
Abstract
Background:
Malignant struma ovarii (MSO) is a germ cell tumor of the ovary histologically identical to differentiated thyroid cancers. There is a paucity of data on this neoplasm, with fewer than 200 reported cases. The primary objective of this study was to examine the survival rate of women diagnosed with MSO using data from the Surveillance, Epidemiology, and End Results (SEER) database. Secondary objectives were to describe the demographic, clinical, pathologic, and treatment characteristics of this population.
Methods:
A retrospective analysis was performed of prospectively collected cancer registry data. A total of 68 patients were identified in the SEER database, 1973–2011. The chi-square test, Student's t-test, and Kaplan–Meier curves were employed for data analyses.
Results:
All 68 patients were females with a mean age at diagnosis of 43.0 years. Nearly 33% underwent unilateral oophorectomy, 28.6% bilateral oophorectomy, and 28.6% oophorectomy and omentectomy, and 4.8% were treated with debulking surgery. Pelvic radiation was administered to 12.3% of patients. The mean tumor size was 52.8 mm; 80% of malignant struma ovarii were SEER staged as local. Overall survival rates at 5, 10, and 20 years were 96.7%, 94.3%, and 84.9% respectively. Among the patients, there were six deaths recorded; only one was attributed to MSO. Six individuals (8.8%) had a concomitant or subsequent diagnosis of thyroid cancer. Four patients underwent total thyroidectomy, three patients had radioactive iodine, and one patient underwent external beam radiation. Two thirds of thyroid cancers extended outside the thyroid gland. All six patients with thyroid cancer were alive at the end of follow-up.
Conclusions:
It was observed that patients with malignant struma ovarii had an excellent disease-specific survival rate, regardless of the management strategy employed. However, MSO patients had a high risk for developing aggressive thyroid cancers. Therefore, MSO patients may benefit from routine thyroid imaging once the diagnosis of MSO is established.
Introduction
S
Little is known about this rare entity. In a recent review of the medical literature, Marcy et al. stated that there are fewer than 200 cases reported in the medical literature (6). Given this paucity of data, the impact on life expectancy of MSO remains controversial, and its optimal management is currently debated (7 –10). Most authors advocate for an aggressive treatment based on local surgery, followed by total thyroidectomy, radioactive iodine ablation (RAI), and thyroid hormone suppressive therapy regardless of the presence of distant metastases at time of diagnosis (11 –15).
The aim of the current study was to utilize the Surveillance, Epidemiology, and End Results (SEER) database in order to gather a sufficiently large cohort of patients to investigate survival rates associated with this malignancy, as well as to describe demographic, clinical, pathologic, and treatment characteristics of patients diagnosed with MSO.
Materials and Methods
Data sources and study patients
The National Cancer Institute's (NCI) SEER database was used to identify patients diagnosed with MSO (16). The SEER database employs the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) for histology reference; code 9090 identifies MSO (17). The SEER Program includes 18 cancer registries; together, they accrue data from nearly 28% of the U.S. population. Data are collected from 18 geographic areas across the nation: 10 state registries (Connecticut, Georgia, Greater California, Hawaii, Iowa, Kentucky, Louisiana, New Jersey, New Mexico, and Utah), five metropolitan area registries (metropolitan Atlanta and rural Georgia, San Francisco–Oakland and San Jose–Monterey, Los Angeles, Seattle–Puget Sound, and Detroit), and three Native American registries (Alaska Native Tumor Registry, Arizona Indians, and the pilot Cherokee Nation Cancer Registry) (18).
Demographic variables of interest were patient sex, age at diagnosis, race/ethnicity, Hispanic origin, marital status, year of diagnosis, and geographic area. Age at diagnosis was treated as a continuous variable. Race/ethnicity was recoded as white, black, or other (American Indian, Alaska Native, Asian, Pacific Islander, and other unspecified). Marital status was dichotomously treated as yes (married and domestic partner) or no (single, divorced, widowed, or separated). Year of diagnosis was divided into two study intervals: 1973–1999 and 2000–2011. Geographic areas were Northeast, South, Midwest, and West.
Clinical information included surgery of primary site, pelvic radiation, survival status as of December 31, 2011, number of primary tumors per patient, and tumor marker CA-125. Surgery was divided into five subcategories: none, unilateral oophorectomy, bilateral oophorectomy, unilateral or bilateral oophorectomy with omentectomy, or debulking surgery. Radiation was coded as none, external beam radiation therapy (EBRT), RAI, or a combination of RAI and EBRT. Number of primary malignancies was grouped into 1, 2, or ≥3. CA-125 values were recorded only from blood or serum prior to treatment. Normal values may vary with patient age and laboratory methods of analysis; the typical reference levels range between 0 and 35 μg/mL.
Pathologic variables were tumor size, laterality, SEER stage, and lymph node status. Tumor size was analyzed as a continuous variable. The SEER stage provides a standardized and simplified measure of disease progression to ensure consistent definitions over time (18). A cancer is described as in situ if it presents only in the layer of cells in which it originated; localized when it is limited to the primary organ; regional if it has spread beyond the primary site to nearby lymph nodes, organs, or tissues; and distant when it has spread to distant organs or lymph nodes. For the purpose of this analysis, in situ and localized cancers were combined into local stage. Lymph node status was categorized as none (no lymph nodes were examined), negative (lymph nodes were examined and were all negative), or positive.
Statistical analyses
Demographic, clinical, and pathologic characteristics of patients were described utilizing simple summary statistics; categorical and continuous variables were analyzed utilizing chi-square analysis and Student's t-test. Kaplan–Meier probabilities of overall survival were estimated with exact confidence intervals at 5, 10, and 20 years of follow-up (19). The standardized incidence ratio (SIR) of thyroid cancer was estimated by dividing the observed number of thyroid cancer cases among MSO females by the expected number of thyroid cases among the same cohort. The expected number of thyroid cancer cases was derived from age-specific incidence rates in the 2000 US Census and age-specific follow-up periods (in years) in the MSO cohort. Exact confidence intervals for SIR were also estimated (20).
Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) software (version 22.0; SPSS Inc., Chicago, IL), and exact confidence intervals estimated using R software v3.1.0. All tests were two-sided, and a p-value of <0.05 was considered statistically significant. Because SEER data are publicly available and all patient information is de-identified, this study was granted an exemption from the institutional review board.
Results
Characteristics
A total of 68 patients diagnosed with MSO were identified in the SEER database between 1973 and 2011. The follow-up duration ranged from 2 months to 34 years, with a mean of approximately 8 years (SD=7.3 years). All patients were female with an ovarian diagnosis of MSO. Age at diagnosis ranged from 16 to 79 years, with a mean of 43.0 years (Table 1). Almost three-quarters of patients were white, and most patients were married (68.2%) and diagnosed after 2000 (82.4%); 42.6% lived in the West region.
SEER, Surveillance, Epidemiology, and End Results; EBRT, external beam radiation therapy; RAI, radioactive iodine ablation; NOS, not otherwise specified.
Approximately 33% were treated with unilateral oophorectomy, 28.6% with bilateral oophorectomy, and 28.6% with oophorectomy and omentectomy, and 4.8% underwent debulking surgery; 4.8% of women did not undergo surgery. Radiation was not commonly administered as part of the treatment algorithm: 87.7% of patients did not receive any form of radiation, while 3.1% were treated with EBRT and 7.7% with RAI, and only 1.5% received a combination of the two. CA-125 was reported for 14 patients; 35.7% of these tested positive.
MSO had a mean tumor size of 52.8 mm (range 1–200 mm), and it was equally distributed between left and right ovaries. The vast majority of MSO had a SEER stage that was deemed to be local (80%). When stratified by SEER stage, no differences were observed in the distribution of age, race/ethnicity, laterality, and tumor size (p>0.05). Lymph nodes were often not examined (73.3%); of the lymph nodes that were removed and examined, none was found to be positive for metastases.
Ten individuals had more than one SEER record due to unrelated cancer diagnoses; six had a separate thyroid cancer diagnosis (TC; Table 2). All thyroid malignancies were diagnosed concomitantly or subsequently to MSO; one patient was diagnosed with follicular thyroid cancer, one had minimally invasive follicular thyroid cancer, one presented with insular thyroid cancer, and three had papillary thyroid cancer. Among the papillary thyroid cancers, there were classic, diffuse sclerosing, and follicular variants. Four patients underwent total thyroidectomy, three patients had RAI, and one patient underwent EBRT. Thyroid neoplasms arising in patients with a diagnosis of MSO were deemed to be SEER stage distant in three of six patients. All six patients with thyroid cancer were alive at the end of the follow-up.
Standardized incidence ratio
Using age-specific incidence rates from the standard 2000 U.S. population and the age-specific follow-up period for the MSO cohort, we calculated an expected number of 0.08 TC cases. Based on the observed incidence of six TC cases, the estimated SIR for TC was 79.8 [CI 29.3–173.6].
Survival analysis
Overall survival rates at 5, 10, and 20 years were 96.7% [CI 2.3–99.9], 94.3% [CI 2.0–99.9], and 84.9% [CI 1.0–99.9] respectively (Fig. 1). Among the MSO patients, only six (8.8%) died; one succumbed to MSO specifically, two to heart disease, one to kidney disease, and one to another cancer, and one died of unspecified causes.
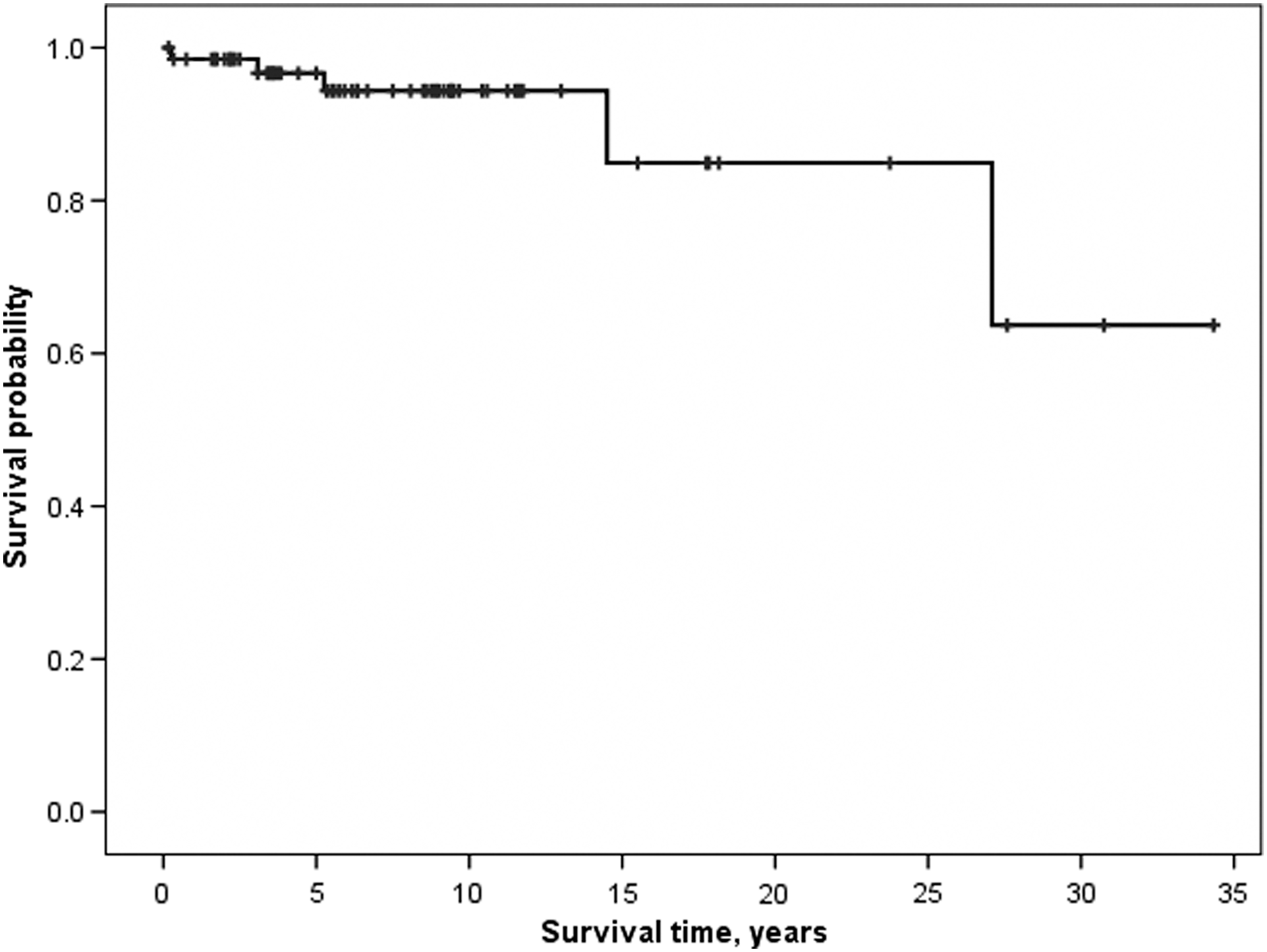
Overall survival of malignant struma ovarii over time, Surveillance, Epidemiology, and End Results 1988–2011.
Discussion
The current study analyzes one of the largest series of patients diagnosed with malignant struma ovarii. A mean age at diagnosis of 43 years was identified. Patterns of care appeared to be variable. Nevertheless, patient survival was excellent; indeed, only one disease-specific death was observed over the follow-up time. Nine percent of patients also had a documented primary thyroid cancer in the neck; the cancer was confined to the thyroid gland in only 33% of cases. Hence, these individuals appeared to present with a more invasive form of the disease than usually expected for differentiated thyroid cancers.
In 2009, Robboy et al. published a study of 88 patients with MSO, including a personal series and cases culled from the larger literature (21). Overall survival rates for all patients were 89% at 10 years and 84% at 25 years; based on these findings, they argued for routine long-term follow-up. The data from the current study indicate that both the disease-specific and overall survival rates for patients with MSO are very good, suggesting that long-term follow-up may be reserved for selected patients with more invasive disease.
A case of a 42-year-old woman with synchronous bilateral multifocal papillary thyroid cancer and MSO was described by Leong et al. (12). The thyroid-type cancers from the thyroid and ovary were different in tissue histology and levels of cytokeratin-19 expression, supporting the independent existence of two cancers. The authors hypothesized that “field cancerization” and early genomic instability may explain multifocality in all thyroid-type tissue. This is in line with the findings of Schmidt et al. After analyzing six patients with malignant struma ovarii and nine with benign struma ovarii in 2007, they found BRAFV600E gene mutations in four of the MSO specimens, suggesting a common pathogenesis for all papillary thyroid cancers, regardless of body location (22). In a review of the literature from 2013, Leite et al. analyzed the clinical dilemma of papillary carcinoma arising in struma ovarii versus thyroid cancer metastasis to the ovary from a primary thyroid cancer in the neck (23). Besides family history and a physical examination followed by an ultrasound of the thyroid gland, the authors reported that unique characteristics on ovarian magnetic resonance imaging might help to differentiate the two diseases. The age-adjusted incidence for thyroid cancer for the general U.S. population from 1975 to 2011 was 11.26 new cases/year per 100,000 females; given a patient cohort of this size, with a mean follow-up time of 8.3 years, it was expected that there would be fewer than one case (∼0.08) of thyroid cancer in the cohort of the current study (24). Conversely, six patients had a diagnosis of thyroid cancer, showing a significant excess of thyroid malignancies cases among the MSO cohort compared to the standard U.S. population (SIR=79.8). This diagnosis was made simultaneously with, or following, the diagnosis of MSO. This may reflect an increased incidence of thyroid cancer due to surveillance bias, since patients with MSO are likely to receive a screening neck ultrasound, or incidentalomas found during subsequent thyroidectomies performed as part of the MSO management. Nonetheless, these individuals presented with more invasive disease than typically expected with differentiated thyroid cancer. Indeed, out of six patients, three were given a SEER stage of distant, one of regional disease, and just two of local disease. These results may be interpreted in two ways. One interpretation is that patients with MSO appear to be predisposed to having thyroid cancer and more aggressive thyroid cancer. Another interpretation could be that in this series, patients with a more aggressive primary thyroid cancer metastatic to the ovary were coded as having MSO. However, this latter interpretation is less likely, given the clear and rigorous SEER cancer coding.
In 2012, Marti et al. published a series of four patients and reviewed 53 reported cases from the literature describing the surgical management of differentiated thyroid cancer arising in struma ovarii (8). After a median follow-up of nine years, all four patients were alive with no evidence of disease. The 25-year recurrence rate of the 57 cases from the literature was 7.5% in spite of a variety of different surgical and adjuvant treatments. The authors concluded that radical pelvic surgery and prophylactic total thyroidectomy may be restricted to those patients with extra-ovarian spread or distant metastases. The findings of the current study appear to support such conclusions; 68 patients were treated with different combinations of surgical and radiation therapy in spite of the variation in care, only one patient died of disease-specific causes. In spite of an 80% rate of SEER-staged local cancers, 57.2% of patients underwent a more invasive surgical resection than a simple oophorectomy. Therefore, MSO might be overtreated, and this might impact long-term the quality of life and fertility of affected women, given the young mean age of diagnosis and the fact that many undergo bilateral oophorectomy as part of their treatment.
The limitations of the present study include those inherent to the SEER database, such as coding errors and lack of data on variables that would have been informative (e.g., pregnancies, cancer recurrence, chemotherapy, reoperations, and pertinent biochemical and genetic laboratory studies). Site of metastatic disease was not captured in SEER. Therefore, some of the distant spread MSOs might theoretically have been miscoded and represented instead synchronous primary thyroid cancer or its metastases, and, similarly, some of the metastatic TCs might have actually been synchronous MSO or its metastases. Nevertheless, SEER has been well validated for oncology studies, and this is therefore less likely to explain the findings of this study (25,26).
In conclusion, MSO appears to be associated with an excellent disease-specific survival rate, regardless of the management strategy employed. In addition, patients with a diagnosis of MSO appear to be at higher risk of developing aggressive thyroid cancers. Therefore, thyroid imaging for case finding of thyroid tumors might be prudent once the diagnosis of MSO is established. Efforts should be pursued to standardize the care of patients with MSO, perhaps with practice guidelines. It is hoped that population-level data such as these will be a first step in this process.
Footnotes
Acknowledgments
Paolo Goffredo was supported by the Italian Foundation for Cancer Research (Fondazione Italiana per la Ricerca sul Cancro—FIRC). Anna M. Sawka holds a Health Services Research Chair funded by Cancer Care Ontario.
Author Disclosure Statement
The authors have nothing to disclose.