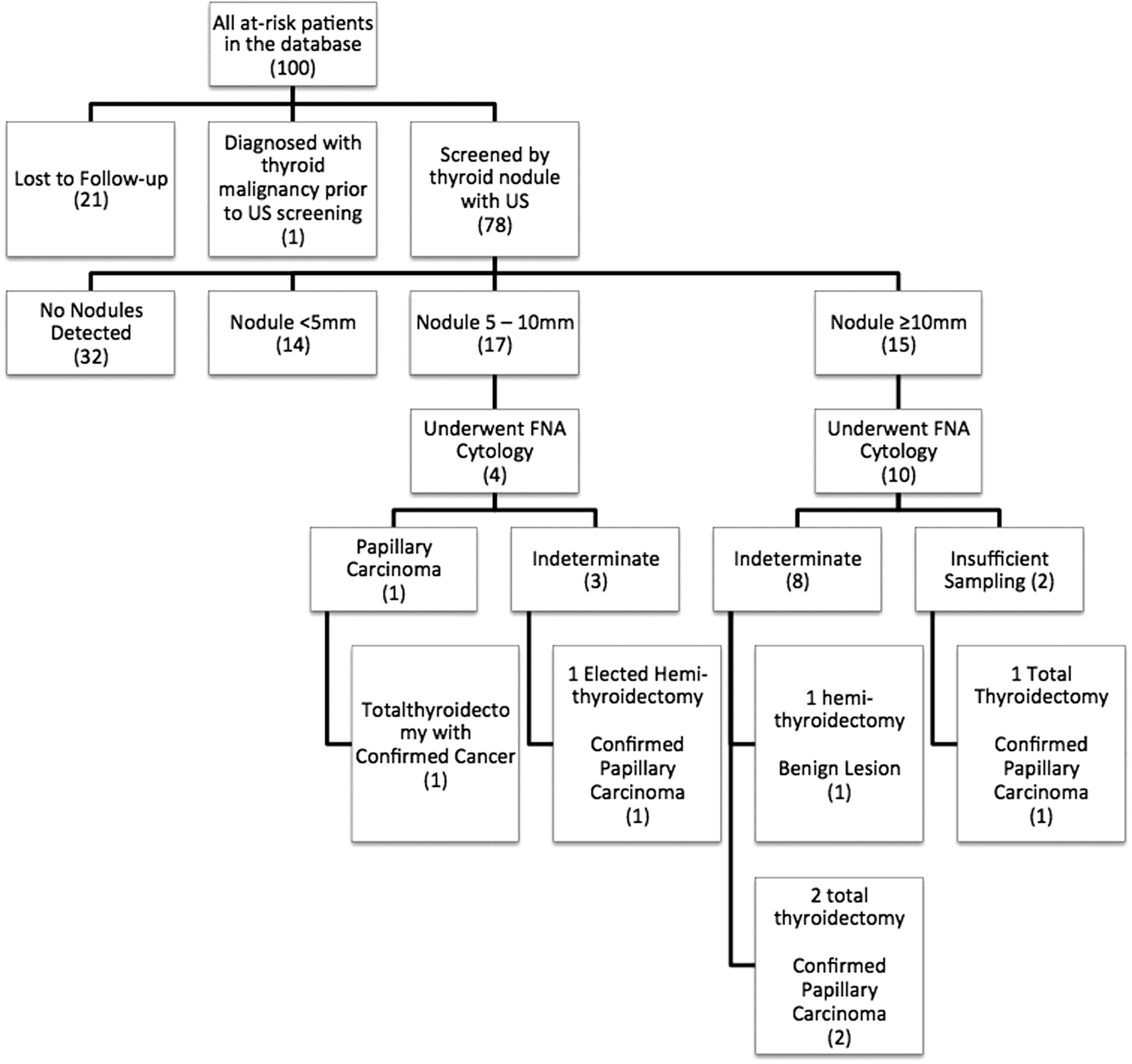
Ultrasound screening outcomes during a 6-year period. A total of 78 patients were included in the analysis. Nodules were detected in 46 (59%) of the cohort, including 32 (41%) with nodules ≥5 mm. Fourteen SCC underwent fine needle aspiration, 6 of which underwent surgery, and papillary carcinomas were detected in 5.
A summary of the patient demographics can be found in Table 1. The SCC in our cohort is composed of 34 (44%) females, and 44 (56%) males. On clinical follow-up, a variety of post-treatment late effects were found. Several endocrinopathies were diagnosed in this population, including several cases of hypothyroidism. A variety of primary malignancies were present in our group; the most common diagnoses were acute lymphoblastic leukemia 46 (59%), Hodgkin's lymphoma 10 (13%), and medulloblastoma 9 (12%). Review of the chemotherapy record showed 82% of SCC had a history of anthracycline and 40 (51%) had an alkylating agent as part of their treatment protocol. In accordance to the primary diagnoses, our cohort was treated with several radiation fields. The most common fields were cranial 37 (47%), cranial–spinal 15 (19%), mantle 10 (13%), and total-body radiation 9 (12%). The average estimated radiation dosage received by the thyroid gland was 817 cGy, and average age at which radiotherapy was initiated was 7.9 years old. Comparing SCC based on different thyroid nodule size (<5 mm, 5–10 mm, and ≥10 mm), individuals with larger nodules had higher numbers of primary cancer relapse, higher radiation dosage, and older age at radiation exposure (Table 2). However, our cohort size was insufficient to establish statistical significance for these factors. Comparison of SCC based on the radiation dosage showed that thyroid nodules were found at all levels of radiation. The size of the thyroid nodules increased with increased radiation exposure. However, there was still substantial risk for the development of thyroid nodules in individuals who have received <200 cGy (Fig. 3). Two of the 45 (4%) SCC who were exposed to radiation <200 cGy had confirmed malignancies and 12/45 (27%) had nodules ≥5 mm.
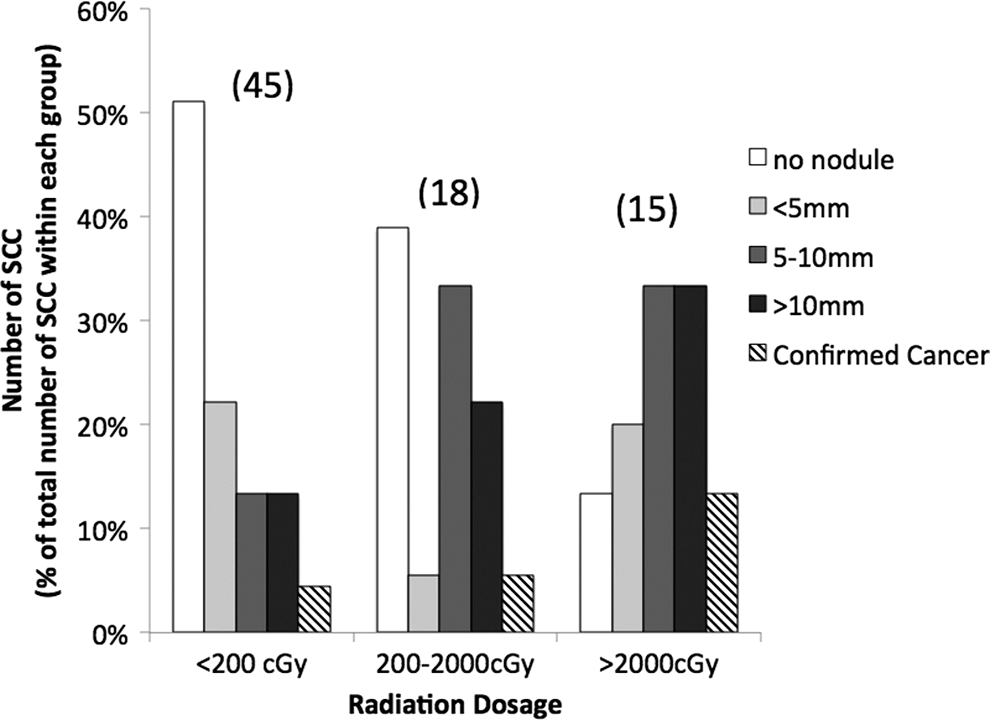
Relationship of radiation dosage and ultrasound screening outcome. The cohort is categorized into individuals who have received low (<200 cGy), mid (200–2000 cGy), and high (≥2000 cGy) levels of radiation. The y–axis represents the number of SCC as a percentage of the total number of SCC within each group. The total number of SCC with in the group is shown in the bracket above each column. Higher proportions of SCC developed larger thyroid nodules when exposed to higher levels of radiation. However, there was one case of confirmed malignancy, even in the low radiation group.
T4, thyroxine; TSH, thyrotropin.
ALL, acute lymphoblastic leukemia; ALM, acute myeloid leukemia.
A summary of the most recent ultrasound screening results can be found in Table 3. In the 6-year screening period, 58 (74%) of the cohort had ≥1 thyroid ultrasound. In keeping with the surveillance protocol, survivors with larger nodules were considered at higher risk, and were followed more closely with more frequent ultrasounds. These individuals with larger nodules also had higher numbers of suspicious sonographic features such as hypoechogenicity, complex and solid nodule, and presence of vascularity, which also contributed to the increased index of suspicion.
SCC, survivors of childhood cancers; US, ultrasound.
To examine whether the screening was initiated at an appropriate time following radiation, we analyzed the earliest ultrasound screening result. This first ultrasound (at an average of 16 years following radiation) showed a variety of thyroid nodule findings: solitary and multiple nodule(s) ranging between <5 mm and ≥15 mm were already present (Supplementary Fig. S1; Supplementary Data are available online at
As shown in Figure 2, 14 SCC underwent FNA cytology examination. Five patients underwent surgical workup due to patient preference despite ambiguous cytology results. A total of 6 SCC underwent surgery, a detailed description of these patients can be found in Table 4. During the thyroid nodule investigation process, no FNA complications were reported. Four of the five cases of ambiguous cytology resulted in diagnosis of papillary carcinomas. The remaining 1 case was a benign neoplasm. The thyroidectomy complication rate was minimal; only 1 case of transient hypocalcemia was reported, which was resolved at subsequent follow-up. Of the SCC who had indeterminate or insufficient FNA but did not undergo surgical work up, 7 out of 8 patients received additional U.S. monitoring of the thyroid nodules.
FHA, fine-needle aspiration.
Discussion
In our SCC cohort, the incorporation of thyroid ultrasound detected a large number of individuals with high-risk thyroid nodules and thyroid malignancies over a 6-year screening period (average 18.45 years since initial radiation). In post-irradiated patients, thyroid nodules ≥5 mm are considered to be high risk and are found in 32 (41%) of the cohort (14). In those who underwent surgery, 5 out of 6 had confirmed malignancies, yielding an overall cancer risk of 6% (average of 19.7 years since initial radiation). Similar to previous studies, this number is significantly higher than expected based on the data from the baseline population. In North America, according to the National Cancer Institute's Surveillance, Epidemiology, and End Result (SEER) Program and the Canadian Cancer Registry data, the estimated annual incidence is 12.2 and 14 per 100,000 for the United States and Canada respectively (20,21). Interestingly, our observed cancer rate was also higher than those previously reported in large SCC cohort studies without ultrasound screening. The CCSS's most recent data reported 119 secondary thyroid malignancies in 12,157 patients; the British Childhood Cancer Survivors Study reported 50 in 17,980 patients; and a similar group in France reported 52 cases in 2,907 patients (7,5,1). Therefore, our result suggests that the use of ultrasound increased the detection of thyroid malignancies in a population that is already at significantly higher risk compared to the baseline population.
Our observation is supported by the few existing reports that examined the use of ultrasound as a screening tool: in a recent report, Kelly and colleagues observed 4 cases of papillary carcinomas in 36 ultrasound-screened patients (22). This high incidence was also found in a European study, where 5 papillary carcinomas were found in 129 screened SCC (23). Similarly, an earlier prospective study of 95 ultrasound-screened patients have identified thyroid nodules in 44% of survivors, and identified 1 case of malignancy (24). Therefore, the incidence of thyroid malignancies may be higher than previously observed in large studies where ultrasound screening was not used. Furthermore, it is important to note that our reported value may be an underestimate of the true cancer rate in our cohort. Survivors who had ambiguous cytology results who elected conservative management and ongoing observation may be harboring additional malignancies.
While ultrasound screening may not be suitable for the general population, it may be appropriate for the SCC. As shown in our data, the incidence of thyroid nodules/malignancies far exceeds that of the baseline population. Therefore, this high risk may justify the need for closer monitoring, without the concern for overt detection of benign nodules. Indeed, this is the current consensus among major thyroid societies; thyroid ultrasound should be employed as part of the routine monitoring workup.
Several studies have characterized the risk factors associated with the development of subsequent thyroid malignancies. The large CCSS cohort found several risk factors, including high radiation dosage, female sex, early age of radiation exposure, and chemotherapeutic drugs (4,9). The observation of a dose–response relationship was particularly interesting due to the plateauing effect around 2000–2500 cGy (4). Our data is not in conflict with this previous study. Although a higher incidence of nodules and malignancies were observed at high radiation dosages, relatively high risks still exist in survivors exposed to low levels of radiation (<200 cGy). This suggests that even individuals who received scattered radiation to the thyroid gland—such as cranial irradiation—may be at risk and require long-term thyroid follow-up and baseline screening. Our observed risk at low radiation level may be partly attributable to the chemotherapeutic medication history of our cohort. In a recent report, it has been suggested that alkylating agents and anthracyclines are associated with a 2.4- and 1.8-fold increase in thyroid cancer risk in individuals with <2000 cGy of radiation (9). Both classes of chemotherapeutic agents are commonly used during the primary cancer treatment protocols for the pediatric malignancies in our study population.
A detailed analysis of the surgical results showed favorable surgical outcomes. All surgeries were preceded by FNA without complications. Five of the surgical cases were indeterminate or insufficient on cytology, and only one case was benign. This malignancy yield is considered to be on the higher end relative to the baseline population, where a malignancy rate of 6%–60% has been reported depending on the subtype of the indeterminate cytology (28 –30). Furthermore, it is noteworthy that 2 out of 5 confirmed cancer cases are from thyroid nodules ≤1 cm, a size that is difficult to detect by manual palpation alone. Thyroid palpation has low sensitivity, and may only detect 10–41% of the thyroid nodules (11). In one study, it was found that even large nodules (≥1.5 mm) could be missed during physical examination (12). Therefore, ultrasound offers a more reliable detection method as it can detect and measure nodules that are <5 mm. In all surgical cases, the complication rate was low and in keeping with the known risk in the literature (31). Only one case of transient hypocalcemia was noted, and this complication is likely attributed to the more invasive nature of the thyroid malignancy and the surgery, as nodal invasion was present.
While reports have consistently described the increased risk of thyroid malignancies associated with childhood radiation, to the author's knowledge, there are no studies of the natural history of thyroid nodules in the SCC population. Therefore, it is unknown when the screening program should be initiated and how frequently the screening tests should be done. Different studies have reported an increase in risk of malignancy between 5 and 15 years following primary cancer (32,4). The SCC in our cohort began ultrasound-screening ≥10 years after completing the therapy for primary cancer. At the time of the first ultrasound (average of 16.5 years from radiation therapy), a range of nodules were already present, including a number of large, high-risk nodules. However, this risk did not increase within our studied period. Therefore, early baseline screening of these individuals may provide valuable information regarding risk level and allows for future comparisons.
The thyroid nodule growth rate was also analyzed. Statistically, an overall minimal growth rate was found. However, it may be prudent to establish a growth trend through multiple ultrasound evaluations, as there was a large standard deviation in our data, including several individuals with fast growing nodules. Because ultrasounds characterize the size and features of nodules precisely, any nodule growth can be monitored reliably with a comparison with previous exam(s). Although it is debated what constitutes a clinically significant increase in nodule size (14,33), information from the ultrasound evaluation can aid the clinical decision-making process. For instance, a large increase in nodule size may prompt additional investigation such as FNA, whereas a modest change may provide relief of anxiety associated with the risk for a potential cancer and avoid unnecessary procedures. In those who are regarded as low-risk individuals, significant nodule growth may not be present until years later. Therefore, these individuals may be observed at longer intervals. Additionally, established high-risk sonographical features such as: hypoechogenicity, solid or mixed cystic composition, the presence of vascularity, the presence of irregular borders, and the presence of microcalcification are also crucial in the determination of nodule management and are clinically useful in the risk assessment process (13,14,34 –36). While additional studies on the natural history of the thyroid nodules in the SCC populations are needed to fully establish the threshold for surgical intervention, thyroid ultrasound provides important information for clinical decisions.
Several limitations exist in our study. Due to the nature of the SCC population, our sample is small and may not have enough power to establish statistical significance. Since all SCC were enrolled in the ultrasound screening protocol, no control group exists for outcome comparison. And lastly, due to the retrospective nature of the study, and limited access to survivor medical history, other forms of external radiations, such as CT scans, were not accounted for. It has been reported that CT scans are a significant source of exposure and can increase the risk of leukemia and brain tumors (37). Therefore, in individuals with low levels of external radiation treatment, the number of CT scans may play an important confounding role.
In conclusion, high rates of thyroid nodules and malignancies were detected via ultrasound in our study. Surgical workup of these individuals resulted in a high yield of malignancies with low rate of complications and unnecessary surgeries. We found that although the majority of detected nodules showed slow growth rate over time, a large number of high-risk nodules were already present at an average of 16 years following radiation. Therefore, early screening may be useful in providing baseline characterization that dictates aggressiveness of future follow-ups. Taken together, these results suggest that screening ultrasounds provide valuable information to aid clinical decisions in this high-risk population, and the current oncology guideline recommendation for follow-up via palpation alone may be in need of revision. The inclusion of ultrasound as part of a routine or baseline work up may be beneficial in providing more information for patient care. However, due to the limitations of our study and the limited knowledge of the natural history of thyroid nodules in the SCC population, future research is needed fully establish these notions. Additionally, ongoing follow-up of these patients for longer duration will be needed to substantiate the benefit of ultrasound screening in SCC and determine whether this early detection significantly impacts the morbidity and treatment outcomes of this unique population.
Footnotes
Acknowledgments
The authors would like to acknowledge the Mach-Gaensslen Foundation of Canada for the research funding in support of this project. We would also like to thank the administrative staff of the Aftercare Long-Term Follow up Clinic at the Children's Hospital of Western Ontario for the data support.
Author Disclosure Statement
No competing financial interests exist.