
Abstract

Dear Editor:
Introduction
The purpose of immunosuppressive treatment in Graves' orbitopathy (GO) is to decrease inflammation and congestion of the orbital tissue (1). High-dose glucocorticoid pulse therapy is the first-line treatment in patients with active, moderate to severe GO (2).
Treatment with supraphysiologic doses of glucocorticoids may suppress the hypothalamic–pituitary–adrenal (HPA) axis. Suppression of the axis may occur even at physiologic doses of exogenous steroids, when used for prolonged period (3).
The aim of the present study was to assess the adrenal reserve in patients with GO, following the currently used intravenous (i.v.) glucocorticoid pulse therapy (2).
Materials and Methods
A total of 32 patients (25 females) with GO, aged 59±12 years, were studied. The patients received treatment with i.v. glucocorticoids, in accordance with the European Group on Graves' Orbitopathy (EUGOGO) protocol (weekly doses of 500 mg methylprednisolone i.v. for six weeks followed by 250 mg per week for another six weeks). All patients were euthyroid at initiation of treatment. Patients with chronic hepatitis B or C infection were given antiviral prophylaxis, and those with a positive tuberculin test were given chemoprophylaxis during glucocorticoid therapy.
The patients underwent a standard dose ACTH stimulation test (Synacthen 250 μg i.v.) 7–15 days after completion of the above regimen. Serum cortisol was measured before, and 30 and 60 minutes after the administration of Synacthen. A cutoff value of stimulated plasma cortisol, where adrenal insufficiency can be ruled out, was set at ≥18 μg/dL (3).
Results
The treatment was generally well tolerated, and no side effects were reported, apart from reversible hepatotoxicity in one patient. Following therapy, there was improvement in the indices of activity and severity of GO (results not shown). The mean level of cortisol was 11.8±4.3 μg/dL at baseline, 24.3±4.1 μg/dL at 30 minutes, and the peak response at 60 minutes, after ACTH stimulation, was 29.7±4.5 μg/dL, indicating sufficient adrenal reserve (Fig. 1). The peak cortisol response was sufficient (≥18 μg/dL) in all 32 patients.
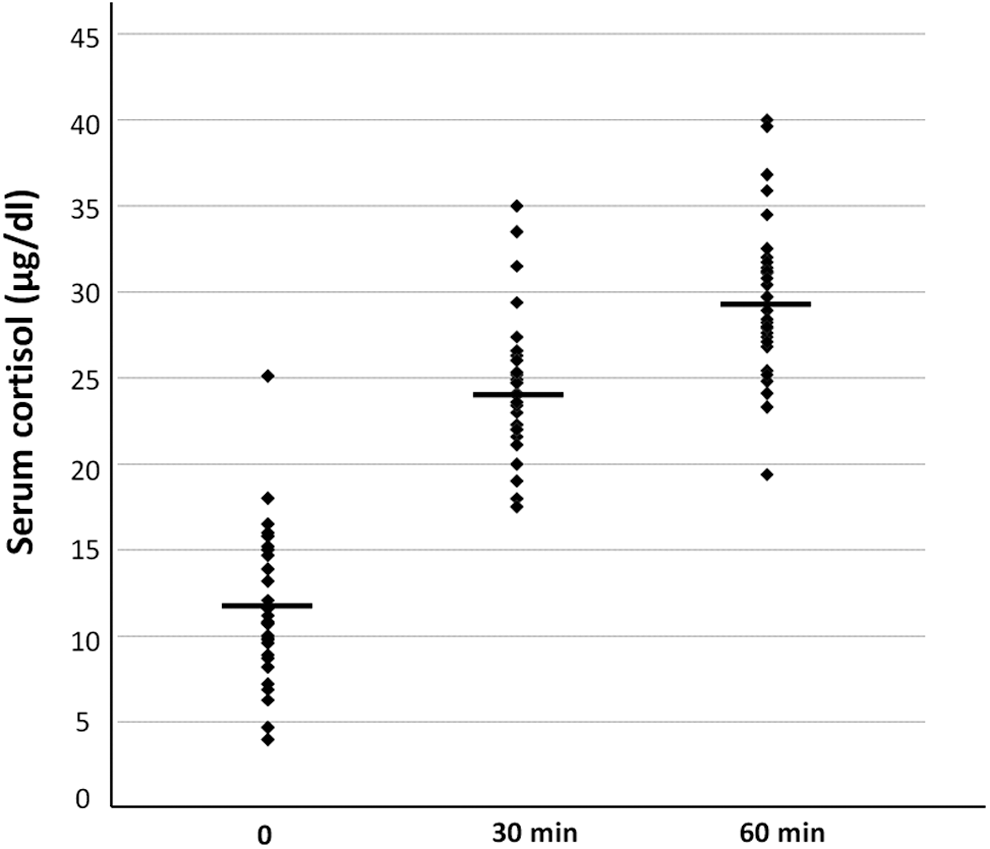
Cortisol responses following the ACTH stimulation test. Bullets represent individual cortisol levels, and cross lines the mean values.
Discussion
Several randomized trials have demonstrated the advantages, in terms of both effectiveness and safety, of i.v. over oral glucocorticoid administration for GO. Adverse events (mostly weight gain, hypertension, and Cushingoid features) are more frequent in patients treated with oral glucocorticoids compared to those treated with the i.v. regimen.
The effect of glucocorticoids on the HPA axis may vary between individuals. Therefore, it is difficult to predict the exact dose and duration of treatment that is required for significant adrenal suppression. However, patients who have been on prolonged oral daily treatment with high-dose glucocorticoids, particularly those with long half-lives such as dexamethasone, are at greater risk. Gradual glucocorticoid tapering is frequently advised in an attempt to reduce the risk of adrenal insufficiency and allow recovery of the HPA axis. Since there are no current evidence-based guidelines, many centers follow empiric tapering regimens.
As far as we know, there are no published data on the effect of the currently recommended i.v. glucocorticoid regimen for GO on adrenal function. Our findings clearly indicate that the treatment scheme proposed by the EUGOGO does not cause secondary adrenal failure.
One would have expected that with this supraphysiological dose of glucocorticoids and the duration of treatment, secondary adrenal insufficiency would have occurred. Our data suggest that periodic, weekly i.v. glucocorticoid administration allows recovery of the HPA axis, and adrenal suppression does not occur, in contrast to what happens when much lower cumulative doses are administered on a daily basis. In addition, the periodic administration appears not to be associated with withdrawal symptoms.
A possible limitation of our study might be the use of the standard-dose (250 μg) rather than the low-dose (1 μg) ACTH stimulation test in order to assess adrenal reserve. However, we opted for the standard dose, since a normal response to this test would exclude severe adrenal insufficiency (4), which is clinically more important.
In conclusion, the currently used i.v. glucocorticoid regimen for GO is safe regarding adrenal functional reserve.
Footnotes
Author Disclosure Statement
No competing financial interests exist.