
Abstract
Background:
Differentiated thyroid cancer (DTC) is the most common endocrine malignancy. In recent decades, the incidence has been increasing, largely due to increased detection of patients with low-risk or very low-risk DTC. According to European Thyroid Association and American Thyroid Association guidelines, radioiodine (RAI) thyroid remnant ablation is not indicated in very low-risk patients, while its role is still debated in low-risk patients. Accordingly, risk stratification of DTC patients is pivotal when deciding for or against RAI ablation. Presently, risk stratification is based on pTNM staging integrated with clinical parameters. The aim of our study was to evaluate the relationship between location of malignant thyroid nodules within the thyroid gland and the presence of loco-regional and/or distant metastases in patients with pT1a-pT1b DTCs.
Methods:
We reviewed the records of 246 patients (214 women, 32 men; female-to-male ratio 6.7:1) affected by unifocal DTC ≤2 cm, who had undergone RAI thyroid remnant ablation (activity ranged 555–4588 MBq) after levothyroxine withdrawal or after recombinant human TSH (rhTSH) stimulation. The majority of the patients (91.5%) were affected by papillary thyroid carcinoma.
Results:
Metastases were discovered by posttreatment whole-body scintigraphy in 29 out of 246 (11.8%) patients. In patients with metastases, malignant thyroid nodules were located in the right lobe (14/123, 11.4%), left lobe (7/95, 7.4%), and isthmus (8/27, 29.6%). The prevalence of metastases was significantly higher in patients with DTC located in the isthmus, compared to other sites (χ2=9.6, p=0.002).
Conclusions:
Our data show for the first time that a location of a thyroid cancer in the isthmus is an additional risk factor for RAI avid metastatic disease in pT1a-pT1b DTC patients, regardless of the presence or absence of other risk factors.
Introduction
T
DTC incidence has been increasing in the last few decades, with a large prevalence of small tumors (≤2 cm), probably due to improved detection of subclinical disease by ultrasonography (US) and fine-needle cytology (4). Accordingly, DTC-related mortality has not increased (3).
In DTC patients, (near-) total thyroidectomy is the treatment of choice followed by adjuvant radioiodine (RAI) therapy for thyroid remnant ablation (TRA) (5 –8).
Recently, the role of TRA has been revised, and according to European Thyroid Association (ETA) (9) and American Thyroid Association (ATA) guidelines (10), it is not indicated in very low-risk patients (i.e., pT1aN0M0), while it is suggested in patients with pT1b-2N0M0 DTCs with no aggressive histology (e.g., tall cell, insular, columnar cell carcinoma) or vascular invasion. Thus, in these patients, the choice to perform TRA or not is based on risk factors (e.g., age, sex, histological variants). During routine clinical observation, we observed that RAI avid lymph node metastases were often observed on the posttreatment whole-body scintigraphy (pWBS) when the malignant nodule was located in the isthmus.
Accordingly, we evaluated if the location of the tumor within the thyroid gland is related to the occurrence of RAI avid loco-regional or distant metastases in a series of patients with pT1a-pT1b cancers.
Materials and Methods
We retrospectively reviewed the records of 1159 patients (884 females, 275 males, aged 16–86 years; female-to-male ratio 3.2:1; median age: 53 years) affected by DTC and admitted to our Nuclear Medicine Unit (at “G. Martino” University Hospital of Messina, Italy) during the last 5 years (from January 1, 2008, through December 31, 2013). For the present study, we selected 246 out of 1159 patients (21.2%) affected by unifocal DTC ≤2 cm (all pT1a or pT1b; 214 women, 32 men, aged 19–75 years; female-to-male ratio 6.7:1; median age: 47 years). Exclusion criteria were 1) histological diagnosis of pT2-pT4 DTC, 2) presence of lymph-nodal or distant metastases at the time of recruitment; 3) age ≤16 years. Two hundred twenty-five patients (91.5%) were affected by papillary thyroid carcinoma (PTC), while 21 (8.5%) had follicular thyroid carcinoma (FTC).
Patients underwent TRA after adequate stimulation by endogenous thyrotropin (TSH; hypothyroidism induced by 5-week levothyroxine (LT4) withdrawal, n=183, or 74.4%) or by intramuscular administration of recombinant human TSH (rhTSH) 0.9 mg daily for two consecutive days (n=63, or 25.6%).
Before TRA, all patients underwent neck US, measurement of serum TSH (chemiluminescent immunoassay, Beckman; normal values in our laboratory, 0–4.2 mIU/L), thyroglobulin (Tg; immunoradiometric assay [Cisbio]), and anti-thyroglobulin antibodies (Tg-Ab; chemiluminescent immunoassay, Beckman; reference values in our laboratory <100). Furthermore, in the 183 hypothyroid patients who were treated after thyroid hormone withdrawal, RAI thyroid uptake was evaluated 24 hours after Na-131I tracer activity (1.8 MBq) administration, as elsewhere described (11).
Radioiodine activities administrated for TRA ranged from 555 to 4588 MBq (15–124 mCi; median 2753 MBq, 74.4 mCi). pWBS was obtained 5–7 days after RAI administration using a double-headed gamma camera (Millennium VG, GE Medical System) equipped with high-energy low-resolution parallel hole collimators. Whole-body images were obtained from head to proximal thighs (anterior and posterior views, matrix 256×256, magnification: 1, acquisition time: 10 cm/min).
The study was integrated by static images of neck and thorax (anterior and posterior views, magnification: 1; matrix: 256×256; frame time: 900 seconds) obtained with and without a jugular radioactive mark (employed to better localize the foci of RAI uptake compared to the upper mediastinum).
In order to obtain a better target/background ratio, patients were required to drink at least 1.5 L of water and take laxatives drugs 1 day before the examination.
Statistical analysis
Numerical data are expressed as median and interquartile difference, and categorical variables as number and percentage. The examined variables did not present normal distribution, as verified by the Kolmogorov Smirnov test; consequently, the nonparametric approach was used.
For each parameter, we performed statistical comparisons between the isthmus and the right or left lobe by means of the Mann–Whitney test. The same test was applied to compare the age parameter between patients, with and without metastasis, and between male and female patients. To assess the association between categorical variables (such as sex, age, histological variant, tumor localization, metastases localization, and Hashimoto thyroiditis), the chi-square test and relative significance were estimated. Odds ratio was estimated to evaluate the risk for patients with an isthmus lesion to develop metastasis compared with patients with malignant thyroid nodule located in the right or left lobes.
Logistic regression models (12) were estimated in order to assess the possible dependence of metastases (in terms of presence or absence) on some potential explicative variables, such as age, sex, histological variant, tumor size, malignant thyroid nodule position, and concomitant Hashimoto thyroiditis. First, we estimated univariate models; subsequently, a multivariate model was analyzed, inserting only the significant variables that resulted from the univariate approach.
Statistical analyses were performed using SPSS 11.0 for Windows package; p<0.05 was considered to be statistically significant.
Results
RAI avid metastases were detected in 29 out of 246 (11.8%) patients (24 women, 5 men, aged 22–74 years, median age: 47 years). Metastases were confirmed by targeted neck US and/or computed tomography with and without enhancement. Serum values of Tg on LT4 therapy were undetectable in all patients with metastases before RAI treatment and low at the time of RAI therapy (median 2.1 ng/mL, range 0.4–11; p=0.08). In patients with metastases, administered activity of Na-131I ranged from 1110 to 4588 MBq (30–124 mCi; median, 2526 MBq [68 mCi]). In all patients with metastases, the histology was papillary, and 16 (55.3%) had a pT1a lesion. Characteristics of the patients with metastases are reported in Table 1. The median age of female patients with metastases was significantly higher compared with male patients (50.1 vs. 33.2 years, respectively; p=0.009).
pWBS, posttreatment whole-body scintigraphy; PTC, papillary thyroid cancer; RL, right lobe; LL, left lobe; I, isthmus; UM, upper mediastinum; L, lung; RLN, right lateral neck; LLN, left lateral neck; CC, central compartment.
In patients with metastases, malignant thyroid nodules were located in the right lobe (14 of 123, 11.4%; 13 women, one man; median age, 47.5 years, range 23–74 years; histological variant: classic variant, n=5; follicular variant, n=8; sclerosing variant, n=1); left lobe (7 of 95, 7.4%; seven women; median age, 49 years, range 40–67 years; histological variant: classic variant, n=3; follicular variant, n=4); isthmus (8 of 27, 29.6%; five women, three men; median age, 46.5 years, range 22–70 years; histological variant: classic variant, n=6; follicular variant, n=2); no metastases were found in the patient with DTC located in the pyramidal lobe (Fig. 1).
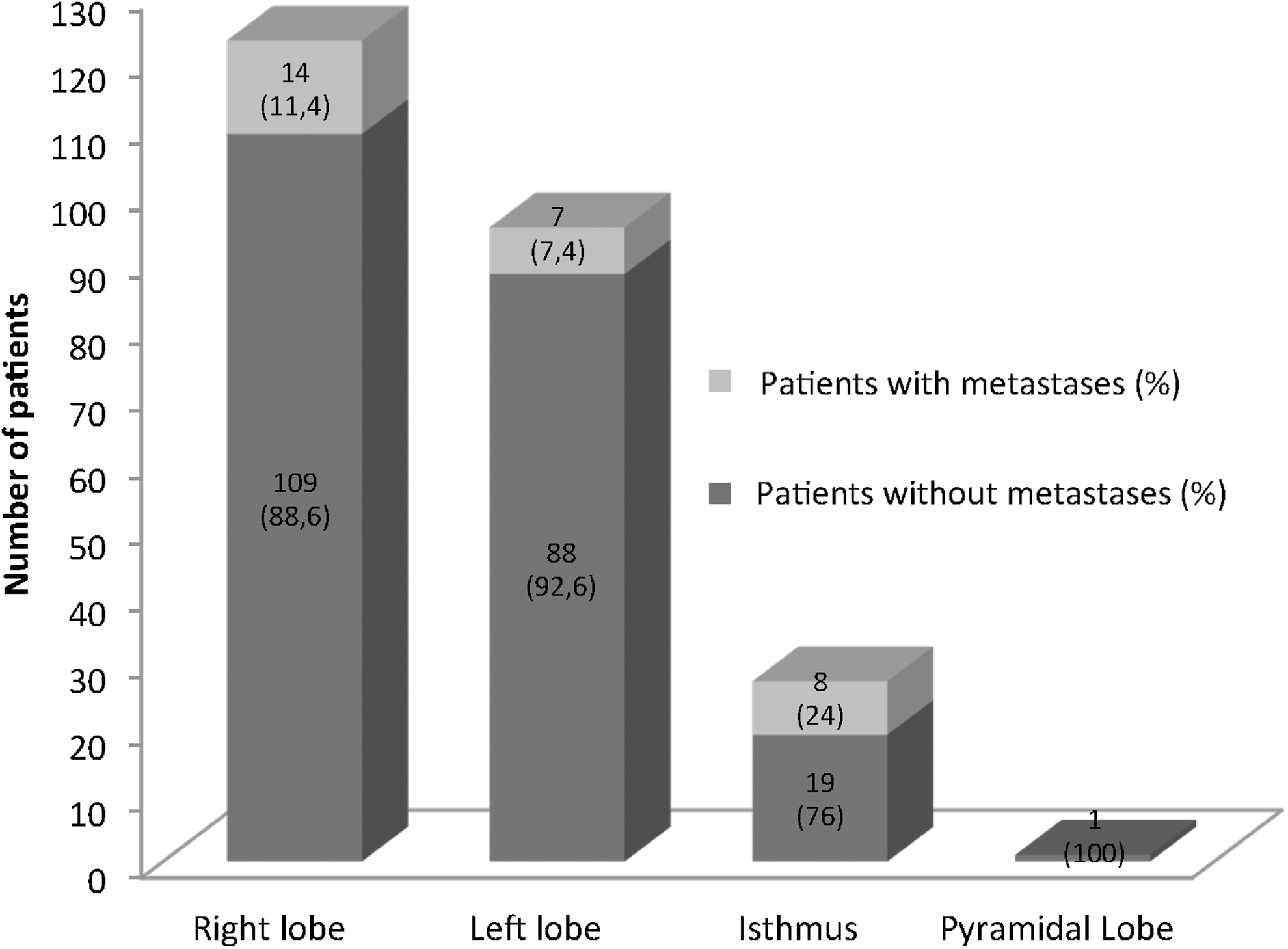
Position of the cancers in our series of unifocal pT1a or pT1b PTC patients with and without metastases.
Concurrent Hashimoto thyroiditis occurred in six women affected by metastatic PTC (21.4%, p=0.155). The median age was 48 years, range 40–67 years. In these patients, the malignant nodule was located in the right lobe (three patients) or left lobe (three patients).
All patients with metastases, except for one with bilateral lung metastases, had lymph node metastases. Three of these patients (two women and one man)—two with central compartment involvement and one with right lateral and central compartment involvement—also had lung metastases that were unilateral in two of them. The lymph node metastases were located in the upper mediastinum (n=5), left lateral neck (n=4), right lateral neck (n=5), and anterior central compartment (n=14) (Figs. 2 and 3). Overall, 30 metastatic lesions were detected at pWBS, two patients harboring metastases both in the right and left regions of the neck and in the anterior central compartment.
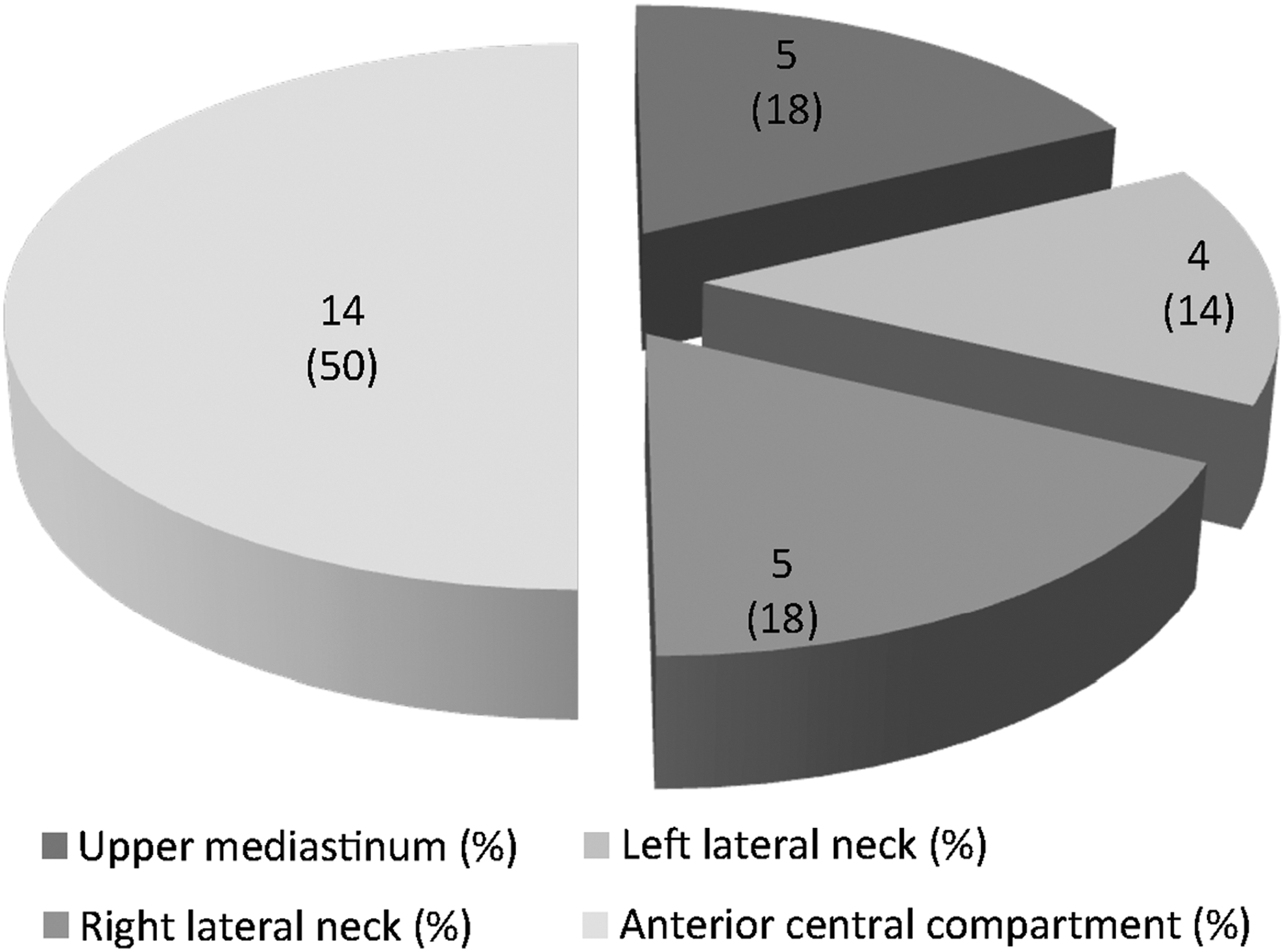
Metastatic lymph node localization in the studied patients.
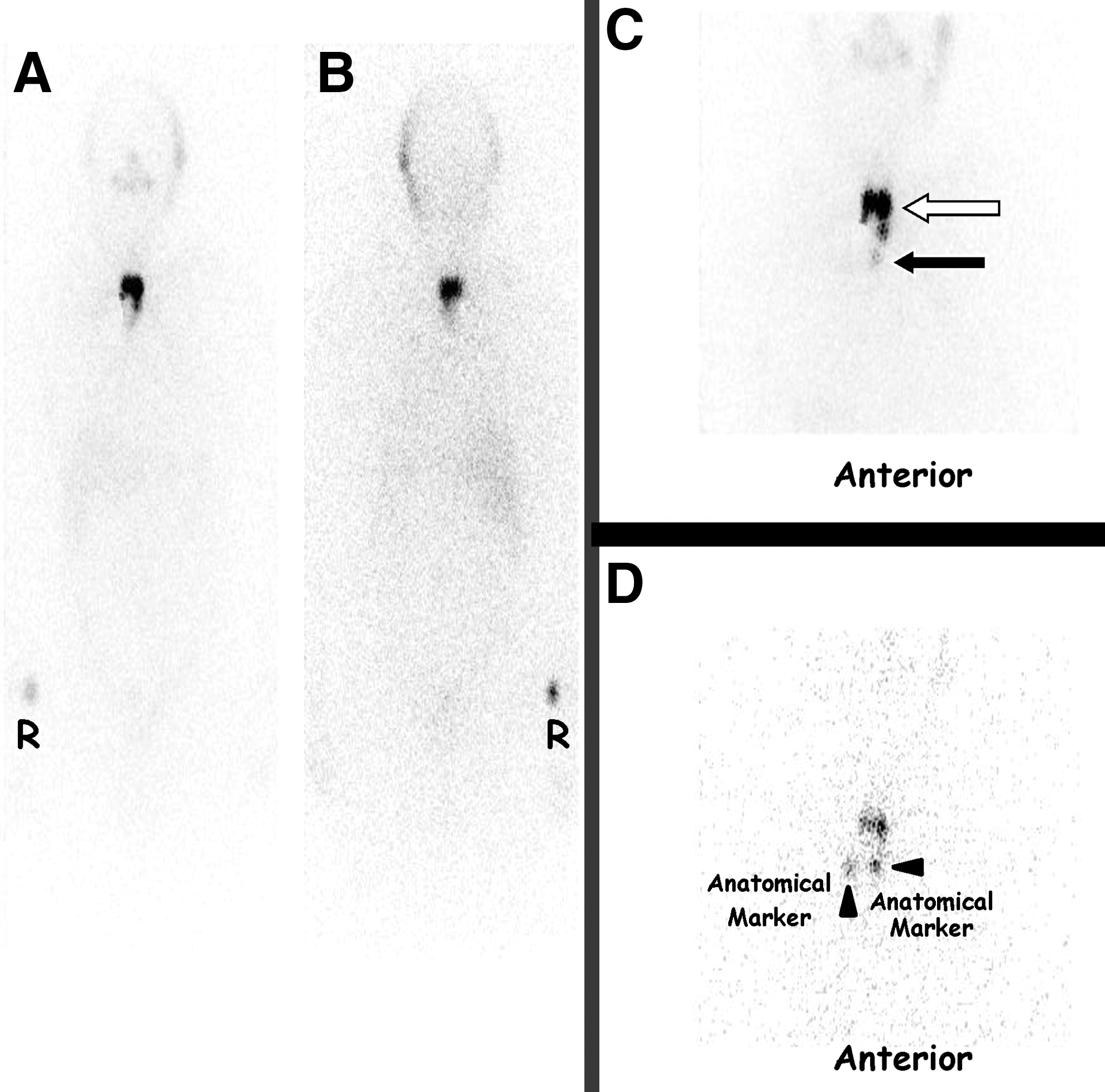
Thirty-three-year-old man, pT1a-PTC (classic variant) located in the isthmus.
Four out of twenty-nine (13.7%) patients with metastases were treated after rhTSH stimulation (euthyroid state). We did not observe significant differences in the capacity to detect metastases between the two stimulation strategies used to treat the patients (p=0.19).
In patients with metastases, the median size of the malignant nodules located in the isthmus was significantly smaller than that of the malignant nodules located in the left lobe (7 and 12 mm, respectively; p=0.04), while there was no significant difference between the median size of the malignant nodules located in the isthmus compared to that of the malignant nodules located in the right lobe (7 and 10 mm, respectively; p=0.388).
The prevalence of metastasis was significantly higher in patients with PTC located in the isthmus compared with patients with malignant thyroid nodules located in the right lobe (p=0.01) or left lobe (p=0.02). The prevalence of metastases remained significantly higher in patients with PTC located in the isthmus compared with those with malignant thyroid nodules located in other sites (left or right lobes) considered together (χ2=9.6, p=0.002) regardless of age, sex, histological variant, Hashimoto thyroiditis (p=0.009) and size (p=0.03) (logistic multivariate regression analysis).
Finally, we noted a significant prevalence of the classic variant of PTC in the isthmus lesions (6 of 8 or 75%, p=0.001).
Discussion
Currently, according to ATA and ETA guidelines, TRA is not indicated in very low-risk cancer patients (pT1aN0M0, TNM 7th edition), while there are conflicting data regarding its use in low (pT1bN0M0) risk cancer patients; thus, “selective use” is suggested. However, these patients may develop recurrent disease or metastases (often loco-regional) during follow-up (7).
Our results confirm that the frequency of both loco-regional and distant metastases in very low-risk or low-risk patients is not negligible (about 10% of all our DTC patients). Of note, the majority of these patients (55.3%) had pT1a lesions, and thus were affected by a so-called microcarcinoma in which, according to actual guidelines, TRA would not have been indicated. These patients would have had occult disease that probably would not have increased the risk of disease-specific mortality (10) or of distant metastatic spread [even if some authors have shown the contrary (13 –18)], but would have had negative effects on patients' outcomes, reducing quality of life.
This is an important point as, today, the mean age of the patients at diagnosis is lower than in previous years, as also demonstrated by our data in which the median age of patients with metastases was 47 years without significant differences between women and men. The histological type was papillary in all our patients with metastases, and the median size of the lesion was about 10 mm. Five of them (17.2%) harbored a lesion less than 5 mm. About 60% of these patients had an isthmus lesion, and these lesions were the smallest.
Currently, in low-risk patients the “selective use” of TRA suggested by the ATA guidelines is based on evaluating the risk factors of the individual patient. Thus, it is important to have the highest number of parameters to evaluate and reduce the likelihood of underestimating the clinical risk of individual patients as much as possible. The common risk factors taken into account are sex, age, tumor size, and histological variant (10). To date, the location of the cancer in the gland has not been taken into account as an additional risk factor because there are no available data.
This is the first study to evaluate the relationship between topography of the malignant thyroid nodule in the thyroid gland and associated risk of metastases.
In our cohort, the prevalence of metastases was significantly higher in patients with isthmus lesions compared with patients with right or left or pyramidal lesions. Taking into account that isthmus lesions are not frequent (19,20) (about 11% in our series), the risk of developing metastases in patients with isthmus lesions is about 39% higher than in other patients (odds ratio=3.95), although the majority of our patients had the classic variant of PTC, which is commonly considered the least aggressive variant.
Isthmus lesions are more insidious than those located in the lateral lobes, also due to the tendency to metastasize to the lymph nodes of the central compartment and upper mediastinum (21) (100% in our patients). Metastases to levels VI and VII (Robbins's levels) can be difficult to detect using common imaging studies (18,22,23) both before and during surgery as well as in the follow-up due to their small size and position.
In all our patients, the neck US performed both before and 3 months after surgery was falsely negative, and the serum Tg value (on LT4 therapy and off LT4 therapy) was undetectable and low (compatible with the presence of thyroid remnant only), respectively. This latter fact was probably linked to the limited involvement of the lymph nodes (i.e., micrometastasis) that frequently occurs when metastatic disease involves the central compartment lymph nodes (24).
Thus, as often happens in very low-risk or low-risk patients, metastases are only demonstrated by pWBS (7), such as in our patients.
The exact reason why cancers in the isthmus spread more easily compared to lesions located in the left or right lobes is unknown. We believe that the thickness of the isthmus may play an important role in this phenomenon.
Conclusion
In line with recent data from the literature (7), our results show that the frequency of both loco-regional and distant metastases in very low-risk or low-risk patients is not negligible. In patients with isthmus lesions, even if classified as very low or low-risk, the risk of metastatic disease is significantly higher than in patients with malignant nodules in the lateral lobes. Thus, in such patients, we suggest performing TRA routinely, followed by pWBS.
In conclusion, we first demonstrate that the isthmic position of malignant thyroid nodules represent a significant independent risk factor for metastatic disease in patients affected by very low-risk or low-risk cancers. However, the retrospective design of the present study may be a limitation and a possible selection bias. Further, prospective studies on a larger series of patients will be necessary to confirm or refute the routine use of TRA in patients with pT1a and pT1b tumors in the case of an isthmic location of the cancer.
Footnotes
Author Disclosure Statement
The authors disclose no conflict of interest, and no funding was received for this work.