
Abstract
Background:
Dyslipidemia is an important global health problem, particularly in the elderly population. Traditionally, the high prevalence of dyslipidemia in elderly people is considered a “natural condition.” Notably, subclinical hypothyroidism (SCH) is one of the most important risk factors for dyslipidemia. Few studies have assessed whether SCH plays a role in the increase in age-related dyslipidemia. This study aimed to explore the association between SCH and lipid profiles in different age groups.
Methods:
This was a large-scale, population-based, case-control study. The population was derived from the REACTION study conducted across China. A total of 17,046 individuals (8827 cases and 8219 controls) aged 40 years or older were enrolled in the final analyses. The relationships between SCH and serum lipid parameters in each age group were evaluated after adjustment for thyroid hormones and common confounding factors.
Results:
In the entire population, thyrotropin (TSH), the key indicator of SCH, was positively associated with cholesterol parameters (total cholesterol [TC] and low-density lipoprotein cholesterol [LDL-C]) through the sixth decade of life. After adjusting for common confounding factors and thyroid hormones, each 1 mIU/L increase in TSH was estimated to elevate the TC level by 0.0147 mmol/L and 0.0551 mmol/L, respectively, in individuals aged 40–49 years and 60–69 years. Similarly, with each 1 mIU/L increase in TSH, the LDL-C level tended to show gradually greater increases as age increased. In moderately old subjects (60–69 years), mild (TSH≤10 mIU/L) and significant (TSH>10 mIU/L) SCH increased the concentration of TC approximately 1.03- and 1.36-fold, and the concentration of LDL-C approximately 1.19- and 1.65-fold, respectively, when compared with younger subjects.
Conclusions:
TSH exhibited a stronger effect on the TC and LDL-C level in moderately old subjects than in younger subjects. SCH might augment and worsen the effects of aging on serum lipid profiles.
Introduction
D
Subclinical hypothyroidism (SCH), which is defined by elevated serum thyrotropin (TSH) and normal serum free thyroxine (fT4) (5), is one of the most important modifiable risk factors for dyslipidemia (6,7). Most population-based studies have demonstrated that serum lipids are elevated in patients with SCH (8). Among 25,862 participants in a statewide health fair in Colorado, fasting total cholesterol (TC), triglycerides (TGs), and low-density lipoprotein cholesterol (LDL-C) were significantly higher in SCH subjects than in euthyroid subjects (9). Among a population-based sample of 2799 subjects, a serum TSH>5.5 mIU/L was associated with an average 9 mg/dL elevation in TC (10). Even within the range of TSH that is considered clinically normal, there was a linear and significant increase in TC, LDL-C, and TGs following an increase in serum TSH levels (11). More remarkably, age is also one of the most critical influence factors on SCH. The prevalence of SCH increases with age, reaching up to 20% in people older than 65 years, which is approximately four times the prevalence in 18–24 year olds (9). Epidemiological studies in the United Kingdom have also determined that 10% of women older than 55 years of age have SCH (12,13). Previous studies have only presented the effect of SCH on lipid profiles after adjusting for age. However, few studies have explored the interaction of SCH and age on lipid profiles. It should be investigated whether the impact of SCH on lipid profiles is the same in elderly subjects and in younger subjects. Meanwhile, there is still a lack of large population-based studies that have evaluated the role of SCH in age-related dyslipidemia.
As SCH and dyslipidemia both increase progressively with age, it was hypothesized that the presence of SCH would worsen the effects of aging on serum lipid profiles. Consequently, a large-scale, population-based case-control study was conducted to explore the effect of SCH on lipid profiles across age groups. The results may have important implications for guidelines and public health discussions aimed at preventing atherosclerotic diseases.
Materials and Methods
The institutional review board or ethics committee at each participating institution approved the study protocol. Written informed consent was obtained from each participant before data collection.
Study design and participants
This study was a large-scale, population-based, case-control study. The study population was derived from the REACTION study (14), which aimed to investigate the epidemiology of metabolic diseases and was conducted across China from 2011 to 2012. Study participants were enrolled from Jiangsu Province and Shandong Province of China based on geographic region, population size, and economic status. Urban and rural locations were involved in this survey, and the iodine nutrition status of the areas was stable. The median urinary iodine levels in school-age children were optimal and stable (100–200 μg/L). The two provinces were randomly selected. After identifying the cases, a frequency-matched sample of the controls was then collected using strata according to residence, age, and sex. Because the major focus was on the relationships between SCH, age, and lipid profiles, the investigation was conducted in middle-aged and elderly populations. Individuals older than 40 years of age who had lived in their current residence for five years or longer were included.
In the present study, the following exclusion criteria were used to ensure the strength of the study: (a) missing vital data, such as age, sex, body mass index, or thyroid function analysis; (b) thyroid tumor, history of thyroidectomy, or radioiodine therapy; (c) hypothalamus or pituitary diseases; (d) intake of medications that influence serum lipids or thyroid function (including thyroid hormone, antithyroid drugs, statins, fibrates, amiodarone, estrogens, androgens, steroid hormones, and β-adrenergic blockers) within the past three months; and (e) hereditary hyperlipidemia, serious liver (either alanine aminotransferase or aspartate aminotransferase >100 IU/L) or renal dysfunction (creatinine >105 μmol/L and a glomerular filtration rate <60 mL/min), or malignant tumors. Ultimately, 8827 cases of dyslipidemia were first identified, and a frequency-matched sample of 8219 controls was then collected using strata according to residence, age, and sex (Fig. 1).
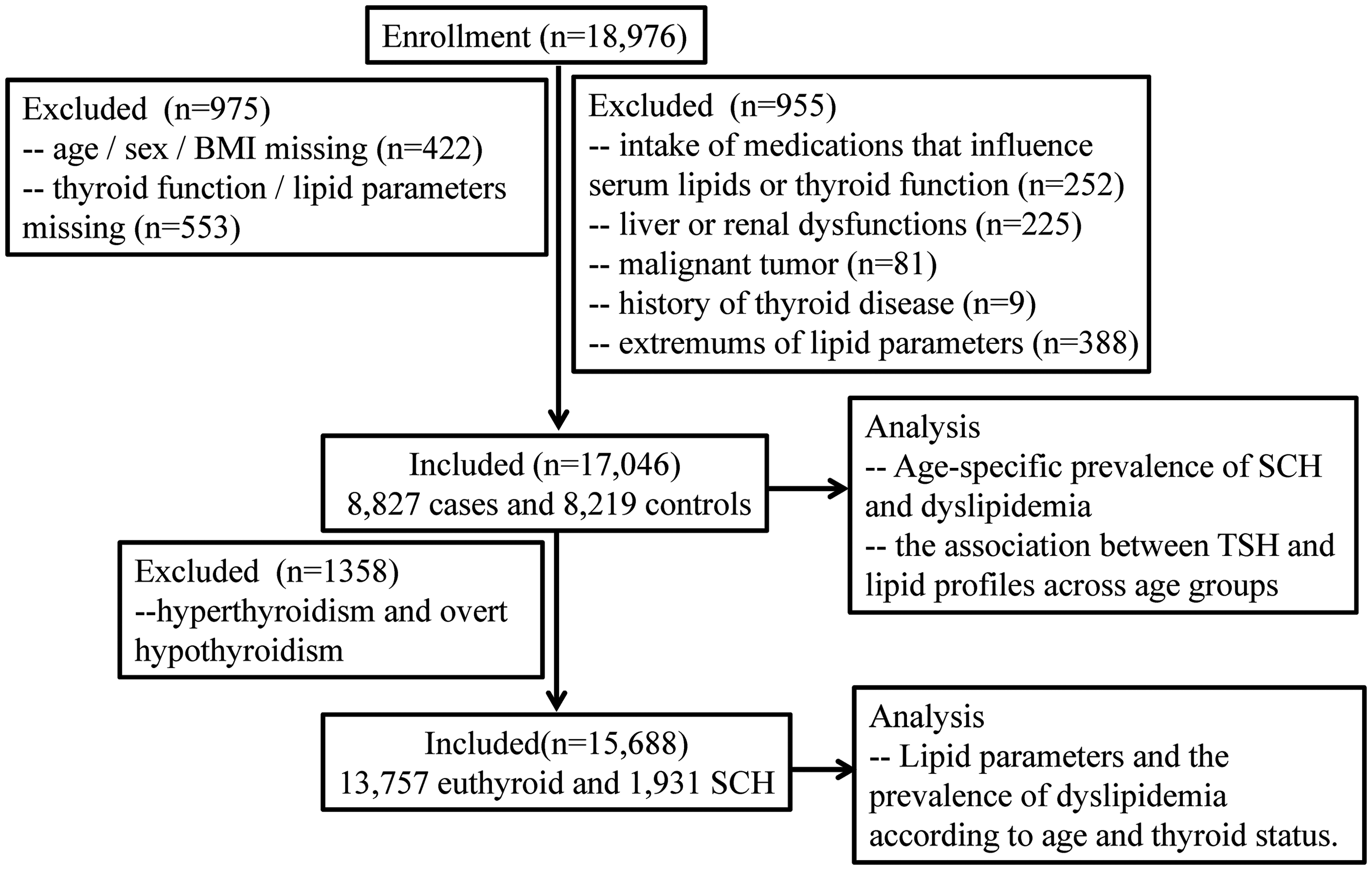
Study design and flow chart.
Data collection
All study investigators and staff members successfully completed a training program that familiarized them with both the aims of the study and the specific tools and methods used. Trained staff administered a standard questionnaire to obtain information on any medication or history of previous medical or surgical diseases. The interview included questions related to the diagnosis and treatment of thyroid dysfunction, dyslipidemia, and cardiovascular events. The smoking and drinking histories of the participants were also recorded. Current smokers were defined as those who had smoked ≥100 cigarettes in their lifetime and smoked tobacco products at the time of the survey. Current drinkers were defined as those who consumed ≥30 g of alcohol per week for at least one year (4). Clinical staff members were trained to measure blood pressure and to obtain anthropometric measurements and blood specimens according to a standard protocol. The blood pressure values are presented as the means of two measurements taken in the sitting position according to a standardized protocol.
Laboratory analyses
Blood samples were collected from all the participants between 8:00 a.m. and 10:00 a.m. after a minimum 10 h fast. Chemiluminescence procedures (Cobas E610; Roche, Basel, Switzerland) were employed to determine the thyroid function, TSH, free triiodothyronine (fT3), and fT4 of each patient. The measurements were performed in the clinical laboratory affiliated with Shandong University. The laboratory reference ranges were 0.27–4.2 mIU/L for TSH, 3.1–6.8 pmol/L for fT3, and 12–22 pmol/L for fT4. Euthyroidism was defined as circulating levels of fT3, fT4, and TSH that were within the reference ranges. SCH was defined as TSH≥4.2 mIU/L with fT4 levels within the reference ranges. Based on the serum TSH level, SCH was further divided into mild (TSH≤10 mIU/L) and significant SCH (TSH>10 mIU/L) (5).
Blood specimens were processed at each regional location and then shipped by air to Shanghai. The lipid profile measurements (TC, TG, LDL-C, and high-density lipoprotein cholesterol [HDL-C]) were performed using an autoanalyzer (ADVIA-1650 Chemistry System; Bayer, Leverkusen, Germany) in the Clinical Laboratory for Endocrinology, Shanghai Institute of Endocrine and Metabolic Diseases. Dyslipidemia was classified and defined in accordance with the National Cholesterol Education Program Adult Treatment Panel III criteria (NCEP/ATPIII) (15). Any of the following criteria was defined as dyslipidemia: (a) high TC: TC≥6.22 mmol/L (≥240 mg/dL); (b) high TGs: TGs≥1.70 mmol/L (≥150 mg/dL); (c) high LDL-C: LDL-C≥4.14 mmol/L (≥160 mg/dL); and (d) low HDL-C: HDL-C<1.04 mmol/L (<40 mg/dL) for men and <1.30 mmol/L (<50 mg/dL) for women.
Statistical analyses
Statistical tests were performed using SPSS Statistics for Windows v17.0 (SPSS, Inc., Chicago, IL). Sample sizes were estimated to meet the recommended requirements for precision in a complex survey design based on the 2010 Chinese census data. Parametric and nonparametric data are presented as the mean (M)±standard deviation (SD) and as the number and percentage. Differences between mean values were tested using Student's t-test, and differences between proportions were tested using the chi-square test. Linear trends for age-specific prevalence were tested using the linear-by-linear association chi-square test. The relationships between TSH and serum lipid parameters were evaluated using partial correlation analysis after adjustment for thyroid hormones (both fT3 and fT4) and several common confounding factors. The response association between TSH and each lipid parameter was analyzed in different age groups using the partial least squares method. The effects of SCH on lipid parameters were investigated using a general linear model among different age groups. All the calculated p-values are two-sided, and p<0.05 was considered statistically significant.
Results
Demographic characteristics of the study population
The basic characteristics of the total subject population (N=17,046; M
age 56.09±8.86 years) are presented in Supplementary Table S1 (Supplementary Data are available online at
Among the entire study population, 19.29% of the population had thyroid dysfunction. The prevalence of SCH, which is the most common type of thyroid dysfunction, was 11.33%. The rate of SCH in the dyslipidemia group was higher than that in the control group (12.34% vs. 10.24%; p<0.001).
Age-specific prevalence of SCH and dyslipidemia in the entire study population
Among all subjects (N=17,046), the prevalence of SCH demonstrated a linear and significant increase with age (linear trend 0.030, p<0.001; Table 1). The prevalence rates of dyslipidemia, high TC, high TGs, and high LDL-C demonstrated linear and significant increases with age (Table 1). Notably, the prevalence rates of high TC and high LDL-C increased 1.61- and 1.69-fold, respectively, from 40 years to 70 years, with a slight decrease in the group aged 70 years and older. However, the prevalence of low HDL-C was reduced with aging.
Linear trends were tested using linear-by-linear association chi-square test.
p-Values<0.05 were considered statistically significant.
SCH, subclinical hypothyroidism; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TGs, triglycerides.
Age-specific association between TSH and lipid profiles after adjustment for thyroid hormones and common confounders
Subsequently, the relationships between TSH and lipid parameters were evaluated across age groups in the entire study population (N=17,046). Importantly, in this section, age, sex, BMI, diastolic blood pressure (DBP), hemoglobin A1c (HbA1c), regional differences, smoking status, and drinking status were adjusted for, which are confounding factors for the association between TSH levels and lipid profiles (8). Furthermore, thyroid hormone (both fT3 and fT4) levels were adjusted for, which affect lipid profiles and thus need to be controlled for to reveal the independent effect of TSH (6,16,17).
As presented in Table 2, TSH had a significant positive association with serum TC in those aged 40–70 years. TSH showed a significant positive correlation with the serum TG level only in those aged 50–59 years. Regarding the relationship between TSH and serum LDL-C, significant positive correlations were observed in both those aged 40–49 years and those aged 50–59 years. There was no relationship between TSH and HDL-C. The relationships between TSH and lipid parameters across age groups were also evaluated in the case and control groups, respectively (Supplementary Tables S2 and S3).
A partial correlation analysis was performed after adjustment for age, sex, body mass index (BMI), diastolic blood pressure (DBP), hemoglobin A1c (HbA1c), smoking status, drinking status, and thyroid hormones.
p-Values<0.05 were considered statistically significant.
A stronger effect of TSH on the TC and LDL-C levels in moderately old subjects
Furthermore, in the entire study population (N=17,046), the study examined whether the extent of the TSH effect on serum lipid parameters was equal among age groups using the partial least squares method (Fig. 2). After adjustment for age, sex, BMI, DBP, HbA1c, smoking status, drinking status, and thyroid hormone (both fT3 and fT4), each 1 mIU/L increase in TSH was estimated to elevate the TC level by 0.0147 mmol/L, 0.0395 mmol/L, and 0.0551 mmol/L, respectively, in individuals aged 40–49 years, 50–59 years, and 60–69 years. Similarly, with each 1 mIU/L increase in TSH level, the LDL-C level tended to show gradually greater increases as age increased. Thus, TSH presented a stronger effect on the TC and LDL-C levels in moderately old subjects (60–69 years) than in younger subjects (aged 40–49 years).
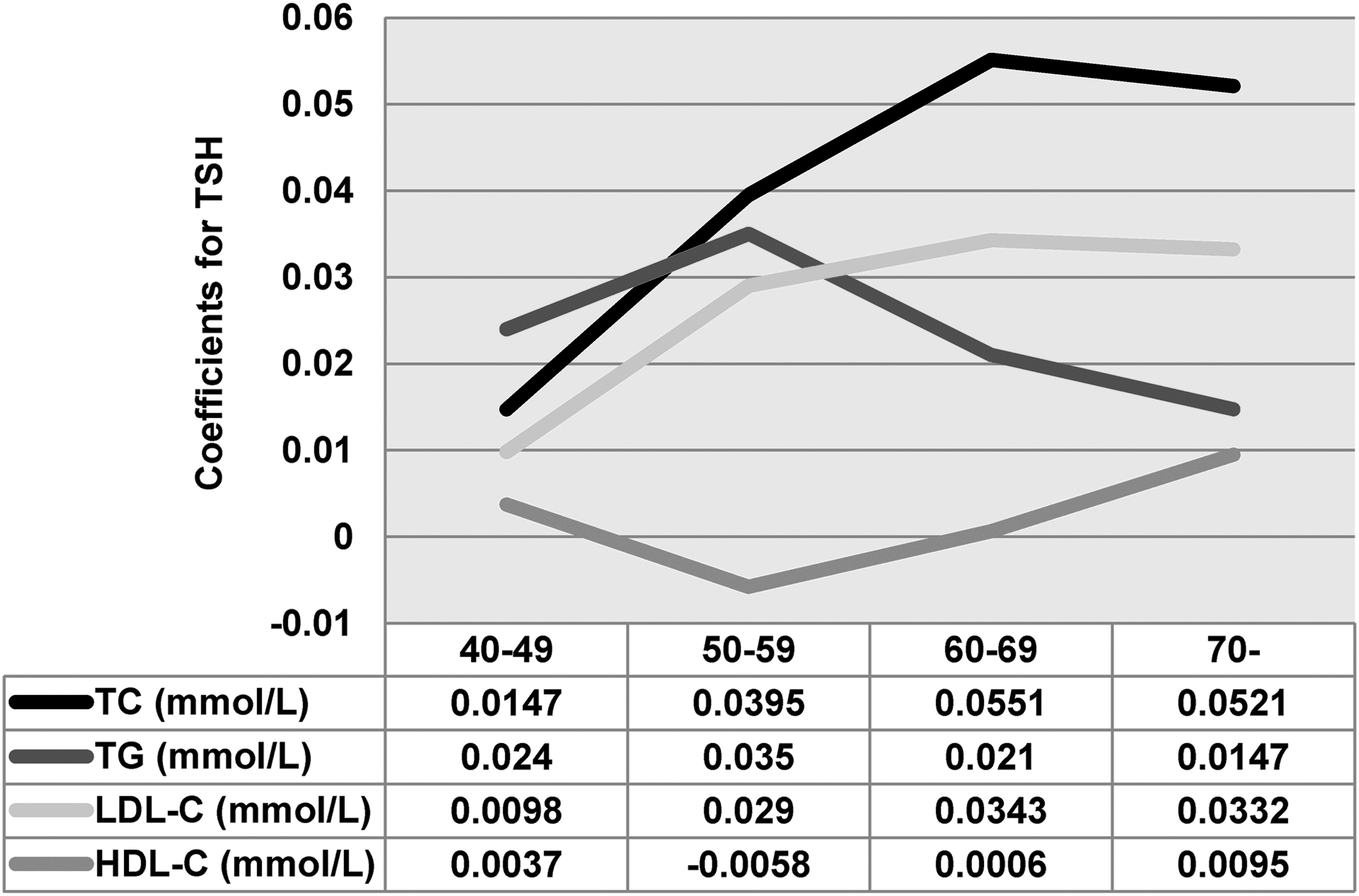
The response association between thyrotropin (TSH) and each lipid parameter in different age groups in the entire study population (N=17,046). The data were analyzed in each age-decade group using the partial least squares method after adjustment for age, sex, body mass index (BMI), diastolic blood pressure (DBP), hemoglobin A1c (HbA1c), smoking status, drinking status, and thyroid hormones. The coefficients indicate the extent to which each 1 mIU/L increase in TSH can affect serum lipid parameters.
SCH worsens lipid profiles, particularly in moderately old subjects
Subsequently, the differences in the prevalence of dyslipidemia and in lipid concentrations between the euthyroid and SCH groups with aging were analyzed. As presented in Figure 3 and Table 3, the analysis of the lipid profiles according to age and thyroid status showed that lipid profiles increased progressively with age and the degree of SCH. Notably, compared with subjects aged 40–49 years, the prevalence of high TC in euthyroid subjects (0.27 mIU/L≤TSH<4.2 mIU/L) aged 60–69 years was increased by 6.76%. By contrast, in patients with mild (4.2 mIU/L≤TSH≤10 mIU/L) and significant (TSH>10 mIU/L) SCH, the prevalence of high TC in individuals aged 60–69 years was increased by 10.11% and 15.33%, respectively, compared with subjects aged 40–49 years. Therefore, in moderately old (60–69 years) subjects, mild and significant SCH increased the prevalence of high TC approximately 1.50- and 2.27-fold, respectively, when compared with younger (aged 40–49 years) subjects. Similarly, in moderately old subjects, mild and significant SCH increased the prevalence of high LDL-C approximately 1.26- and 1.88-fold, respectively, when compared with younger subjects.
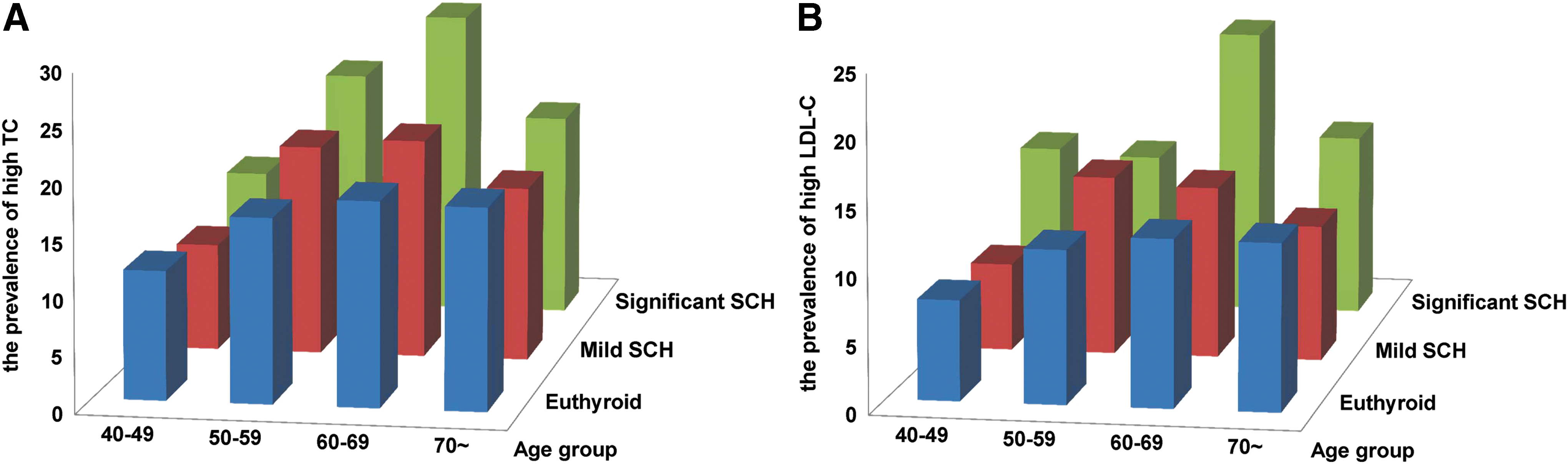
The prevalence of high total cholesterol (TC) and high low-density lipoprotein cholesterol (LDL-C) according to age and thyroid status. Analysis of the lipid profile according to age and thyroid status revealed that the prevalence of high TC
The data are presented as the percentage of individuals in each category.
Euthyroid: 0.27 mIU/L≤TSH<4.2 mIU/L; mild SCH: 4.2 mIU/L≤TSH<10 mIU/L; significant SCH: TSH≥10 mIU/L.
Simultaneously, SCH also increased serum lipid concentrations with age (Table 4). In moderately old subjects, mild and significant SCH increased the concentration of TC approximately 1.03- and 1.36-fold and the concentration of LDL-C approximately 1.19- and 1.65-fold, respectively, when compared with younger subjects.
Lipid concentrations were estimated using General Linear Modeling after adjustment for sex, age, BMI, DBP, HbA1c, smoking status, and drinking status.
The data are presented as estimated marginal means (standard errors).
Euthyroid: 0.27 mIU/L≤TSH<4.2 mIU/L; mild SCH: 4.2 mIU/L≤TSH<10 mIU/L; significant SCH: TSH≥10 mIU/L.
The prevalence of high TGs and low HDL-C changed irregularly with age in subjects with different thyroid statuses (Supplementary Fig. S1).
Discussion
In this large, population-based, case-control study, it was demonstrated that TSH exhibited a stronger effect on the TC and LDL-C level in moderately old subjects than in younger subjects. SCH might augment and worsen the effects of aging on serum lipid profiles. Traditionally, it has been taken for granted that the high prevalence of dyslipidemia in elderly people is a “natural condition.” The results of this study improve upon the traditional concept and suggest that SCH might play a role in age-related dyslipidemia. As aging is a non-modifiable factor for dyslipidemia, these findings have important clinical implications. Based on the results, thyroid screening and modification should be strongly considered in elderly and dyslipidemic patients. Maintaining TSH in an appropriate range might be beneficial for the primary prevention of atherosclerotic diseases.
In agreement with our results, Tognini et al. have reported that age substantially influences the impact of increased TSH on lipid profiles in both males and females (18). However, Tognini et al. investigated a population with a high frequency of endocrine diseases, which may have influenced the serum lipid levels, and they did not exclude patients who had received levothyroxine (L-T4) therapy. These factors may have confounded the interrelationship among age, lipids, and serum TSH. In the present study, a larger natural population was assessed. Importantly, when evaluating the relationship among TSH, lipid profiles, and age, further exclusion criteria were applied and sex, BMI, DBP, HbA1c, smoking status, drinking status, regional differences, and thyroid hormones were adjusted for. Therefore, more subjects, stricter exclusion criteria, and careful study design may improve the power of this study and provide the most reliable and up-to-date information on the relationships among TSH, aging, and lipid profiles in the adult Chinese population.
The main finding of this study is that SCH might play a role in age-related dyslipidemia, which could have important clinical implications. The treatment of SCH by L-T4 replacement is effective and economical (19). The AACE guidelines for SCH recommend that most patients with serum TSH levels of 4.5–10 mIU/L should be considered for treatment (20). However, the treatment of SCH in the elderly population is controversial. Some researchers have raised the interesting point that in many older subjects, the increase in TSH is most likely physiological, and that older people with higher serum TSH should not be labeled as having SCH (21,22). Therefore, they recommend maintaining relatively high TSH levels in elderly people (23). The oldest subjects (>80–85 years) with elevated serum TSH≤10 mU/L should be carefully followed, avoiding hormonal treatment (24,25). The present findings show that TSH exhibited a stronger effect on the TC and LDL-C level in moderately old (60–69 years) subjects than in younger subjects. These results are supported by the majority of previous studies, which demonstrate that TC and LDL-C are elevated in patients with SCH (8,9,26). The laboratory findings also demonstrate that TSH is associated with cholesterol synthesis in the liver and elevated serum cholesterol levels (27). Prospective epidemiological studies have shown that the elevation of serum cholesterol constitutes a major cardiovascular risk factor, and cholesterol-lowering therapy reduces cardiovascular disease risk in many populations (15,28). Therefore, the deteriorating effect of SCH on age-related dyslipidemia may potentially augment the prevalence of cardiovascular disease in elderly people. Nevertheless, the crucial evidence that the treatment of SCH with L-T4 results in a reduction of clinically significant endpoints, including cardiovascular morbidity and mortality, is lacking (29,30). The authors are currently conducting a large randomized controlled trial of L-T4 replacement in elderly populations, and the findings will be helpful to elucidate these issues.
However, in this study, no significant relationship between TSH and the serum lipid parameters was identified in people aged 70 years and older. This finding is in accordance with previous reports demonstrating that the relationship between TSH and serum lipids tends to plateau in the last decades of life (2,4). The following may at least partially explain this result. First, enrollees older than 70 years were relatively healthy, suggesting that individuals who suffered from cardiovascular or other diseases may have died before the age of 70. Second, sick people with mobility difficulties did not enroll in the study. This group undoubtedly included older individuals. Thus, overall, sick people who were older than 70 years tended not to enroll in the study. In addition, the possibility cannot be excluded that the relationships between TSH and serum lipid parameters were not significant in people aged 70 years and older. Similar results have been reported previously. For example, in the Leiden study of subjects aged older than 85 years, increased TSH was associated with increased longevity and decreased risk of death from cardiovascular disease (31). These results and the present findings coincide with the arguments that in the oldest older subjects, the increase in TSH is most likely less harmful and that hormonal treatment should be carefully undertaken (21 –24). The interpretation of these results is unclear. Is TSH less bioavailable in the old? Or are the target organs of TSH impaired due to organ aging? In addition, one must note that using a fixed TSH upper limit might lead to the possibility that too many euthyroid 70 year olds were classified as SCH and the control group might have been more euthyroid (healthy) than most 70 year olds. This may be a limitation of the present study. It is recommended to utilize age-adjusted TSH values. Unfortunately, there are still no reference ranges for TSH in different age group, especially for the Chinese population. Further studies are urgently needed to address these issues.
The strengths of the present study include its population-based, case-control design and its large sample size. The study also has several limitations. First, no conclusions can be drawn about direct causes and effects. Although a variety of confounders were considered, unknown residual confounding factors cannot be excluded. A series of well-designed, prospective clinical and experimental studies are presently underway. Second, the lack of subjects younger than 40 years and the small number of those older than 70 years are also limitations. Therefore, the actual association between serum TSH levels and lipid profiles among subjects older than 70 years may not have been fully reflected here. For further investigation, the authors are planning to recruit additional elderly subjects to account for this shortage. Third, the measurement of serum thyroid peroxidase and thyroid globulin antibodies might be of great interest. Meanwhile, the results were based on a single test of thyroid function, and tests with extremely abnormal results were repeated for confirmation. Although the majority of published studies on thyroid function have adopted a single TSH measurement (32,33), given that a single test may introduce a test bias, this may be a limitation of the present study.
In summary, the findings of this large-scale, population-based, case-control study indicate that SCH and dyslipidemia increase progressively with age in middle-aged and elderly Chinese subjects. Indeed, TSH exhibited a stronger effect on the TC and LDL-C level in moderately old subjects than in younger subjects. Additionally, SCH increased the prevalence of high TC and high LDL-C and augmented the concentrations of TC and LDL-C with age. Thus, SCH might worsen the age-related increase in the prevalence of dyslipidemia. Overall, SCH has generated interest because of its increasing prevalence, its detrimental effects (34,35), and the challenging issues it raises, which must be urgently addressed.
Footnotes
Acknowledgments
This work was supported in part by grants from the National Basic Research Program (2012CB524900), the National Natural Science Foundation (81230018, 81471006, 81430020, 81270869, and 81370891), the Natural Science Foundation (ZR2009CZ009), the Chinese Society of Endocrinology, an international cooperation grant (2011) of Shandong Province and the Jinan self-renovation plan for colleges, universities, and scientific research institutes (2012) of China.
Author Disclosure Statement
No competing financial interests exist.