
Abstract
Background:
Treatment with antithyroid drugs is effective in conditions of increased thyroid hormone production (mostly Graves' Disease; GD), but not in subacute thyroiditis (SAT) or autoimmune thyroiditis (AIT). Positive thyroid stimulating immunoglobulins (TSI) make GD likely. However, not all children with GD have increased TSI. Uptake studies with 123I or 99Tc (99mTc) provide accurate and rapid diagnosis but are expensive and involve radiation exposure. Our objective was to compare TSI with 99mTc uptake for diagnosis of pediatric hyperthyroidism.
Methods:
We performed a retrospective chart review of hyperthyroid children who had both TSI estimation and 99mTc uptake assessment at presentation. Based on subsequent laboratory studies and follow-up, 37 had GD and 10 had non-GD thyroiditis. The TSI index was considered positive (TSI+) when it was above the upper limit of normal. 99mTc uptake was considered positive (Tc+) for any uptake >0.4% and negative (and low) (Tc-) for uptake ≤0.4%.
Results:
Forty-seven youth (83% females), aged 12.3±4.6 years, presented with a suppressed thyrotropin (TSH) and elevated free thyroxine and total triiodothyronine. All 37 patients with GD were Tc+ (100% sensitivity and specificity). The sensitivity of TSI for diagnosing GD was 84%, and the specificity was 100%. Six patients with GD were discordant with Tc+ but TSI–. Elevated TSI correlated with Tc+ (p=0.01) with a degree of agreement (kappa) of 0.69.
Conclusion:
99mTc has excellent specificity and sensitivity in diagnosing GD. Given additional costs of 99mTc (two and a half times as much as TSI), it is reasonable to reserve 99mTc uptake assessment for hyperthyroidism of unclear etiology and negative TSI.
Introduction
A
The American Thyroid Association (ATA) recommends obtaining a thyroid scan for hyperthyroidism of unclear etiology (7), in order to differentiate hyperthyroidism due to increased synthesis of TH from increased release of preformed TH from thyroid follicles. Traditionally, and per ATA recommendation, 123Iodine (123I) is used for this purpose in many centers. Technetium99 (99mTc) is taken up by the thyroid follicular cells but, in contrast to 123I, does not undergo organification. Yet 99mTc scans can provide excellent information regarding morphology and thyroid function. While both 99mTc and 123I can be used for determination of isotope uptake, 99mTc provides more rapid diagnosis (within minutes of the procedure as opposed to hours with 123I) (8). Further, 99mTc involves less radiation to the thyroid and has a lower total effective dose than 123I (99mTc: 0.009 rems; 123I: 0.16 rems, for respective doses administered during uptake studies) (9,10). For these reasons, 99mTc is the preferred isotope uptake at our center for hyperthyroidism evaluation. However, the 99mTc scan is expensive (compared with assessment of TSI) and not available at all centers. Given the cost and radiation exposure with 99mTc scans, we sought to evaluate the efficacy of TSI compared with measured uptake on the 99mTc scan in differentiating GD from SAT and AIT.
Materials and Methods
We performed a retrospective medical record data analysis of patients who presented to our pediatric endocrine unit between January 2002 and January 2014 with symptoms of hyperthyroidism and a suppressed TSH level associated with an elevated total triiodothyronine (T3) and/or elevated free thyroxine (T4). Subjects with diagnoses such as thyroid nodules or thyroid malignancy were excluded. Our initial query retrieved 111 patients. Of these patients, only 47 (42%) had assessment of both TSI levels and a 99mTc scan at the time of diagnosis. These 47 subjects were included in our study to allow us to examine the utility of 99mTc compared with TSI. Details of clinical presentation included signs and symptoms at diagnosis and physical exam findings such as thyroid enlargement or a thyroid bruit. Diagnosis of the cause of hyperthyroidism was established based on subsequent laboratory tests and clinical progress. GD was diagnosed by clinical presentation and successful treatment with antithyroid medication, surgery, or radioactive ablation at follow-up visits. AIT was defined by spontaneous resolution of symptoms with normalization of thyroid function tests at subsequent visits and the presence of thyroid peroxidase or thyroglobulin antibodies. SAT was characterized by the absence of thyroid peroxidase or thyroglobulin antibodies and spontaneous resolution of symptoms at follow-up. No patient had painful thyroiditis, as is often seen in SAT. We recognize that there is overlap between these definitions of AIT and SAT diagnosis and have combined these patients into a single non-GD thyroiditis group for further analyses.
Laboratory tests, including levels of TSH, free T4, total T3, thyroid peroxidase and thyroglobulin antibodies, and TSI, were recorded, in addition to 99mTc uptake. Thyroid function tests were obtained by electrochemiluminescence immunoassays. The normal range for TSH was 0.4–5.0 mIU/L with a lower detection limit of 0.005 mIU/L. For TSH values reported as <0.01 mIU/L, we assumed the value to be 0.009 mIU/L. The detectable range for free T4 and total T3 in the assay was 0.023–7.77 ng/dL (0.300–100.0 pmol/L) and 19.5–651 ng/dL (0.3–10.0 nmol/L) respectively, with normal ranges between 0.9 and 1.8 ng/dL (12–23 pmol/L) for free T4 and 60 and 181 ng/dL (0.92–2.8 nmol/L) for total T3. Five patients had thyroid function tests drawn at other laboratories with slightly variable ranges of normal measurements. In order to account for this variability, we present hormone and antibody levels as multiples of the upper limit of normal (ULN; for thyroid hormones and TSI) or of the lower limit of normal (LLN; for TSH). TSI assessment was performed at the Mayo Medical Laboratories (11) by comparing cyclic AMP activity in TSH responsive cell lines after addition of patient's serum with exposure to normal control serum. The test was performed using Diagnostic Hybrids kits with a coefficient of variation of <15%. The clinical sensitivity and specificity for the test was determined to be 92% and 99.4% respectively (12). In 11 out of 37 patients with GD, the TSI was sent out to other clinical laboratories. Therefore, we performed the analysis with the TSI value represented as multiples of the ULN for the respective labs. The test was considered positive if the TSI index was above the upper limit of normal for the lab.
The 99mTc uptake was performed in the Nuclear Medicine Unit of Massachusetts General Hospital (MGH). 99mTechnetium pertechnetate was given as an intravenous injection, and the dose was calculated based on the patient's weight (0.15 mCi/kg). Standard and pinhole images were obtained 20 minutes after the intravenous injection, and an uptake was calculated. Quantified 99mTc uptake varies geographically. The lower limit of normal was based on the normal reference range described by our nuclear medicine department, which is 0.5–3.75%. Therefore we considered uptake ≤0.4% to be decreased/negative and suggestive of destructive/non-GD thyroiditis. Any uptake, that was either increased or inappropriately normal was considered a positive result and suggestive of GD. In 3 out of 47 patients, the absolute value of uptake was not quantified, but the report indicated symmetrically increased uptake in both lobes and the results were considered positive.
Statistical analysis
Statistical analysis was performed with SAS v9.2 (SAS Institute). Descriptive data are presented as mean±standard deviation or n (%). Analysis of variance and Fisher's exact test were used to compare continuous and categorical variables respectively. Sensitivity, specificity, and positive and negative predictive values of TSI in the diagnosis of hyperthyroidism were calculated. Degree of agreement between TSI and 99mTc uptake was calculated using the McNemar test.
Results
Demographic details
Patient characteristics of the diagnostic groups are presented in Table 1. The majority of patients (79%) had a diagnosis of GD, and 21% had non-GD thyroiditis. Age at presentation did not differ significantly between the two groups. However, subjects who presented with non-GD thyroiditis tended to be older than those with GD (14.8±4.5 years in non-GD thyroiditis vs. 11.7±4.4 years in GD; p=0.05).
The bolded p-values indicate statistical significance with p<0.05.
GD, Graves' disease; TSH, thyrotropin; LLN, lower limit of normal; T4, thyroxine; ULN, upper limit of normal; T3, triiodothyronine.
Clinical features
Thyroid enlargement was noted on physical examination in 32 of 37 subjects with GD, while only 5 of 10 patients in the non-GD thyroiditis group had thyroid enlargement (p=0.02). The presence of a thyroid bruit was assessed in only 24 (51%) subjects. Eight of 24 patients (33%) had a positive bruit on exam, and all subjects with a positive bruit were eventually diagnosed with GD. Eleven of the 16 subjects who were not found to have a bruit on examination had GD, and five had non-GD thyroiditis.
The clinical characteristics of the six GD patients with negative TSI compared with the GD patients with positive TSI are presented in Table 2. Of the 37 patients who were diagnosed with GD, three were in remission at the time of data collection and off antithyroid medication. Two patients were in remission for a few months to a year but subsequently had to be restarted on antithyroid medications due to relapse. Eight of the 37 patients chose to undergo a total thyroidectomy for reasons such as noncompliance, side effects of medication, or lack of response to medication. Three patients underwent radioactive iodine therapy. We are thus not able to comment on the remission status of these 11 individuals. One person was given a trial off medication and remained clinically euthyroid but biochemically continues to have suppressed TSH levels; we do not consider this a remission. The remaining 20 patients continue to take antithyroid medications and have not achieved remission.
TSI, thyroid stimulating immunoglobulins.
Laboratory tests
Both groups had suppressed TSH levels. The GD group had significantly higher levels of free T4 and total T3 compared with the non-GD thyroiditis group (p=0.001 and p=0.0006 respectively). All non-GD thyroiditis patients except one had free T4 and total T3 levels less than twice the ULN. In contrast, 27/36 of the subjects with GD had free T4 levels more than twice the ULN, and 24/31 had total T3 levels elevated more than twice the upper limit of normal.
TSI and 99mTc uptake
TSI
TSI were positive in 31/37 subjects with GD and negative in all patients with non-GD thyroiditis (n=10). TSI had 84% sensitivity and 100% specificity in accurately diagnosing GD. The positive predictive value (PPV) of this test was 100%, while the negative predictive value (NPV) was 63% in differentiating hyperthyroidism from GD compared with non-GD thyroiditis.
99mTc uptake
99mTc uptake was increased in all patients with GD and decreased in all non-GD thyroiditis subjects. The 99mTc uptake had 100% sensitivity, specificity, PPV, and NPV in differentiating hyperthyroidism from GD compared with non-GD thyroiditis. There was a clear distinction in the magnitude of 99mTc uptake between our GD (mean 14.3±8.8%, median 11%, range 1.9–35.4%) and non-GD patients (mean 0.2±0.1%, median 0.15%, range 0.0–0.4%; p<0.0001).
We did not find a significant difference in absolute 99mTc uptake in patients with complete remission (mean uptake 7.9±2.7%, median 6.4%, range 6.3–11%), intermittent remission (mean uptake 13.4±6.0%, median 13.4%, range 9.1–17.6%), or those who continue on medication without remission (mean uptake 13.3±9.0%, median 10.1%, range 1.9–32.3%; p=0.26).
There was significant agreement (p=0.01) between increased 99mTc uptake and positive TSI with a kappa coefficient of 0.69 [confidence interval (CI) 0.47–0.91]. There was a modest correlation (r=0.35, p=0.02) between the magnitude of 99mTc uptake and absolute TSI values (expressed as multiples of ULN; Fig. 1).
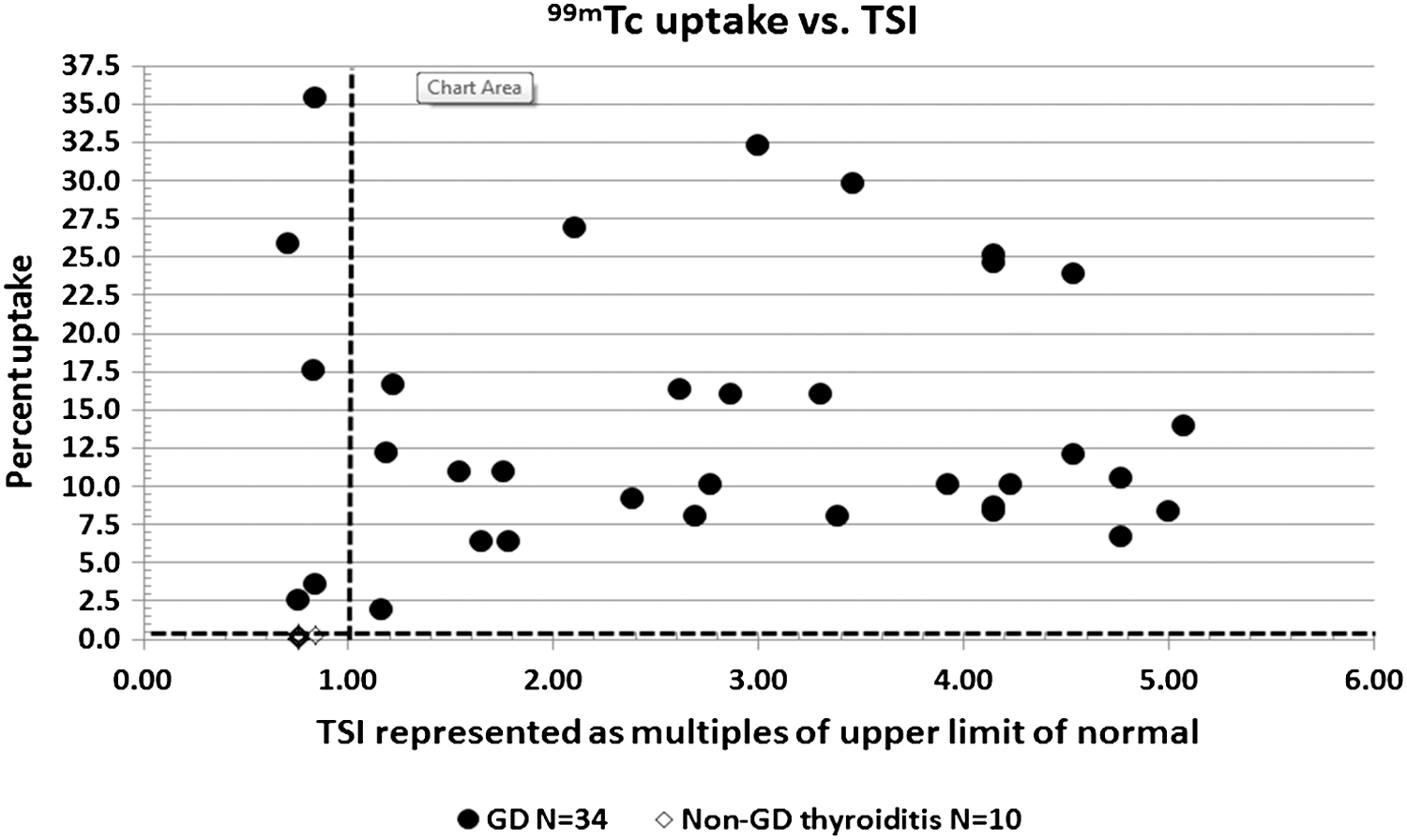
The distribution of absolute values of technetium uptake (99mTc) against the thyroid stimulating immunoglobulins (TSI) represented as upper limits of normal. Values presented on the left of vertical line represent patients with negative TSI with elevated 99mTc uptake on the scan. One of six patients with discordant TSI had elevated uptake, but the uptake was not quantified and is not shown on the graph.
Discussion
99mTc uptake has been in use for the evaluation of thyroid function for more than 50 years. Despite its prevalence in Europe, its use remains limited in children presenting with hyperthyroidism in the United States. To our knowledge, our study is the first to evaluate the utility of 99mTc uptake (compared with the more commonly used TSI) in a pediatric population with hyperthyroidism. In our study, we demonstrate that 99mTc uptake has excellent sensitivity and specficity in establishing the cause of hyperthyroidism in a pediatric population. In comparison with 99mTc uptake, TSI had lower sensitivity but an excellent PPV.
Diagnosing the cause of hyperthyroidism (increased TH synthesis from TSH receptor activation vs. increased release of preformed TH from thyroid follicles) may be difficult in children. The presence of TSI supports the diagnosis of GD. However, Rahhal et al. reported TSI negativity in as many as 54% of pediatric patients who presented with GD (3). Another retrospective study evaluating the utility of TSI in the diagnosis of Graves' opthalmopathy reported only 65% TSI positivity at diagnosis of GD (4). In contrast, Botero et al. showed TSI positivity in 10/11 (91%) children with active GD (5). Further, a more recent multicenter study from Europe and America reported 100% sensitivity for TSI for diagnosis of GD in 82 children using the same assay used in this report (6). The variability in TSI sensitivity reported in these studies calls for the use of additional diagnostic tests in establishing the etiology of hyperthyroidism, especially in children.
Assessment of 99mTc uptake by the thyroid is an excellent strategy to differentiate increased TH synthesis from TSH receptor activation (as in GD) compared with increased release of preformed TH (as in non-GD thyroiditis). Despite the extensive use of 99mTc scans in the newborn period for diagnosis of congenital hypothyroidism, the role of 99mTc uptake in the diagnosis of pediatric hyperthyroidism is less well studied. A study from Japan evaluating the 99mTc uptake as a predictive test to determine outcomes of thyrotoxicosis in adult patients demonstrated a significant correlation of uptake with levels of TH and TSH receptor stimulating antibody (13). A more recent study evaluated the relationship between second-generation thyrotropin receptor antibody (TRAb) assays and 99mTc uptake in patients with untreated autoimmune hyperthyroidism, and found a significant association between antibody levels and 99mTc uptake (14). This study, performed primarily in adults, assessed TRAb levels but not their biological activity measured with cyclic-AMP production. This test is less sensitive than TSI (2,6). In patients diagnosed by 99mTc uptake, Kamijo et al. established cutoff values for TRAb levels to differentiate GD from painless thyroiditis. Nevertheless, no comparison with 99mTc uptake was performed in the study, and 99mTc was considered the gold standard (15). Our study is unique in having evaluated and compared the utility of both 99mTc uptake and TSI in all patients simultaneously. Additionally, we assessed the utility of these tests in the two common conditions causing pediatric hyperthyroidism.
There were no differences in clinical characteristics of patients among the diagnostic groups in terms of age at presentation or sex. Furthermore, despite being a significant distinguishing factor between the two groups, thyroid enlargement was not found on physical examination in 5/37 patients in the GD group, indicating the need for additional diagnostic tests to identify the etiology.
With respect to laboratory evaluations, we were able to demonstrate significantly higher free T4 and total T3 levels in patients with GD compared with non-GD thyroiditis patients, supporting the greater severity of hyperthyroidism in patients with GD. In all non-GD thyroiditis patients, total T3 levels were less than twice the ULN. Free T4 levels were elevated to less than twice the ULN in 9/10 non-GD patients. These data suggest that the degree of elevation of free T4 and total T3 in patients with hyperthyroidism might be helpful in distinguishing GD from non-GD thyroiditis patients.
Radionuclide uptake studies are considered the gold standard in differentiating hyperthyroidism caused by increased TH synthesis versus increased release of preformed TH. In our study, 99mTc upake had 100% sensitivity, specificity, and PPV and NPV in differentiating GD from non-GD thyroiditis. Compared with 99mTc uptake, TSI had a slightly lower sensitivity of 84% in diagnosing GD in our pediatric population. Despite the lower sensitivity, TSI had 100% specificity and PPV for diagnosing GD. The degree of agreement between the two tests was quite high at 0.69.
We compared the clinical characteristics of the six GD patients with negative TSI against the GD patients with positive TSI. There were no statistically significant differences between the groups for age at presentation, sex distribution, or degree of free T4/total T3 elevation, 99mTc uptake, or thyroid enlargement. This is in contrast with the findings reported earlier in a study of adults in which antibody negative GD patients were characterized by mild elevation of TH, mildly elevated 123I uptake, weak TSI activity, and small goiters (16). Furthermore, in our study, we did not find any correlation between age of GD presentation and TSI positivity.
Both GD and activating mutations of the TSH receptor can present with clinical and biochemical hyperthyroidism and are difficult to distinguish in the absence of supporting evidence for GD. Even though the presence of auto-antibodies (TSI, other auto-antibodies such as thyroglobulin, and thyroid peroxidase antibodies) and eye findings strongly suggest a GD diagnosis, the possibility of a TSH receptor mutation cannot be excluded definitively in patients who are TSI negative. In five of our six patients with TSI negative hyperthyroidism and non-suppressed 99mTc uptake, the presence of eye findings (two of six), TSI positivity on a repeat test (two of six), and presence of other auto-antibodies (one of six) make GD the most likely diagnosis. However, an activating mutation in the TSH receptor is possible in the patient who presented at three and a half years of age and underwent thyroidectomy one and a half years later without achieving presurgical remission. Because of the cost associated with gene sequencing and the relatively low prevalence of activating mutations (4.5% of all patients presenting with diffuse goiter and negative thyrotropin receptor antibodies) (17), this distinction is typically not sought in a clinical setting but nevertheless is important for discussion.
At our institution, a 99mTc scan costs approximately two and a half times as much as a blood test for TSI. While 16% of our subjects might have required the 99mTc uptake test in addition to TSI for accurate diagnosis of GD, most children with GD would have been diagnosed with TSI alone. Without doubt, 99mTc uptake is an excellent diagnostic tool for diagnosis of hyperthyroidism. Nevertheless, the additional costs and radiation exposure of such uptake studies need to be factored into the choice of diagnostic tests during the process of decision making.
The relatively small number of patients in each of the non-GD thyroiditis groups is a limitation of our study. In addition, the significant elevation of free T4 and total T3 levels in the GD group compared with the non-GD thyroiditis groups might be related to small numbers in the latter groups. Another limitation of our study is the lack of data on iodine consumption in these children, a determinant of Tc uptake.
Conclusion
99mTc uptake has excellent sensitivity and specificity in diagnosing GD and differentiating such patients from those with hyperthyroidism from increased release of preformed TH. However, despite its lower sensitivity compared to 99mTc uptake, TSI alone is sufficient for the diagnosis in most cases of pediatric hyperthyroidism. Given the additional costs associated with 99mTc uptakes (two and a half times as much as TSI at our institution), it seems reasonable to reserve 99mTc uptakes for those patients with unclear etiology who are TSI negative.
Footnotes
Acknowledgments
This study was supported by funding from NIH grants T32DK007260 and K24HD071843.
Author Disclosure Statement
We have no financial disclosures or conflicts of interest.