
Abstract
Background:
Rebound thymic hyperplasia (RTHP) is not an uncommon finding after radiation or chemotherapy in patients with various malignancies. However, there are limited case reports of this phenomenon after radioactive iodine ablation therapy (RIAT) in differentiated thyroid cancer (DTC). The goal of this study was to evaluate the incidence, patterns, and factors affecting RTHP after RIAT using 18F-FDG PET/CT.
Methods:
The study design was a retrospective review of 2550 patients (568 men, 1982 women; age 13–79 years) who underwent FDG PET/CT imaging after total thyroidectomy and RIAT from June 2009 through June 2012. Patients were divided into four age-related subgroups. Overall incidence, age-related incidences, and sex distribution were evaluated in patients with thymic FDG uptake on PET/CT (RTHP+). The correlation between incidence of RTHP and age was assessed using the Cochran–Armitage trend test. The Wilcoxon rank–sum test and multiple regression were applied to investigate the effect of applied dose of radioactive iodine (RAI) and age on the incidence of RTHP. Correlations of standardized uptake value (SUV) and thymic volume with age and morphologic type were also evaluated.
Results:
Overall incidence of RTHP after RIAT was 1.49%, and all of the RTHP+ patients except one were female. The Cochran–Armitage trend test revealed significantly decreased incidence from the second to fifth decade (8.84%, 1.74%, 0.98%, and 0.39% respectively; p<0.001). In each age-related subgroup, the RAI dose was significantly higher in the RTHP+ than RTHP− group (p<0.001), while there was no difference in RAI dose in RTHP+ patients among age-related subgroups (p=0.838). SUVmean and SUVmax of RTHP revealed no meaningful correlation with RAI dose or age. There were no differences among morphologic patterns of RTHP in age distribution and ablation dose.
Conclusions:
RTHP after RIAT showed a strong female predominance, despite the higher administration dose of RAI in male patients. Although the decreased incidence of RTHP after RIAT with age is similar to the pattern of RTHP induced by other causes, the fact that older patients, even sixth decade patients, can present with RTHP after RIAT is noteworthy in the management of DTC.
Introduction
T
Several conventional imaging modalities such as plain radiography, ultrasound, computed tomography (CT), as well as 123I and 131I whole body scans (WBS) play important roles in the management of patients with thyroid cancer. However, these anatomic imaging tools are not perfect and have certain limitations. Currently, FDG PET/CT is widely used for evaluation of recurrence and treatment effect as well as initial staging of various malignancies because of its metabolic imaging ability, and this modality may be rapidly applied to thyroid cancer (3 –5). FDG uptake reflects the glycolytic activities of cells, and malignant cells usually have strong FDG uptake due to vigorous anaerobic glycolytic activity (6). However, many benign conditions also display strong FDG uptake, which can cause false-positive PET/CT findings in oncologic applications (7). In patients with thyroid cancer, increased FDG uptake in the anterior mediastinum may be challenging to interpret. Both primary malignancy and metastatic lesions involving this area can reveal increased FDG uptake, but benign conditions such as rebound thymic hyperplasia (RTHP) can also display high FDG uptake and mimic malignant conditions (8).
RTHP may be triggered by stressful conditions (9) such as chemotherapy, radiation therapy, burns, and surgery (10). Radioactive iodine (RAI) therapy after thyroid surgery is one such cause, although available references are limited (11). To date, except for several case reports, there has been little information about both RTHP and FDG PET/CT findings related to radioactive iodine ablation therapy (RIAT). Furthermore, to the best of our knowledge, there is no large population study of these topics. Therefore, we aimed to investigate the age-related and overall incidences, morphologic patterns, and factors affecting RTHP in 2550 patients with thyroid cancer who underwent surgery and RIAT.
Materials and Methods
Patients
A total of 2550 consecutive patients with thyroid cancer who underwent 18F-FDG PET/CT after bilateral total thyroidectomy and RIAT from June 2009 through June 2012 were retrospectively reviewed (M:F=568:1982, median age±interquartile range (IQR)=46±13 years). Of the 2550 patients, 44 displayed an FDG-avid mass in the upper anterior mediastinum on FDG PET/CT. Inclusion criteria for positive RTHP (RTHP+) were as follows: a well-defined mass in the anterior mediastinum on contrast-enhanced CT (CECT) images, visually detectable 18F-FDG activity of the lesion higher than that of the adjacent aortic arch, no aggravation of the initially detected lesions on follow-up PET/CT or 131I-WBS, and no change in unstimulated serum thyroglobulin (Tg) level. The minimum acceptable period of follow-up was one year. Exclusion criteria included masses with infiltrating margins, masses invading adjacent structures including the sternum and chest wall (n=2), and conglomerated multiple enlarged nodes with strong FDG uptake in the anterior mediastinum (n=4).
Finally, 38 patients (M:F=1:37, median age±IQR=31±16.5 years) were included in the RTHP group (RHTP+). The remaining 2506 patients who exhibited no significant upper anterior mediastinal mass or 18F-FDG uptake on 18F-FDG PET/CT scan, and the excluded patients (n=6), were allocated into the control group (RHTP−). The time interval between PET/CT imaging and RIAT was compared between the RTHP+ and RTHP− groups to eliminate bias caused by differing follow-up times. The median interval±IQR of the RTHP+ and RTHP− groups was 189±67.25 and 194±22.00 days respectively. The time intervals of the two groups showed no statistically significant difference, as confirmed by the Wilcoxon rank–sum test (p=0.462). The study was approved by the institutional review board, and the need for written informed consent was waived.
FDG PET/CT imaging
All patients fasted for at least 6 h before the injection of 5.18 MBq/kg (0.14 mCi/kg) of 18F-FDG, and serum glucose levels of all patients were lower than 150 mg/dL. Whole-body PET with non-CECT for attenuation correction was performed consecutively 60 min after the injection of 18F-FDG, using a dedicated PET/CT system (Biograph TruePoint 40; Siemens Healthcare). CECT was performed after intravenous injection of 50 mL iopromide (Ultravist 300; Bayer HealthCare) at a rate of 1.5 mL/s to obtain fusion images of PET and CECT. The parameters for CECT were 120 kVp, 170 effective mAs, 0.5 s gantry rotation, 1.2 mm collimation, and 0.05 mm intervals. Acquired 18F-FDG PET images were reconstructed using the ordered-subset expectation maximization method under the condition of two iterations and 21 subsets. Fusion of reconstructed PET and CECT data was performed for image interpretation.
Image analysis
PET/CT images of 38 patients in the RTHP+ group were reviewed using both P-mod software (PMOD Technologies) and PACS (GE Healthcare). A region of interest (ROI) was drawn in each transaxial slice image showing FDG uptake in the anterior mediastinum, and the volume of the thymus was obtained by summation of these areas. The standardized uptake value (SUV) was measured for each ROI, and then maximum SUV (SUVmax) and mean SUV (SUVmean) were obtained for each volume of interest (VOI); these values were automatically calculated by the P-mod software. The morphologic pattern of FDG uptake in the RTHP+ group was classified into four types: (a) typical inverted V-shape mass with a linear or concave outer margin, (b) inverted V-shape mass with a lobulated or convex contour, (c) mixed type of types a and b, and (d) asymmetrically located mass (Fig. 1). Image analysis in the RTHP− group was not performed because this group had no positive findings except for the six excluded cases showing FDG-avid malignant lesions.
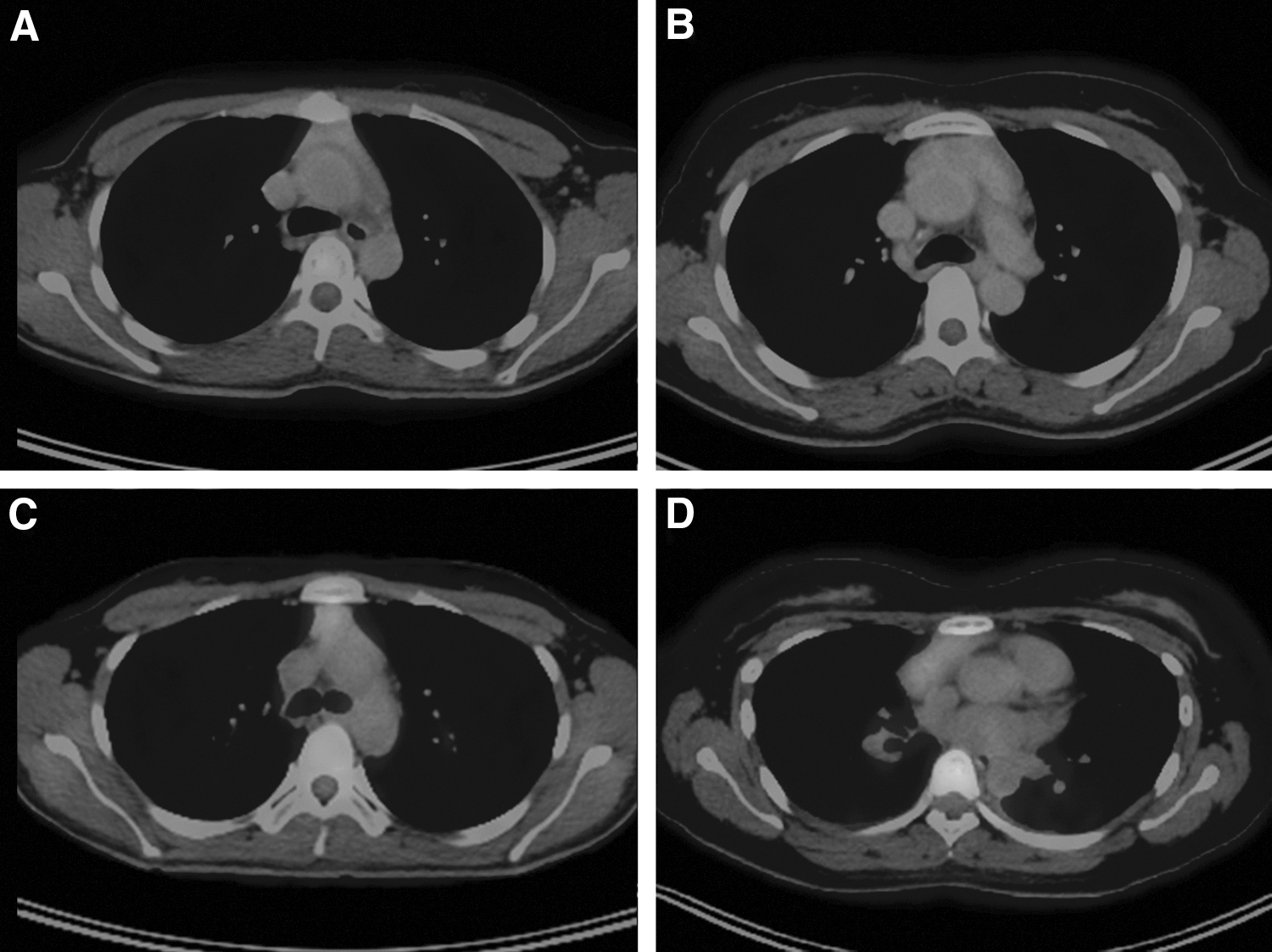
Four morphologic subtypes of rebound thymic hyperplasia: type a (
Data analysis
Overall incidence, age-related incidences, and sex distribution of RTHP were obtained. For the age-related incidences, RTHP+ patients were subdivided into four age groups by decades. Two teenagers (18 and 19 years) were merged into the group of twenties, and the final age distributions of the four subgroups were 18–29, 30–39, 40–49, and 50–59 years. Incidences of RTHP of these four subgroups were evaluated by the Cochran–Armitage trend test to assess the age-related change in RTHP incidence. We also attempted to determine whether any differences existed in the median age and administered dose of RAI between RTHP+ and RTHP− patients. These calculations were executed in the age-related subgroups as well as the overall groups. To identify age-related differences in RAI dose, the RAI dose was compared among the age-related subgroups in RTHP+ patients only using the Wilcoxon rank–sum test.
The volume (cc), SUVmax, and SUVmean of the FDG-avid mass in the anterior mediastinum were selected as candidate factors indicating the severity of RTHP. Multiple regression analysis was performed to determine correlations between these three severity factors of RTHP and the two factors of age and morphologic type.
Results
Incidence of RTHP according to age and sex
The overall incidence of RTHP after RIAT was 38 of 2550 patients (1.49%), and the incidences of the four age-related subgroups were 8.84% (16/181) in the second to third decade, 1.74% (11/631) in the fourth decade, 0.98% (7/711) in the fifth decade, and 0.39% (4/1027) in the sixth decade. The Cochran–Armitage trend test revealed a significant reduction in RTHP incidence as patient age increased (p<0.0001). In terms of sex distribution, 37 of the 38 RTHP patients were female. The ages of the RTHP+ and RTHP− groups were 31±16.5 years and 46±18 years respectively. The Wilcoxon rank–sum test revealed a statistically significant age difference between these two groups (p<0.001).
Dose of RAI and RTHP
The therapeutic dose of RAI (median±IQR) in the RTHP+ group was 180±65 mCi, which was significantly higher than that of the RTHP− group (100±100 mCi). This result was validated by the Kruskal–Wallis test (p<0.001). Repeated comparison of the same data in each age-related subgroup confirmed a higher administered dose of RAI in RTHP+ patients. These results are summarized in Table 1. However, comparison of RAI dose in RTHP+ patients among the age-related subgroups did not reveal any statistical difference with the Kruskal–Wallis test (p=0.838). Although the same test performed in RTHP− patients showed significant differences (p=0.0001), post hoc testing in the RTHP− cohort revealed no differences between the third and fourth decades (p=0.504) and the fifth and sixth decades (p=0.222).
Median±IQR.
RAI, radioactive iodine; RTHP, rebound thymic hyperplasia.
Three severity factors and morphologic patterns of RTHP
Overall results of three factors selected as severity indexes of RTHP, including thymic volume, SUVmean, and SUVmax, were 29.29±23.62 cc, 2.13±0.38, and 2.88±0.78 respectively (median±IQR). In terms of morphologic pattern, the most common was the inverted-V shape, which was subdivided into three patterns according to outer margin—linear or concave outer margin (type a: 22 of 38), convex to lobular outer margin (type b: 7 of 38), and partly lobulated outer margin (type c: 7 of 38). The remaining two cases showed asymmetrically located masses (type d).
There were no differences among the four morphologic subtypes of RTHP in the three severity factors, as well as in age and ablation dose. The only difference detected was thymic volume between morphologic types a and b (Table 2). Thymic volume, SUVmax, and SUVmean in the four age-related subgroups of RTHP+ patients are summarized in Table 3. Multiple regression analysis to evaluate the correlation between these three indicators of severity of RTHP and the two factors age and morphologic pattern of RTHP revealed no statistical significance (p>0.05).
Morphologic subtype; †significant difference in volume between types a and b.
All data are presented as median±IQR.
Age-related subgroup.
All data are presented as median±IQR.
Discussion
This retrospective study investigated characteristics of RTHP after RIAT. A strong female predominance and an association with younger age were found, and four morphologic types were identified.
RTHP, which means regrowth of the atrophied thymus, has been not uncommonly reported in children and adolescents after various stress conditions such as chemotherapy, radiation, and surgery (12). Since an early report of RTHP after cessation of corticosteroid treatment in a pediatric patient (13), RTHP has also been observed in the recovery phase after thermal burns (14) or surgery of great vessels. As the reports of RTHP have accumulated, various modalities for imaging RTHP have been proposed. For example, Cohen et al. demonstrated RTHP on plain radiography and CT after chemotherapy in a 3-year-old boy with Wilm's tumor in 1980 (15). Subsequently, histology confirmed RTHP was reported in an adult cancer case in which RTHP was detected on CT (16), and in a patient with lymphoma in whom an anterior mediastinal mass was detected on MRI after chemotherapy (17). In 1979, Jackson et al. confirmed thymic uptake of 131I in a patient who underwent thyroid surgery by autoradiography (18). Later, Michigishi et al. described 131I-WBS, and demonstrated strong thymic uptake on histologically confirmed hyperplastic thymic tissue after RIAT for thyroid cancer (11). After additional reports regarding thymic uptake of 131I (19,20), Godart et al. reported intense uptake of FDG in thymic hyperplasia after thyroid surgery (21). However, these are all case reports, and there has been no large population study of RTHP related to RIAT.
The incidence of DTC continues to increase (22). Although the overall survival rate of thyroid cancer is excellent, recurrence rate of this malignancy is known to vary depending on the severity of disease, and can range from <5% to >50% (23). Further, many of the patients with a higher rate of recurrence have an impaired prognosis (2). Among the diverse diagnostic tools for thyroid cancer, 18F-FDG PET/CT has recently played a growing role in staging, treatment monitoring, and recurrence evaluation of thyroid cancer patients with noniodine avid, persistently elevated Tg levels, and other risk factors, similar to other malignancies (4,5). The usefulness of 18F-FDG PET/CT for thyroid cancer has been reported in cases with negative 131I-WBS, despite elevated serum Tg levels. However, another study reported that 18F-FDG PET findings can alter the management of patients exhibiting both negative 131I-WBS and undetectable Tg levels, similar to Hürthle cell carcinomas and poorly differentiated thyroid cancers (3). Although the application of FDG PET/CT in thyroid cancer is still limited, considering the rapid progress of PET technology, the role of PET/CT in this disease will expand.
In clinical practice, FDG PET/CT plays an important role in the detection of distant metastatic lesions, as well as local recurrences in patients with thyroid cancer. However, the interpretation of FDG-avid lesions encountered in the anterior mediastinum during follow-up of thyroid cancer can be challenging because these lesions may represent many possible malignant conditions such as extensive nodal metastases, unexpected viable residual or recurrent disease, and even double primary malignancies including lymphomas and thymic tumors (8). In addition, it is also very important to exclude the possibility of benign conditions such as RTHP to avoid futile management, including surgical resection or external beam radiation, as well as high-dose RAI therapy. Although many RTHP lesions show the typical inverted-V shape, there are some variations. Thus, understanding the incidence, affecting factors, and morphologic patterns of RTHP after RIAT may facilitate the accurate interpretation of PET/CT with findings of FDG-avid lesions in the anterior mediastinum.
The thymus grows from birth to reach its peak weight at puberty, then gradually becomes atrophied with fatty replacement (24). Physiologic uptake of FDG by the thymus is commonly seen in children before puberty, up to the age of 13 years, but this finding is not normal in adults. The present study cohort included only eight teenagers of which two were RTHP+ and both older than 13 years (18 and 19 years). Thus, the possibility of age-related physiologic uptake in our population was considered very low.
The cause of RTHP is diverse and includes treatment with RAI. However, incidence, age and sex distributions, and affecting factors of RHT after RIAT have not been clearly defined. According to our results, the overall incidence of RTHP was approximately 1.4%, which is significantly lower than that of a previous study carried out by Jerushalmi et al. (25); this resulted from differences in age distribution and the cause of RTHP. The upper age limit in the previous study was 40 years, and total fatty involution of the thymus occurs by this time. However, the median age of our study population was 46 years, which is significantly higher than that of Jerushalmi et al. (M age=26.2 years) because approximately 40% (1027/2550) of thyroid cancer cases in our study group occurred after 40 years of age. Considering the cause of RTHP, the study by Jerushalmi et al. included diverse diseases such as lymphoma, sarcoma, melanoma, and cervical and colon cancer, while our study was focused on a single disease. Treatment options varied among diseases in the previous study, while a single treatment protocol—RIAT after total thyroidectomy—was applied in our study subjects.
Previous reports have shown that RTHP is more common at a younger age, and our study results support this finding. The median age of the RTHP+ group (31±16.5 years) was lower than that of the RHT− group (46±18 years), and the difference was statistically significant. In age-related incidences of RTHP in the four subgroups, the youngest age group, aged <29 years, showed the highest incidence (8.84%), and the older decade groups revealed rapidly decreasing incidences as age increased. As a result, the oldest age group (50–59 years) revealed a very low incidence of RTHP (0.39%). Considering the fact that there was no significant difference in RAI dose among the age-related subgroups of RTHP+ patients, patient age is one of the most important factors related to incidence of RTHP after RIAT, as it is in RTHP with other etiologies. It is noteworthy that the incidence in old age, although very low, is not zero. This means that both clinicians and nuclear medicine physicians should be mindful in the interpretation of PET/CT and management of thyroid cancer in patients of all ages after RIAT.
In terms of sex distribution, the higher prevalence of thyroid cancer in female patients is well known; our study group showed a similar sex distribution (M:F=1:3.49). However, the predominance of female RTHP+ cases was extremely strong, and all but one of 38 cases were female. This is an exceptional result considering that the age and sex distributions in our study cohort are similar to those of other reported data about thyroid cancer. Furthermore, our study group received a higher median dose of RAI in male (115 mCi) than female (100 mCi) patients. The statistical difference was confirmed by Mann–Whitney U-test (p<0.0001). Therefore, female patients appear to be more susceptible to developing RTHP after RIAT than male patients. Although this result may be controversial because of the small number of positive cases, further study of different reactions to RAI according to sex is warranted.
The most common pattern of RTHP was the inverted-V shape, but some cases presented with asymmetric masses and the outer contour differed among the inverted-V-shaped lesions. Therefore, we classified the 38 RTHP cases into four categories and investigated correlations with SUV and thymic volume. The study results revealed no significant differences in SUV among the four morphologic types of RTHP, and that type a had a significantly smaller volume compared with type b. However, these results are questionable because of the small number and uneven distribution of cases in each morphologic type. Further study is needed to evaluate the usefulness of the morphologic pattern of RTHP in differentiating this condition from other pathologic lesions.
Three candidate factors proposed to be indicators of the severity of RTHP—that is, thymic volume, SUVmax, and SUVmean—were compared with age and morphologic type by multiple regression analysis to evaluate the correlations among these factors. However, contrary to expectation, no significant result was found. This indicates that volume and SUV may not be suitable surrogate markers of severity in RTHP. However, further study is necessary because of the small number of cases used to generate this result.
The exact time of onset of RTHP after RIAT and the duration of RTHP remain intriguing issues in clinical practice. However, the evaluation of these topics could not be performed because of the retrospective study design, and because routine follow-up with PET/CT was only carried out once, approximately six months after RIAT, according to our institutional protocol. In addition, this protocol is not routinely used at all other institutions. Thus, a multicenter study with various PET/CT follow-up schedules will be helpful to elucidate these questions.
There are several limitations in the present study. First, this was a retrospective study, and there might have been bias in patient constitution or uncontrolled factors. Second, RTHP was not histologically confirmed because tissue confirmation of RTHP requires invasive biopsy techniques. Third, the number of RTHP cases was relatively small, even with the large population of 2550 subjects, because of the low incidence of RTHP. Thus, certain subgroup analyses failed to attain sufficient reliability. However, despite these limitations, this study reveals useful information regarding the characteristics of RTHP after RAIT.
In conclusion, age is the most important influencing factor for the development of RTHP after total thyroidectomy and RIAT in patients with thyroid cancer. The strong female predominance of RTHP despite a higher administration dose of RAI in male patients is an intriguing result, and further study is necessary to elucidate the genetic or molecular background for this finding. Although a robust decrease of the RTHP incidence in older patients with thyroid cancer is reported in this study, the fact that older patients, even those in their fifties, can present with RTHP is noteworthy.
Footnotes
Acknowledgment
This study was supported by a faculty research grant from the Yonsei University College of Medicine for 2011 (6-2011-0070).
Author Disclosure Statement
No competing financial interests exist.