
Abstract
Background:
Patients with a thyrotropin-secreting pituitary adenoma (TSHoma) are exposed to unregulated and inappropriately high levels of thyrotropin (TSH). Given the rarity of this condition, it is not known whether this chronic TSH stimulation of the thyroid gland might represent a risk factor for the development of differentiated thyroid cancer (DTC). We analyzed the incidence of DTC in a large cohort of patients with TSHomas.
Methods:
The study population consisted of all consecutive patients who underwent neurosurgery for a TSHoma between 1990 and 2013. Criteria for the diagnosis of TSHoma in patients without previous thyroid ablative procedures included elevated free thyroid hormones and normal/high serum TSH concentrations, presence of a lesion at magnetic resonance imaging (MRI), and abnormal response of TSH to at least one dynamic test. Patients who had received thyroid ablative procedures were required to have a pituitary lesion on MRI and TSH levels not suppressed while on levothyroxine therapy at doses causing elevation of free thyroid hormone levels.
Results:
Sixty-two patients (32 females, 30 males) underwent surgery for a TSHoma at our center. Among them, 3 patients had a coexistent diagnosis of DTC with an estimated incidence of 4.8%. In 2 patients, DTC was diagnosed during the evaluation for suspected TSH-dependent hyperthyroidism, whereas in the third patient, diagnosis of DTC preceded the detection of the pituitary tumor.
Conclusions:
The elevated incidence of DTC in patients with TSHoma suggests a possible role of TSH hypersecretion in the development of thyroid tumors. A formal high-resolution ultrasound of the thyroid is recommended in patients diagnosed with a TSHoma, especially if a long history of the pituitary tumor is suspected. Moreover, suspicion about the presence of TSHoma should be raised by the lack of suppression of TSH levels despite adequate doses of levothyroxine after thyroidectomy for DTC.
Introduction
T
Our department is a tertiary referral center for pituitary surgery in Italy. Taking advantage of the possibility to accrue a relatively large number of patients with TSHomas, our study aimed at investigating the frequency of DTC in such a cohort. Moreover, we report in detail the diagnostic and therapeutic challenges that may arise in such an uncommon situation.
Materials and Methods
Patients
The study population consisted of all consecutive patients who underwent neurosurgery for a TSHoma at the Neurosurgical Department of the Istituto Scientifico San Raffaele in Milan, a tertiary referral center for pituitary surgery in Italy. Surgical results in the cohort from 1990 to 1995 have been published previously (19). In patients who had not undergone thyroid ablative procedures in the past, a TSHoma was diagnosed in the presence of elevated free thyroid hormones and normal/high serum TSH concentrations, the presence of a lesion at magnetic resonance imaging (MRI), and an abnormal response of TSH to at least one dynamic test. Lack of inhibition of TSH secretion after triiodothyronine (T3) suppression test (80–100 μg TID orally for 8–10 days) and a TSH peak less than 50% of basal value after thyrotropin-releasing hormone (TRH) stimulation test (200 μg IV) were considered suggestive for a TSHoma. Patients who had received thyroid ablative procedures were required to have a pituitary lesion on MRI and TSH levels not suppressed while on levothyroxine therapy at doses high enough to cause a rise of free thyroid hormone levels.
Laboratory measurements
Venous blood samples were drawn in the morning, after fasting overnight. If the patient was on levothyroxine substitution, the morning dose of the drug was withheld beforehand. In Milan, serum FT4 and FT3 concentrations were measured by immunofluorometric assays (AIA-PACK FT4 and AIA-PACK FT3, Tosoh Corp, Tokyo, Japan). Normal reference ranges are as follows: FT4 0.7–1.7 ng/dL; FT3 2.0–3.6 pg/mL; TSH 0.2–5.0 mU/L. In Cagliari, serum FT4, FT3, and TSH concentrations were assayed by automatic ultrasensitive chemiluminiscent assays (Ortho Clinical Diagnostic SpA, Milan, Italy). Normal reference ranges are as follows: FT4 0.8–2.2 ng/dL; FT3 2.8–5.3 pg/L; TSH 0.2–3.0 mU/L.
The serum alpha subunit was measured by an immunoradiometric assay (Immunotec, Vandreuil, Canada). Normal reference range in normogonadotropic men is 0–0.8 IU/L.
Results
From January 1990 to June 2013, 62 consecutive patients (32 females, 30 males) underwent surgery for a TSH-secreting pituitary adenoma at our center. Mean age at surgery was 43.3±1.7 years (range, 14 to 76 years). Based on MRI findings, 17 patients (27.4%) had a microadenoma and the remaining 45 (72.6%) had a macroadenoma. Invasion of the cavernous sinus was observed in 18 patients (29%). At the time of diagnosis, the mean TSH level was 3.9±0.4 mU/L and it was above 5 mU/L in 15 patients (24.2%). As summarized in Table 1, 3 patients, whose clinical histories are detailed below, had a concomitant diagnosis of DTC. Therefore, the incidence of DTC in our cohort of 62 consecutive patients with TSHomas was 4.8%.
Normal ranges: aTSH, 0.2–3.0 mU/L; FT3, 2.8–5.3 pg/mL; FT4, 0.8–2.2 ng/dL.
TSH, 0.3–4.2 mU/L; FT3, 2.3–4.5 pg/mL; FT4, 0.9–1.7 ng/dL; alpha subunit, 0–0.8 IU/L; alpha subunit/TSH calculated according to Beck-Peccoz et al. (1), reference value for normogonadotropic controls with normal TSH <5.7.
Before starting therapy with somatostatin analogues.
While on therapy with suppressive doses of levothyroxine after thyroidectomy.
TSHoma, thyrotropin-secreting pituitary adenoma; DTC, differentiated thyroid cancer; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyrotropin; ND, not done.
Patient 1
A 47-year-old male came to our attention because of hyperthyroidism with inappropriately normal levels of TSH. His medical history began at the age of 37 years, when he underwent thyroid function tests because of palpitations, weakness, and an anxiety disorder. Laboratory data performed elsewhere showed a high FT3 (9.0 pg/mL; reference range, 2.8–5.3 pg/mL) and FT4 levels (2.2 ng/dL; reference range, 0.7–1.6 ng/dL) with high normal levels of TSH (4.4 mU/L; reference range, 0.25–5.0 mU/L). Ultrasonography of the neck showed a solid hypoechoic thyroid nodule in the left lobe. Apparently, the attending physician of the patient at that time diagnosed RTH and no further diagnostic evaluation or treatment was suggested. At the age of 47 years, palpitations and anxiety symptoms persisted and he sought a second opinion. Repeated thyroid function tests confirmed high levels of thyroid hormones (FT3 7.3 pg/mL; reference range, 2.8–5.3 pg/mL; FT4 3.1 ng/dL; reference range, 0.8–2.2 ng/dL), with inappropriately normal values of TSH (2.9 mU/L; reference range, 0.2–3.0 mU/L), and slightly increased alpha subunit concentrations (0.89 IU/L, reference range 0.0–0.8 IU/L). Other pituitary hormones were within the reference range. A TRH stimulation test elicited no response of TSH, FT3, FT4, and alpha subunit. An MRI revealed a 10 mm×19 mm pituitary mass occupying the anterior and left side of the pituitary gland. A diagnosis of TSHoma was confirmed. A repeated neck ultrasonography confirmed the presence of a 20 mm×13 mm solid hypoechoic thyroid nodule in the left lobe with enhanced intranodular vascularization during color Doppler evaluation. A thyroid scan showed a reduced 131I uptake. A fine-needle aspiration biopsy (FNAB) of the nodule was diagnostic for follicular neoplasm (class IV, according to the Bethesda classification). We decided to schedule a total thyroidectomy first and to start therapy with lanreotide 120 mg subcutaneously monthly. One month after the beginning of lanreotide, normalization of FT3 and FT4 values was obtained and the TSH level decreased to 0.68 mU/L. The patient then underwent total thyroidectomy with central neck lymph node resection. Postoperative histologic examination confirmed the diagnosis of a 15 mm follicular carcinoma, Hürthle cell variant, with no invasion of the thyroid capsule, blood vessels, and neck lymph nodes. The 131I total body scan performed after surgery revealed a small bilateral residual uptake at the level of the thyroid gland. The patient was treated with 106 mCi of 131I after stimulation with recombinant TSH. The final TNM evaluation was pT1bN0M0. Therapy with 1.7 μg/kg per day of levothyroxine was started immediately after surgery, in association with lanreotide subcutaneously, but TSH values remained between 1.56 and 2.27 mU/L, even when free thyroid hormone concentrations were at the upper limit of the reference range. Approximately 10 months after total thyroidectomy, the patient underwent trans-sphenoidal resection of the pituitary adenoma. Intraoperatively, a fibrous pathologic nodule located in the superior and left portion of the gland was identified and completely removed. Postsurgical histologic examination showed fibrous tissue that did not stain positive for TSH or the other pituitary hormones. The postoperative course was uneventful. On the fifth postoperative day and while on the same dose of levothyroxine therapy, the TSH level decrease to 0.2 mU/L, while FT3 and FT4 levels were 1.3 pg/mL and 1.3 ng/dL, respectively. One month after surgery, the TSH level was suppressed (0.1 mU/L) with borderline elevated FT3 and FT4 levels (3.5 pg/mL and 1.7 ng/dL, respectively). A postoperative MRI, performed 6 months after pituitary surgery, showed no residual pituitary adenoma.
Patient 2
A 46-year-old male presented with an episode of atrial fibrillation. His previous medical history was unremarkable except for nephrolithiasis. Thyroid function tests revealed high values of FT3 (8.9 pg/mL; reference range, 2.8–5.3 pg/mL) and FT4 (3.1 ng/dL; reference range, 0.8–2.2 ng/dL) with inappropriately normal levels of TSH (2.5 mU/L; reference range, 0.2–3.0 mU/L). Serum anti-TSH receptor antibodies (TRAb), TPOAb, and TgAb were all negative. The alpha subunit value was normal (0.49 IU/L, normal values 0–0.8 IU/L), as well as growth hormone (GH) and insulin-like growth factor (IGF)-1 levels (0.3 ng/mL and 120 ng/mL, respectively). The other anterior pituitary axes were intact. A TRH test elicited no response of TSH and alpha subunit levels. A suppression test with octreotide 0.1 mg subcutaneously showed a 36% reduction of TSH levels 6 hours after drug administration (from 2.4 to 1.5 mU/L). A pituitary MRI demonstrated the presence of a 7 mm lesion in the left side of the pituitary gland. The diagnosis of a TSHoma was made. A neck ultrasonography revealed a 25×17 mm solid hypoechoic thyroid nodule in the right lobe, with prevalent perilesional vascularization during color Doppler examination. A thyroid scan showed a reduced 131I uptake of the thyroid nodule. The patient underwent FNAB and the cytologic evaluation of the nodule suggested a follicular neoplasm (class IV, according to Bethesda classification). Surgical resection of the pituitary lesion was scheduled. In the meantime, therapy with lanreotide 120 mg monthly was initiated, which led to normalization of thyroid hormone levels after 4 months (FT3 2.4 pg/mL, FT4 1.9 ng/dL). Trans-sphenoidal resection of the pituitary tumor was then performed. Histologic evaluation showed a pituitary adenoma with 1% of GH-positive cells on immunohistochemistry and negative staining for all other pituitary hormones. Five days after surgery, the TSH level was undetectable with normalization of FT3 and FT4 values. A pituitary MRI, performed 2 months after surgery, showed no residual disease. Soon thereafter, the patient underwent total thyroidectomy with central neck lymph node resection. Postoperative histologic evaluation revealed a 12 mm papillary carcinoma, follicular variant, with no invasion of thyroid capsule, blood vessels, and neck lymph nodes. The 131I total body scan showed a small bilateral residual uptake at the level of the thyroid bed. Final TNM evaluation was pT1bN0M0. The patient was treated with 100 mCi of 131I after stimulus with recombinant TSH. Immediately after surgery, therapy with levothyroxine 1.6 μg/kg per day was started. At the last follow-up visit, 5 years after thyroidectomy, the TSH level is adequately suppressed (0.2 mU/L) with a normal level of FT3 (3.2 pg/mL) and a minimally elevated FT4 level (1.7 ng/dL). Another pituitary MRI did not show any recurrence of the pituitary tumor.
Patient 3
A 42-year-old male presented to our outpatient clinic with the diagnosis of a nonfunctioning pituitary adenoma. His medical history began at the age of 36 years, when he underwent total thyroidectomy because of a bifocal papillary carcinoma of the thyroid gland with metastatic invasion of three central lymph nodes in the neck. Thyroid function tests, performed before thyroidectomy, were as follows: FT3 1.8 pg/mL (reference range 2.3–4.5 pg/mL), FT4 0.9 ng/dL (reference range 0.9–1.7 ng/dL), and TSH 2.2 mU/L (reference range 0.3–4.2 mU/L). After surgery, he was treated with 100 mCi of 131I. The postsurgical final TNM evaluation was pT3bN1aM0. In the subsequent 6 years, there was no recurrence of disease. As shown in Figure 1, therapy with levothyroxine was started immediately after surgery. Complete TSH suppression (as required by the standard therapeutic protocols at the time when the patient was submitted to total thyroidectomy) was never achieved, despite a dose of levothyroxine as high as 2.8 μg/kg per day, with FT3 and FT4 values at the upper limits of the reference range (1 year after surgery: FT3 3.6 pg/mL, FT4 1.9 ng/dL, TSH 1.3 mU/L). Liothyronine 20 μg/d was also added to therapy, with no effect on TSH, FT3, and FT4 values. Two years after thyroidectomy, a pituitary MRI revealed a 12 mm pituitary mass with no extrasellar invasion. The other pituitary axes were normal. The patient was referred to another tertiary center for pituitary disease where a diagnosis of an incidental nonfunctioning pituitary adenoma was established, and the hormonal data misinterpreted as showing incomplete compliance with substitution therapy. Yearly follow-up with sellar MRI for 4 years did not reveal any apparent change of tumor size. Six years after thyroidectomy, a repeat MRI showed a slight increase of tumor size and for this reason the patient was referred to our clinic. Preoperative results confirmed lack of suppression of TSH levels (1.5 mU/L) with a normal FT3 level (3.0 pg/mL) and an increased FT4 level (2.0 ng/dL). A TSHoma was diagnosed. Radical removal of the tumor was achieved through a trans-sphenoidal approach. Histologic evaluation confirmed the presence of a pituitary adenoma with 40% of TSH-positive cells on immunohistochemistry. Eighteen and 28 months after surgery, pituitary MRIs showed no recurrence of the tumor and laboratory tests revealed an adequate suppression of TSH values (<0.1 and 0.3 mU/L, respectively), with normal values of FT4 (1.2 and 1.2 ng/dL, respectively), while on therapy with levothyroxine 1.84 and 1.53 μg/kg per day, respectively (Fig. 1).
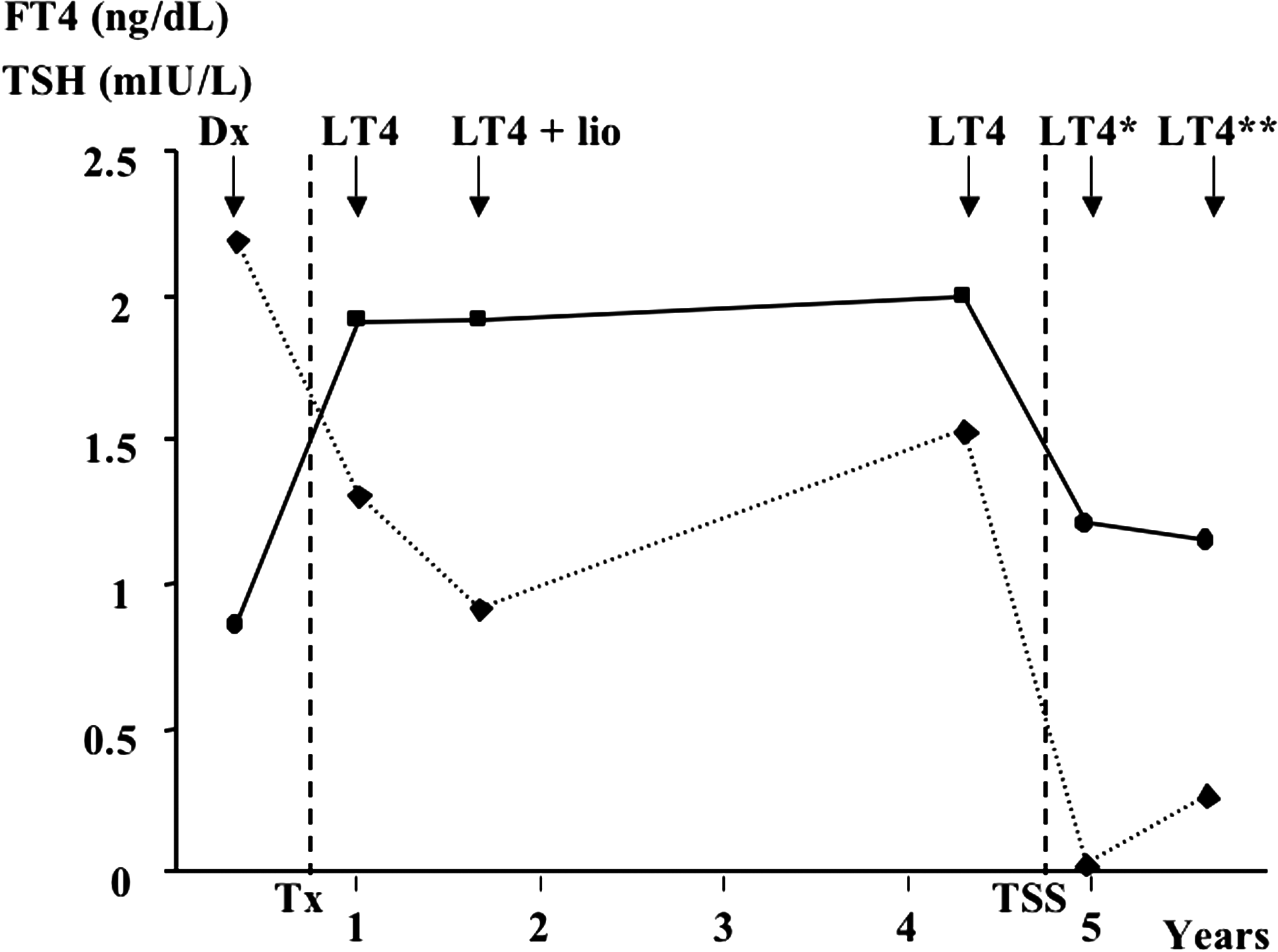
Serum FT4 (continuous line) and TSH levels (dashed line) in a patient with TSHoma and a coexistent DTC. At the top of the figure Dx indicates the time of diagnosis of DTC. Soon thereafter, thyroidectomy (indicated by Tx and a vertical dashed line) was performed. When the diagnosis of TSH-secreting pituitary adenoma was done, removal of the pituitary tumor through trans-sphenoidal surgery was performed (indicated by TSS and a vertical dashed line). Different doses of thyroid replacement therapy were used during follow-up (LT4=levothyroxine 2.8 μg/kg per day; LT4+lio=levothyroxine 2.8 μg/kg per day+liothyronine 20 μg/d; LT4*=levothyroxine 1.84 μg/kg day; LT4**=levothyroxine 1.53 μg/kg per day. FT4, free thyroxine; TSH, thyrotropin; TSHoma, thyrotropin-secreting pituitary adenoma; DTC, differentiated thyroid cancer.
Discussion
TSH is the major growth factor for thyroid cells and many experimental studies suggest that it could have a role in carcinogenesis and development of thyroid tumors (6 –10, 20). A recent dose-response meta-analysis of 22 studies has demonstrated that slight increments of mean serum TSH levels are associated with a higher risk of thyroid cancer, even in the presence of normal or subnormal concentrations of TSH (20). Moreover, maintenance of suppressed TSH levels in the management of patients with thyroid cancer is associated with a lower risk of tumor recurrence and mortality in high-risk patients (21), supporting the relevance of TSH in tumor development and growth.
All these data suggest a possible increased risk of thyroid tumors in patients with TSH-secreting pituitary adenomas, which are characterized by autonomous hypersecretion of TSH (2). Nevertheless, the exact clinical impact of this continuous TSH stimulation on the thyroid gland has not been well established. TSHomas account for about 0.5–3% of all pituitary adenomas (2). The rarity of this tumor makes it very difficult to know the exact prevalence of thyroid tumors in patients with TSHomas. Until now, only a few isolated cases of TSHomas coexisting with DTC have been reported in the literature (11 –18). In Table 2, we summarize some clinical information of the patients reported in the literature together with the present series. To the best of our knowledge, our series of 62 surgically treated patients with TSHomas is one of the largest in the world. Herein, we describe three cases of TSHomas coexisting with a DTC, for an overall incidence of 4.8%. Histologic examination of the pituitary tumor did not reveal a positive staining for TSH in patient 1 and 2. This is not an exceptional finding, however, and has been reported in other cases (1,22). It is likely that some TSHomas have only few cells that are positive for TSH and may, therefore, escape detection on routine histopathologic examination. Nevertheless, the preoperative hormonal picture and the resolution of the endocrine abnormalities after surgery confirm the diagnosis of a TSHoma in both patients.
DTC, differentiated thyroid cancer; TSHoma, thyrotropin-secreting pituitary adenoma; NR, not reported; SSA, somatostatin analogues; TNS, trans-sphenoidal surgery.
Patient 3 had histologic confirmation of TSH immunoreactive cells in the pituitary tumor. However, he had normal FT3 and FT4 levels before thyroidectomy and the diagnosis of a pituitary adenoma was first confirmed 2 years after thyroid surgery. Therefore, from our data we can speculate that this patient was still euthyroid before thyroidectomy probably because the pituitary tumor was not yet secreting sufficient amounts of TSH to cause hyperthyroidism. Alternatively, the development of the TSHoma occurred in the two years between thyroidectomy and its detection. However, the slow rate of tumor growth seems to support the first hypothesis. All three of our patients had normal TSH levels. This is not uncommon in TSHomas (1,19,22), adding to the diagnostic complexity of this rare disease. It has been demonstrated that neoplasm-derived TSH shows a higher bioactivity (23), thus explaining the presence of elevated FT3 and FT4 levels despite normal TSH values.
The incidence of DTC was previously reported to vary worldwide between 1.2–2.6 per 100,000 individuals for males and 2.0–3.8 per 100,000 individuals for females (24), but this incidence is steadily increasing in the last decade. According to WHO's International Agency for Research on Cancer (25), the current estimation for Italy provides an annual incidence of 6.7 per 100,000 in males and 14.7 per 100,000 in females, corresponding to an age-adjusted prevalence of 42.5 per 100,000 for males and 105 per 100,000 for women. Although our study does not allow a precise epidemiological estimation of the risk of thyroid cancer in patients with TSHomas because of the inevitable small sample size, our findings suggest an increased risk of DTC in patients with a TSHoma, possibly through a stimulatory effect of TSH hypersecretion on cancer development. This is in agreement with recent clinical and experimental studies, which have shown a possible direct role of TSH in the carcinogenesis and progression of thyroid tumors (6 –10). On the other hand, the prevalence of DTC in multinodular goiters (a condition more comparable to the thyroid involvement in TSHomas) is reported between 1% and 15% (26), a value not different from our observation. Thus, taking also the small number of cases reported in the present study into account, no firm conclusion can be drawn on the risk for DTC actually associated with TSHomas.
As is common in patients with this rare type of pituitary adenomas, in patients 1 and 3 a long time elapsed (ranging from 6 to 10 years) before the pituitary tumor was diagnosed as a TSHoma. A long history of disease could represent an additional risk factor for the development of DTC in patients with TSHomas. Previous studies have also described an association between DTC and a long-term exposure to high TSH levels in patients with TSHomas (18). Based on this, the presence of a thyroid tumor should be ruled out accurately in patients with a long history of TSH hypersecretion from a pituitary tumor.
In patient 2, it was not possible to achieve an adequate suppression of TSH levels before the resection of the pituitary tumor after thyroidectomy. In patient 3, the TSHoma was diagnosed because of TSH levels that could not be suppressed with thyroid hormone after thyroidectomy for DTC. Thus, the lack of suppression of TSH levels after thyroidectomy for DTC despite apparently adequate replacement therapy with thyroid hormones could be a possible clinical presentation in a patient with a TSHoma, once more common causes, such as lack of compliance and absorption problems, have been excluded. RTHβ coexistent with a pituitary incidentaloma would also resemble the situation of our patient, but this combination is exceedingly rare. Nevertheless, in our patient RTHβ can be excluded by the postoperative changes of thyroid hormones and TSH.
The optimal treatment strategy in patients with TSHoma and coexistent DTC has not been established (11 –18) (Table 2). Some authors prefer to perform pituitary adenomectomy before total thyroidectomy, to avoid a theoretically possible growth of the TSHoma and to normalize TSH levels, thus removing a stimulus for DTC progression (17,18). Another reason given for this strategy is that performing pituitary surgery first could be helpful to control thyrotoxicosis and reduce thyroid vascularization to perform thyroid surgery under optimal conditions (18). On the other hand, according to other authors, thyroid surgery should be performed before pituitary adenomectomy, even if it could lead to a progression of the TSHoma (14). In patient 1, we decided to perform thyroidectomy first and postpone resection of the pituitary tumor. Simultaneously, the patient was treated with somatostatin analogues and we did not observe any significant growth of the pituitary adenoma. In patient 3, pituitary adenomectomy was performed 6 years after total thyroidectomy, because of an initial erroneous diagnosis of a nonfunctioning pituitary adenoma. After thyroidectomy, pituitary MRI follow-up studies did not show any apparent change of tumor size for at least 4 years, despite no concomitant medical therapy for the TSHoma. In our opinion, considering the malignant nature of thyroid cancer versus the benign nature of TSHomas, total thyroidectomy should have priority over pituitary surgery in most cases, especially when the pituitary tumor does not cause mass effect symptoms, because in the short term the risk of TSHoma progression after thyroidectomy is probably less than the risk of delaying thyroid surgery. On the other hand, in patients with a large and/or invasive TSHoma causing neurologic symptoms, the reverse order of treatment might be appropriate. Nevertheless, the therapeutic strategy should be individualized for every single patient, taking into account all the relevant associated comorbidities.
Another treatment option for TSHomas, when it is not possible to perform surgical resection or while awaiting surgery, is medical management with somatostatin analogues (27 –31). Treatment with octreotide has been reported in a patient with TSHoma coexisting with DTC, who declined pituitary surgery, leading to normalization of thyroid function (17). In patients 1 and 2 we decided to start therapy with lanreotide, while waiting for pituitary adenomectomy, to improve the biochemical status of the patients. In patient 1, therapy with lanreotide led to normalization of thyroid function one month after the beginning of medical therapy, but after thyroidectomy, it was unable to produce an adequate suppression of TSH values. In patient 2, we observed a complete normalization of thyroid function soon after starting lanreotide.
To summarize, we describe three patients with TSHomas coexisting with DTC, which, to the best of our knowledge, represents the largest series described in the literature to date. The observed frequency of DTC in our patients with TSHomas is 4.8%, suggesting a possible role of TSH hypersecretion in the development of thyroid tumors. Our findings confirm the importance of considering the presence of a thyroid carcinoma in patients diagnosed with a TSHoma, especially if a long history of the pituitary tumor is suspected. A formal high-resolution ultrasound of the thyroid is recommended in patients with a TSHoma. Lack of suppression of TSH levels after thyroidectomy for DTC may represent a possible clinical presentation of a TSHoma. Thus, it is important to rule out a TSHoma when an adequate suppression of TSH levels cannot be reached after thyroidectomy.
Footnotes
Acknowledgment
We thank Denise O'Toole, Gamma Knife Service of the Neurosurgical Department of San Raffaele Hospital, for her editorial assistance and stylistic revision of the manuscript.
Author Disclosure Statement
No competing financial interests exist.