
Abstract
Background:
Antithyroid drug (ATD)-induced severe hepatotoxicity is a rare but serious complication of ATD therapy. The characteristics of severe hepatotoxicity have been reported in only a small number of patients.
Method:
Ninety patients with ATD-induced severe hepatotoxicity presenting during a 13 year period (2000–2013) who were about to undergo nuclear medicine therapy with 131I from a sample of 8864 patients with hyperthyroidism were studied, and the outcomes were evaluated.
Results:
The mean age of the patients with ATD-induced severe hepatotoxicity was 41.6±12.5 years (mean±standard deviation), and the female to male ratio was 2.2:1. The methimazole (MMI) dose given at the onset was 19.1±7.4 mg/day. The propylthiouracil (PTU) dose given at the onset was 212.8±105.0 mg/day. ATD-induced severe hepatotoxicity occurred in 63.3%, 75.6%, and 81.1% of patients within 4, 8, and 12 weeks of the onset of ATD therapy, respectively. The types of severe hepatotoxicity did not differ significantly between the MMI and PTU groups (p=0.188). The frequency of the cholestatic type in the MMI group (35.3%, 18/51) was higher than that in the PTU group (17.9%, 7/39), but these frequencies were not significantly different (p=0.069). The patients who were treated with 131I received an average dose of 279.1±86.1 MBq (n=84). Therapy was successful in 60 of the 67 patients (89.6%). The success rate was equivalent (p=0.696) between the groups receiving MMI (91.7%, 33/36) and PTU (87.1%, 27/31).
Conclusions:
Severe hepatotoxicity tends to occur within the first three months after the onset of ATD therapy. The type of ATD-induced severe hepatotoxicity did not differ between the MMI and PTU groups. 131I therapy is an effective treatment approach for patients with ATD-induced severe hepatotoxicity.
Introduction
I
Severe hepatotoxicity commonly occurs suddenly in the early stages of ATD treatment according to a small number of case reports and reviews. No studies with a large number of patients have demonstrated the characteristics of this complication because of its low incidence. Adverse side effects from ATDs occur in patients with hyperthyroidism, especially patients with ATD-induced severe hepatotoxicity, and 131I treatment is an alternative choice for these patients. Medical information about patients who were evaluated for 131I treatment was collected, including their age, sex, time to onset of adverse reactions, types of adverse reactions, dose at onset, treatment details, and outcomes. This information was obtained from the Department of Nuclear Medicine at the First Affiliated Hospital, College of Medicine, Zhejiang University, covering a period of 13 years (2000–2013). Ninety cases presenting with ATD-induced severe hepatotoxicity were studied.
Materials and Methods
Study patients
The records of patients with hyperthyroidism who were about to undergo therapy with 131I at the Department of Nuclear Medicine at Zhejiang University from January 2000 to July 2013 were retrospectively reviewed. During that time, 8864 patients (6306 female) with hyperthyroidism were referred to the Department of Nuclear Medicine for radioiodine therapy. Details of those patients who were confirmed to have ATD-induced severe hepatotoxicity according to the following criteria were collected. First, all patients were diagnosed with Graves' disease according to clinical findings and on the basis of a technetium-99m scan showing diffuse uptake of the isotope or an elevated radioactive iodine-131 uptake. In each case, hyperthyroidism was confirmed based on increased concentrations of plasma free thyroxine (fT4) and/or free triiodothyronine (fT3) and by a decreased concentration of thyrotropin (TSH) (4). Second, data from all patients who were confirmed to have normal liver function tests before taking ATD were collected. Third, the signs and symptoms of acute, viral-like hepatitis were used to alert clinical suspicion. Laboratory investigations confirmed hepatic dysfunction. The criteria for severe hepatotoxicity and the three types of hepatotoxicity in patients taking ATDs according to the guidelines proposed by Tajiri et al. are as follows (8): serum alanine aminotransferase (ALT) more than eight times the upper limit of normal (ULN) or ALT more than five times the ULN for two weeks, which is defined as the hepatocellular type; ALT more than three times the ULN in association with a serum total bilirubin (TB) level more than two times the ULN or prothrombin time international ratio (PT-INR) prolonged more than one and a half times, which is defined as the mixed type; and symptoms of liver injury with TB more than three times the ULN or a PT-INR prolonged more than one and a half times, which is defined as the cholestatic type. Finally, severe hepatotoxicity patients with viral hepatitis, autoimmune hepatitis, alcoholic liver disease, liver cirrhosis, cholangitis, cardiac insufficiency, and toxicity from other drugs, such as Chinese herb-induced liver dysfunction, were excluded.
A total of 90 patients with Graves' disease who developed ATD-induced severe hepatotoxicity complications were selected from 8864 patients. All treated patients provided written informed consent before the 131I treatment and were aware of the radiation safety precautions following treatment. The study was approved by the institutional review board.
The age, sex, time of severe hepatotoxicity onset, type of hepatotoxicity, prognosis, and other medical information for all patients were also analyzed.
Methods and outcomes assessment
ATD therapy was discontinued at least two weeks before the patients were treated with 131I. Over the study period, based on the ATA guidelines (4), both fixed dose and thyroid weight-adjusted dose calculations were applied to treat hyperthyroidism with 131I: 25 patients were offered a single fixed dose of 131I (296 MBq) from 2000 to 2006, and 59 patients were given a thyroid weight-adjusted dose of 131I from 2007 to 2013.
131I therapy was considered successful if the patient was either hypothyroid or euthyroid in the absence of all antithyroid drugs one year after radioiodine treatment. Treatment failure was defined as recurrent hyperthyroidism according to elevated fT3 and fT4 levels (9).
Statistical analyses
Descriptive quantitative data are expressed as the mean±standard deviation (SD); qualitative data are expressed as percentages. Significant differences between the groups were ascertained using analysis of variance (quantitative variables) or the chi-square test (qualitative variables). When expected values of <5 were included in the data table, Fisher's exact probability test was used instead of the chi-square test. Calculations were performed using SPSS for Windows v16 (SPSS, Inc., Chicago, IL). Statistical significance was defined as p<0.05.
Results
Analysis of the clinical characteristics of 90 patients with ATD-induced severe hepatotoxicity
Ninety cases of ATD-induced severe hepatotoxicity at the Department of Nuclear Medicine from January 2000 to July 2013 were studied. An average of seven patients per year was reported. The number of reports increased every year until 2006, which was likely due to the increase in endocrinologist awareness of ATD complications. The clinical characteristics of the 90 patients with ATD-induced severe hepatotoxicity are shown in Table 1. Age, sex, the time of the onset of severe hepatotoxicity, and the type of hepatotoxicity did not differ between the MMI and PTU groups. One patient was diagnosed with agranulocytosis when he had severe hepatotoxicity at the same time after taking 20 mg/day of MMI for four weeks.
Including one week cases; #including one and two week cases.
ATD, antithyroid drug; MMI, methimazole; PTU, propylthiouracil; SD, standard deviation.
The female to male ratio was 2.2:1. There was no significant difference in the female to male ratio (p=0.327) between these two groups. The patient age ranged from 20 to 72 years, and the mean age was 41.6±12.5 years (mean±SD). The incidences of severe hepatotoxicity were 18.9%, 21.1%, 28.9%, 22.2%, 7.8%, and 1.1% among patients in their 20s, 30s, 40s, 50s, 60s, and 70s, respectively. Most patients (91.1%) were between the ages of 20 and 50 years (Fig. 1). The mean ages were 42.9±12.8 and 39.9±12.0 years in the MMI and PTU groups, respectively (p=0.257); thus, the two groups were equivalent.
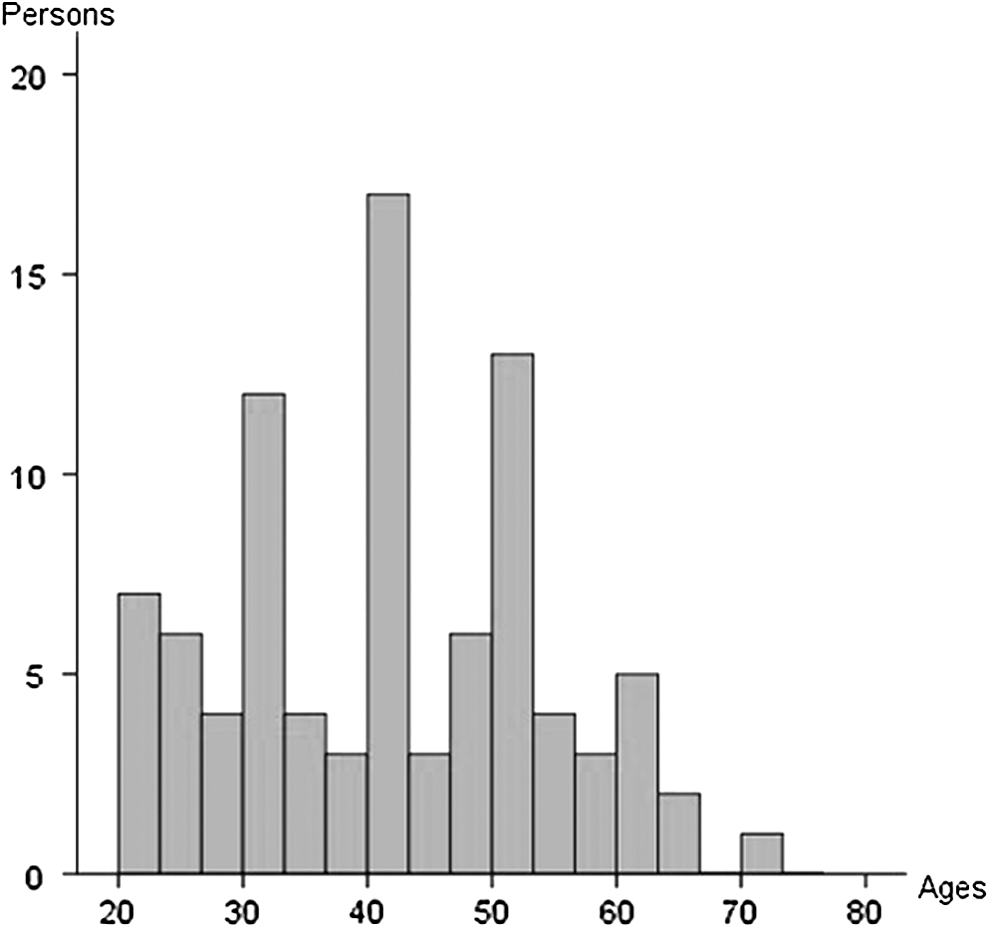
The age distribution of patients with antithyroid drug (ATD)-induced severe hepatotoxicity. The mean age was 41.6±12.5 years (mean±standard deviation) in 90 patients.
When these patients were diagnosed with severe hepatotoxicity, 51 patients were treated with MMI and 39 patients were treated with PTU. Most patients (65.7%) were given MMI, reflecting the fact that MMI is more commonly administered than PTU in China. Seven patients had a history of taking another ATD before they had severe hepatotoxicity. Six patients were switched from PTU to MMI for the following reasons: three developed PTU-induced granulocytopenia after taking PTU for one week, two developed cutaneous reactions after taking PTU for two weeks, and one relapsed after taking PTU for two years. In addition, one patient was switched from MMI to PTU because of MMI-induced liver injury within six months. The average dose of MMI given at the onset of severe hepatotoxicity was 19.1±7.4 mg/day in 51 patients. PTU was used for only 39 patients, and the mean dose at the onset of severe hepatotoxicity was 212.8±105.0 mg/day.
The numbers of days before the onset of severe hepatotoxicity and after the initiation of ATD therapy are shown in Figure 2. Severe hepatotoxicity occurred in 63.3%, 75.6%, and 81.1% of patients within 4, 8, and 12 weeks, respectively. There were no differences in the number of weeks between the MMI and PTU groups. In addition, 17 patients developed severe hepatotoxicity after 12 weeks. Six percent (n=5) of the patients were reported to have developed severe hepatotoxicity more than one year after starting ATD treatment. However, most of these patients had resumed treatment after a discontinuation or have been re-exposed to the ATD after a change in the dose.

Time to the onset of severe hepatotoxicity after taking of ATD therapy in 90 patients. Severe hepatotoxicity occurred in 63.3%, 75.6%, and 81.1% after 4, 8, and 12 weeks of treatment, respectively. After three months, 17 patients developed severe hepatotoxicity.
A summary of the frequency of the type of severe hepatotoxicity in the two groups is presented in Table 1. There were no significant differences between the MMI and PTU groups (p=0.188). The hepatocellular, cholestatic, and mixed types occurred in 43.1%, 35.3%, and 21.6% of the MMI patients, respectively, and in 56.4%, 17.9%, and 25.6% of the PTU patients, respectively. The frequency of the cholestatic type in the MMI group (35.3%, 18/51) was higher than that in the PTU group (17.9%, 7/39), but this difference was not significant (p=0.069).
Therapy outcomes of the patients with ATD-induced severe hepatotoxicity
Six patients did not receive radioiodine therapy because they withdrew their consent. Eighty-four patients were treated with radioiodine after they were diagnosed with severe hepatotoxicity and after they had discontinued ATD for at least two weeks. Seventeen of the 84 patients who received radioiodine were lost to follow-up (Fig. 3).
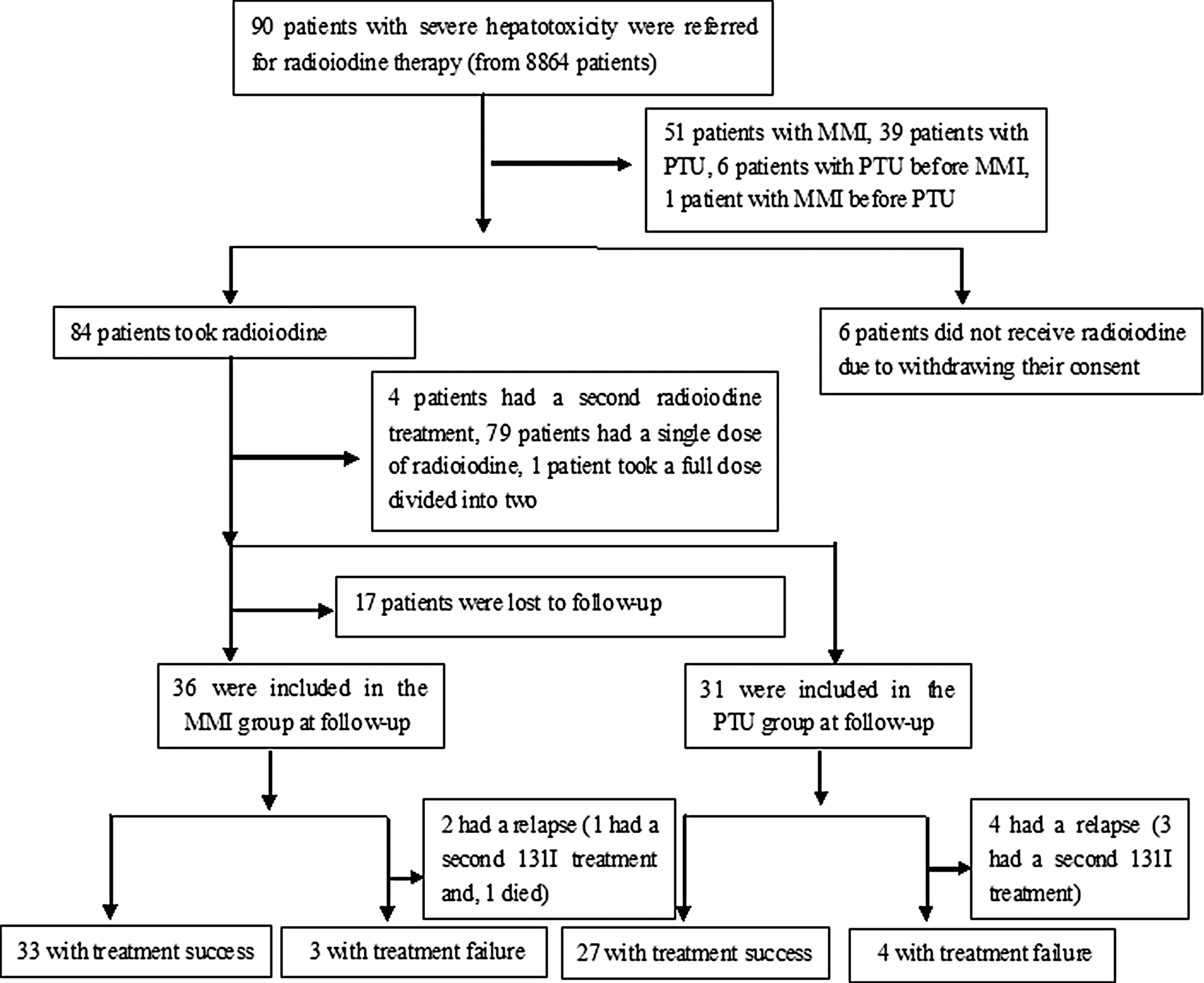
Flow and follow-up of the study patients.
The average dose in the patients who were treated with 131I was 279.1±86.1 MBq (n=84), with a range of 74–518 MBq. The mean doses were 272.5±89.6 and 287.5±81.9 MBq in the MMI and PTU groups, respectively (p=0.430); thus, there was no significant difference in dose between the two groups. Of the 84 patients, a single dose of radioiodine was administered to 83 patients; only one patient received the total dose divided into two doses, with two thirds of the dose given on day 1 and one third of the dose given on day 3. Four of the 84 patients received a second radioiodine treatment at least six months after the first treatment. The success rate was 89.6% in the 84 patients who received 131I therapy. The rates of successful therapy were estimated at 91.7% and 87.1% in the groups who received MMI and PTU, respectively (p=0.696); thus, the two treatments were not significantly different. A second 131I treatment was administered to four of the seven patients who failed to respond to therapy and who had hypothyroidism after one year; two refused additional therapy after the first 131I treatment course. One patient was diagnosed with MMI-induced severe cholestatic hepatotoxicity within nine weeks after initiating treatment with 20 mg/day MMI; this patient died one week after radioiodine therapy because of progressively worsening liver function and complications.
Discussion
In this study including 8864 patients treated at the Department of Nuclear Medicine at Zhejiang University in China, ninety cases of ATD-induced severe hepatotoxicity were identified, and several important findings were uncovered. ATD-induced severe hepatotoxicity is rare; the incidence was 1.0% in the current study, which is higher than that reported in the literature (0.01%) (5,6). This discrepancy could be due to the fact that the criteria used for the diagnosis of severe hepatotoxicity were less strict. Indeed, the previously reported patients appeared to be more sick (6,10) with more severe liver enzyme abnormalities than the abnormalities used for the diagnosis in the current study. Ascertainment bias may have occurred among endocrinologists, as patients who are routinely monitored by liver function tests are more likely to be treated. It was found that severe hepatotoxicity is more likely to occur in females than in males, which is in agreement with previous reports (10). The reason for the female predominance may be the higher female-to-male ratio (2.4-10:1) among patients with Graves' disease (3,11). Thus, women are more likely than men to receive ATD therapy. Williams et al. (10) revealed that there were more case reports of PTU hepatotoxicity in women than men, with an overall female-to-male ratio of 8.3:1. The low sex ratio (2.2:1) of hepatotoxicity in the current study is similar to the sex ratio of 2.46:1 in the overall Graves' disease population, and may be the result of differences in the ethnicity of the subjects, the inclusion criteria, and the population sample. Graves' disease can occur at any age. However, the peak incidence is between 40 and 60 years of age. It was found that patients in the 20–50 year age group were more susceptible to severe hepatotoxicity. Because the incidence of severe hepatotoxicity is very low, a very large comparison group is necessary, and it is possible that the sample size of 90 patients may not be sufficient. It was also confirmed that severe hepatotoxicity most often occurs within a few months after the initiation of ATD therapy. More than 60% of patients developed severe hepatotoxicity within four weeks, and more than 80% within 12 weeks. The mean durations of treatment before the development of severe hepatotoxicity were 9 weeks and 10 weeks for MMI and PTU, respectively. The risk of developing severe hepatotoxicity in the early treatment stages, especially within the first three months (10) has been reported in some previous studies (10,12 –14) as well as this study. In the current study, 17 patients developed severe hepatotoxicity four months after starting treatment. Although continuous, vigilant monitoring for severe hepatotoxicity is necessary, particular caution is necessary in the first three months. Surveillance is also necessary when altering the dose and when patients are re-exposed to ATDs after a period of discontinuation.
Second, the MMI dose at the onset of severe hepatotoxicity was 19.1±7.4 mg/day, ranging from 5 mg/day to 30 mg/day in 51 patients, and the PTU dose was 212.8±105.0 mg/day, ranging from 50 mg/day to 600 mg/day in 39 patients. Previous findings have suggested that the side effects of MMI are dose related, while those of PTU are less clearly related to the dose (15). Nakamura et al. (16) reported that 15 mg/day MMI is safer than 30 mg/day MMI, and that PTU induced mild liver damage four times more frequently than 30 mg/day MMI in a prospective randomized clinical trial exploring initial treatments for Graves' disease. Although routine monitoring of liver function in all patients taking ATDs has not been confirmed to prevent severe hepatotoxicity, as the frequency is low (0.01%) and the onset is sudden (5,6), careful monitoring of liver function in patients who are being treated with larger doses of MMI and PTU might be useful in the early detection of hepatotoxicity.
Third, it was found that the hepatocellular, cholestatic, and mixed types of ATD-induced severe hepatotoxicity were present at approximately equivalent rates in the MMI and PTU groups (p=0.188). PTU-induced hepatotoxicity takes the form of allergic hepatitis accompanied by laboratory evidence of hepatocellular injury, often including markedly elevated aminotransferase levels and pathological findings that range from hepatocellular inflammation to submassive or massive hepatic necrosis (6,10,13,17,18). MMI-induced hepatotoxicity is generally considered to be a cholestatic process characterized by preserved hepatocellular architecture, intracanalicular cholestasis and mild periportal inflammation (14,19,20). As far as can be established, this is the first demonstration of the presence of all types of severe hepatotoxicity associated with MMI and PTU therapy in a large sample. The frequency of the cholestatic type in the MMI group (35.3%) was higher than that in the PTU group (17.9%), which is in agreement with previous reports (1,15,19). The mechanism of ATD-induced hepatotoxicity is uncertain. Current data indicate that biotransforming downstream events and their interactions with several environmental and genetic factors could play a role in the proposed model of ATD-induced hepatotoxicity (21,22). Reactive drug metabolites and increased oxidative stress can directly activate inflammatory and immunological pathways. ATDs are not only immunogenic but may also bind through electrostatic forces to available T-cell receptors (23). Their unpredictable idiosyncratic course and chemical heterogeneity further complicate the understanding of the involved mechanisms (24).
Finally, the early recognition of ATD-induced severe hepatotoxicity and intervention are very important. With supportive therapy and immediate discontinuation of ATD, patients should recover a majority of their liver function. However, the exact time required for recovery of liver function is not clear because liver function assessments for some patients were not obtained in the follow-up after 131I treatment. Alexander et al. (25) reported that if a sufficient radioiodine dose is administered, hypothyroidism develops in 80–90% of patients with hyperthyroidism, which is in agreement with the current study. Williams et al. (10) evaluated two of their own cases in conjunction with 28 cases of PTU-induced severe hepatic toxicity described in the literature and reported that seven patients died. In the present study, the death rate (1.11%) was significantly lower than that reported in the literature (from 23% to 41%) (7,10,26,27), which may be attributed to improved understanding and treatment of ATD-induced severe hepatotoxicity in recent years, more inclusive criteria for the diagnosis of severe hepatotoxicity, and the different sample sizes of patients in the various studies.
The limitations of the present study are that the cases were retrospectively reviewed, the sample size was small, and some medical details were missing from the follow-up information for a small subset of patients. Additionally, the exact time required for the recovery of liver function remains unclear. Despite these limitations, this study, which adds to the number of reported cases of ATD-induced severe hepatotoxicity, reveals that all types of severe hepatotoxicity can occur after treatment with MMI and PTU and provides thought-provoking information that will be useful for further studies in this field.
Footnotes
Acknowledgments
This study was supported by the Science and Technology Planning Project of Zhejiang Province (2013C33119, 2012C33091) and the Health Bureau Project of Zhejiang Province (2013KYA069, 2013ZDA008). We would like to thank Dr. Guo-ping Sheng for his constructive comments on our work and Dr. Yi-li Yang, Dr. Zhen-feng Liu, and Dr. Hong-ye Fu for their contributions to the initial study performed on this cohort.
Author Disclosure Statement
No competing financial interests exist.