
Abstract
Background:
At the onset of thyroid-associated orbitopathy (TAO), most patients are hyperthyroid, while scarce data are available on euthyroid/hypothyroid TAO. The aim of this study was to assess the prevalence, phenotype, and psychosocial burden of patients with initially euthyroid/hypothyroid TAO.
Methods:
The medical records of 461 consecutive and unselected patients with TAO followed at a specialized joint thyroid–eye clinic were analyzed within this retrospective cross-sectional study. Main outcome measures were the prevalence of initially eu- or hypothyroid TAO as well as ophthalmic signs and symptoms, disease-specific quality of life (QoL), work impairment, and rate of psychotherapy in initially eu-/hypothyroid versus hyperthyroid TAO.
Results:
The prevalences of eu-/hypothyroid and hyperthyroid TAO were 4.3% (n=20; [confidence interval, CI, 2.6–6.3]) and 95.7% (n=441; [9.37–9.74]), respectively. In 12 patients (2.6% [CI 1.3–4.3]), Hashimoto's thyroiditis was present and in 8 (1.7% [CI 0.7–3.0]) no thyroid disease was noted at the time of inclusion. One (0.05%) patient with eu-/hypothyroid TAO and 172 (39%) with hyperthyroid TAO had clinically active TAO (p=0.001). In eu-/hypothyroid versus hyperthyroid patients, 14 (70%) versus 135 (30.6%) had a mild TAO, 6 (30%) versus 183 (64.2%) a moderate-to-severe TAO, and 0 versus 23 (5.4%) had a sight-threatening TAO (p<0.001). TAO was asymmetric in 4 (20%) eu-/hypothyroid and in 27 (6.1%) hyperthyroid patients (p=0.038). Only 5.3% versus 30.2% and 10.5% versus 44.1% of patients with eu-/hypothyroid and hyperthyroid TAO, respectively, were on sick leave (p=0.003) or work disabled (p=0.018). QoL was less impaired in eu-/hypothyroid versus hyperthyroid TAO (median visual functioning and appearance scores: 100 versus 75; p<0.001 and 81.25 versus 75; p=0.315). Of patients with eu-/hypothyroid and hyperthyroid TAO, 15% and 20.2% had psychotherapy respectively (p=0.409). Eu-/hypothyroid TAO was positively (odds ratio 7.05, p=0.060) and negatively (odds ratio: 0.09, p=0.026) associated with a unilateral involvement and thyrotropin-receptor autoantibodies respectively.
Conclusions:
Compared with hyperthyroid TAO, QoL and working ability are less impaired in eu-/hypothyroid TAO with an often asymmetric and less severe clinical phenotype.
Introduction
T
The objective of this study was to provide actual data on prevalence and phenotype of initially euthyroid or hypothyroid TAO in a large collective of consecutive patients with TAO followed at a multidisciplinary center. Furthermore, the individual psychosocial burden (quality of life [QoL] and work impairment) in these subjects was evaluated for the first time in the literature.
Methods
Patients
The study protocol was consistent with the principles of the Declaration of Helsinki. Because this study was observational and did not include any interventions aside from those commonly falling within the daily routine, and because no decoded patient-related data were passed to third parties, no approval by the Ethics Committee was required. Written informed consent to be included in the database and to draw blood was obtained from all participants.
The medical records or files of 461 consecutive and unselected patients with TAO were analyzed within this retrospective cross-sectional study. All patients were followed for at least 12 months after the onset of TAO at the joint thyroid–eye clinic of the Johannes Gutenberg University (JGU) Medical Center, Mainz, Germany, between 2005 and 2012. Patients who were euthyroid or had overt or subclinical hypothyroidism before or within 6 months after the onset of TAO were compared with primarily hyperthyroid patients. To exclude other reasons for proptosis, orbital imaging (magnetic resonance or computed tomography) was performed in patients with euthyroidism or hypothyroidism.
The primary outcome measure was the prevalence of euthyroid or primarily hypothyroid TAO. Secondary outcome measures included the clinical phenotype of TAO, as well as QoL, work impairment, and the rate of psychotherapy in this subgroup of patients in comparison to initially hyperthyroid TAO patients.
Ophthalmic assessment
All patients were screened for signs of orbital involvement. TAO was classified as clinically active or inactive and as mild, moderate to severe, and sight threatening as recommended by the European Group on Graves' orbitopathy (21). TAO was considered unilateral if the proptosis difference between both eyes was larger than 4 mm, and/or if clinical signs and symptoms of TAO were found unilaterally.
Data on the following specific therapies was collected: bony orbital decompression, squint and eyelid surgery, retrobulbar irradiation, and steroid therapy. At our institution, intravenous steroids were usually administered during 12 consecutive weeks (cumulative dose 4.5 g) in clinically active, moderate-to-severe TAO (22,23), whereas in patients with sight-threatening TAO higher doses were given (24). Low dose orbital radiotherapy (with or without additional oral steroids) was performed during 10 weeks with single doses of one Gray per week (25,26) in patients with ocular motility disturbances and clinically active moderate-to-severe TAO.
Assessment of quality of life, work impairment, and need for psychotherapy
Quality of life was assessed with the disease-specific Graves' orbitopathy quality of life questionnaire (GO-QoL) as previously described (28 –32). Additionally, a comprehensive interview regarding work impairment and the need for psychotherapy was performed as previously reported (33).
Endocrine assessment and laboratory testing
Patients with subclinical, overt hypothyroidism prior to or within six months after the onset of TAO were considered as primarily hypothyroid. Euthyroid patients had normal thyroid-related parameters prior or within six months after the onset of TAO. Primarily hyperthyroid patients were selected as controls. GD was defined as hyperthyroidism with positive TRAb and a typical hypoechoic thyroid ultrasound pattern. HT was defined as the presence of at least five-fold increased serum levels of thyroid peroxidase and thyroglobulin autoantibodies (measured at least once), a typical ultrasound pattern, and eu- or hypothyroidism. Thyroid-related hormones (TSH, free T4 and T3) and autoantibodies (TSH receptor, thyroperoxidase, and thyroglobulin) were measured in all patients with commercially available immunoassays (Thermofisher, Henningsdorf, Germany).
Analysis
Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences, Version 21, Chicago, IL). A bootstrap analysis was used to calculate the 95% confidence intervals (CI) of the prevalences. Exact Fisher's test was used to calculate dependencies between two categorical variables. Mann-Whitney U test and Kruskal-Wallis test were used for associations between continuous and binary or categorical variables, respectively. To calculate the corresponding odds ratios (ORs), a univariable logistic regression analysis was used. The parameters which were significantly associated with eu-/hypothyroid TAO in these univariate analyses were put in a multivariable binary logistic regression model. Results with p<0.05 were considered statistically significant.
Results
The prevalence of primarily euthyroid or hypothyroid TAO was 4.3% (20 of 461 [CI 2.6–6.3]). In 12 patients (2.6% [CI 1.3–4.3]), HT was present and in 8 (1.7% [CI 0.7–3.0]) no thyroid disease was noted at the time of inclusion. The control group with primarily hyperthyroid TAO consisted of 441 (95.7% <CI 9.37–9.74]) subjects. Demographic data and endocrine parameters of these individuals are summarized in Table 1.
TAO, thyroid-associated orbitopathy; TSH, thyrotropin.
Ophthalmic assessment
Overall, 7 (35%) eu-/hypothyroid patients had undergone a clinically active phase of TAO requiring immunosuppressive therapy. At the time of inclusion in the study, TAO was clinically active (clinical activity score [CAS] ≥3) in one (5%) of 20 patients with initial eu- or hypothyroidism and in 172 (39%) of 441 with primarily hyperthyroid disease (p=0.001). Figure 1 illustrates the rates of mild, moderate-to-severe, and sight-threatening TAO in patients with euthyroidism or primarily hypothyroidism versus in those with hyperthyroid GD. A unilateral (or highly asymmetric) disease was documented in 4 (20%) patients with initial eu-/hypothyroidism and in 27 (6.1%) TAO patients with hyperthyroidism (p=0.038). Table 2 illustrates the various specific therapies administered in these patients. Of the 8 euthyroid patients, 4 (50%) had mild and 4 (50%) moderate TAO. Intravenous steroids had been given in 2 patients during the active phase of the disease. During follow up, none of these patients deteriorated and no orbital surgery or further treatment were required.
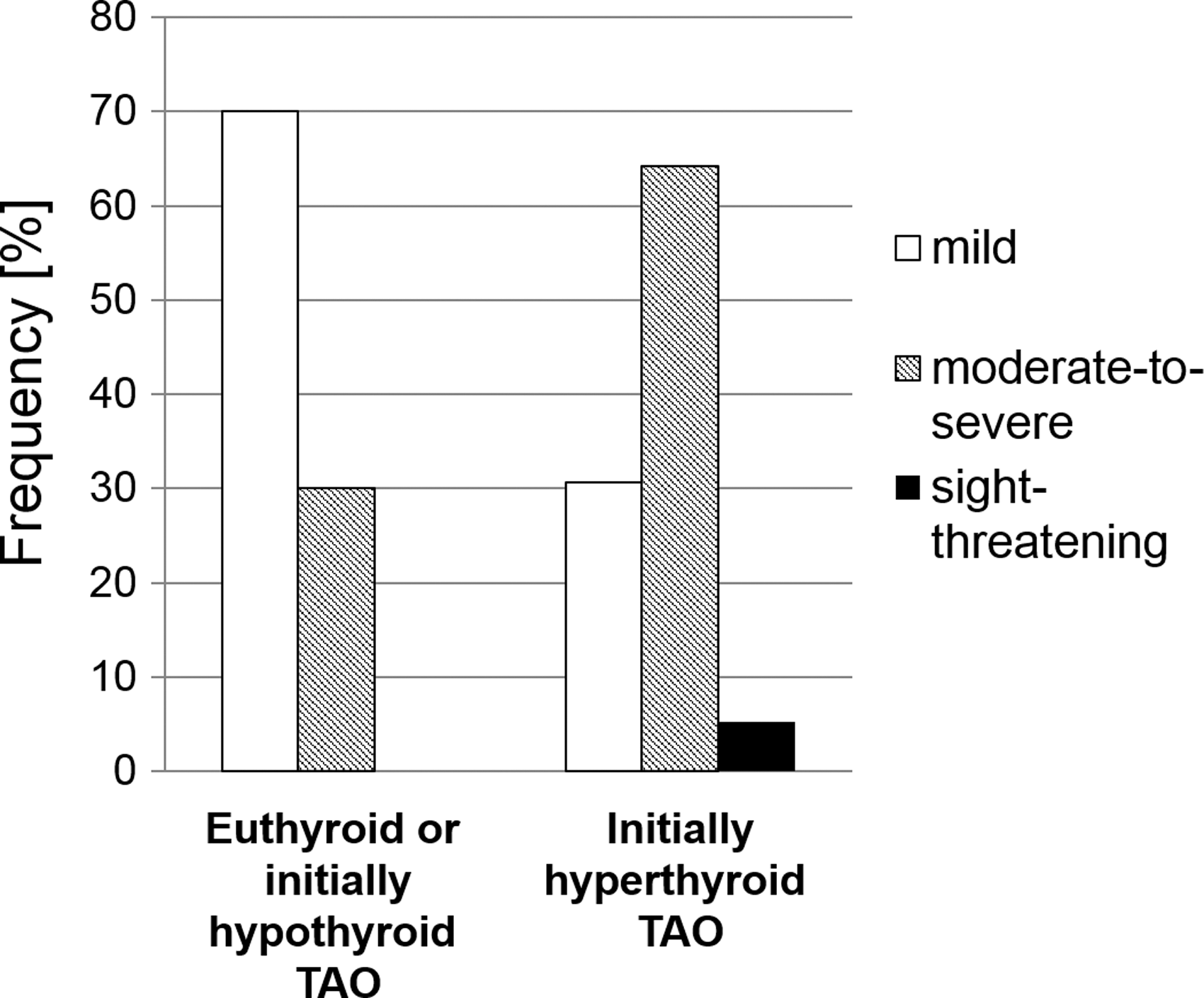
Association between clinical severity of thyroid-associated orbitopathy (TAO) and thyroid function. Of patients with euthyroid or primarily hypothyroid TAO (n=20), 14 (70%) had mild and 6 (30%) had moderate to severe TAO. No case of sight-threatening disease was noted in these patients. In contrast, of patients with initially hyperthyroid TAO (n=441), 23 (5.4%) had sight-threatening disease, 183 (64.2) had moderate to severe, and 135 (30.6%) had mild TAO (p<0.001).
Quality of life, need for psychotherapy, and work impairment
Nineteen (95%) and 407 (92.3%) patients with euthyroid/primarily hypothyroid and hyperthyroid TAO answered the GO-QoL. Both median visual functioning (VF) and appearance (AP) scores were 75 (range 0–100) in hyperthyroid TAO, and 100 (43.75–100; p<0.001) and 81.25 (25–100; p=0.315) in euthyroid or primarily hypothyroid TAO. Three (15%) of 20 and 88 (20.2%) of 436 (missing data in n=5) patients with euthyroid/primarily hypothyroid and hyperthyroid TAO had psychotherapy because of their TAO (p=0.409), respectively.
Of patients with euthyroid/primarily hypothyroid and with hyperthyroid TAO 19 of 20 (95%) and 329 (74.6%) of 441, respectively, were working in employment. Two (10%) patients with (initially) eu-/hypothyroid TAO and 145 (44.1%) patients with hyperthyroid TAO were on sick leave due to TAO (p=0.003). Work disability was documented in 1 (5%) and in 102 (30.2%) of patients with eu-/hypothyroid and with initially hyperthyroid TAO respectively (p=0.018).
Logistic regression analysis
The detailed results of the univariate analysis are shown in Table 3. A positive association (OR 3.83, p=0.024) was found between unilateral TAO and initially eu-/hypothyroid TAO. The odds of having active TAO, of having a more severe manifestation of TAO, and of having received intravenous steroids was 82%, 19%, and 30% lower in eu-/hypothyroid TAO than in initially hyperthyroid TAO (p=0.015, p=0.001, and p=0.012, respectively). Higher levels of TRAb were also negatively associated with eu-/hypothyroid TAO. Furthermore, initially eu- or hypothyroid TAO was negatively associated with age at onset of thyroid disease (OR 0.96, p=0.043). The odds of being on sick leave and work disabled was 15% and 13% lower in eu-/hypothyroid versus in hyperthyroid TAO (p=0.012, p=0.047) respectively. As a sign for being less impaired in daily activities, the odds of higher GO-QoL VF scores was 5% higher in patients with eu-/hypothyroid than in hyperthyroid TAO (p=0.002). All parameters that were significantly associated with eu-/hypothyroid TAO were included into the multivariate analysis (Table 4). Unilateral TAO was positively associated with eu-/hypothyroid TAO (OR 7.05, p=0.060), whereas a negative association between TRAb and eu-/hypothyroid TAO was found (OR 0.09, p=0.026).
Univariate binary logistic regression analyses.
Results with p<0.05 and 95% confidence intervals not including one are shown in bold.
GO-QoL, Graves' orbitopathy quality of life questionnaire.
All parameters that were significantly associated with hypo-/euthyroid TAO in the univariate analyses (Table 3) were included in a binary logistic regression model.
Significant results are shown in bold.
Discussion
To the best of our knowledge, this study is the first to report on the rates of sick leave, work disability, and the need for psychotherapy in a subgroup of patients with euthyroid or hypothyroid TAO. Furthermore, this study extends the knowledge regarding phenotype and course of orbital disease in initially eu- or hypothyroid TAO. In these patients the clinical phenotype of TAO is significantly less severe, the manifestation is more often unilateral, and QoL and working ability are less impaired than in patients with initially hyperthyroid TAO.
In patients with eu-/hypothyroid TAO other orbital diseases—for example, IgG4-related ophthalmic disease (IgG4-RD), an emerging GD-like disorder—have to be considered in the differential diagnosis (34). IgG4-RD is a new entity characterized by lymphoplasmacytic infiltration and tissue fibrosis causing organ dysfunction. It typically affects the lacrimal glands, orbits, salivary glands, lungs, pancreas, biliary ducts, and retroperitoneal tissue. Recently, a novel subtype of HT with an increased level of IgG4-bearing plasmocytes in the thyroid was proposed, thus suggesting a common mechanism in HT and IgG4-RD. As the eu-/hypothyroid TAO patients were TRAb-negative in the present study, besides orbital magnetic resonance imaging–sensitive laboratory assays (i.e. cell-based bioassays), may, as previously shown (35 –38), significantly improve diagnostics of TAO.
In a large collective of consecutive and unselected TAO patients seen at our university-based multidisciplinary orbital center, the prevalence of euthyroid and initially hypothyroid TAO was 4.3%. This is in line with a recent study reporting a prevalence of euthyroid and initially hypothyroid TAO of 4.2% (6). Nevertheless, both studies might have overestimated the “true” prevalence as they were performed at specialized referral orbital centers. Therefore, the prevalence of thyroid diseases and their extrathyroidal manifestations should be assessed in population-based studies. Another limitation is that the overall number of patients with eu-/hypothyroid TAO, which is explained by the low prevalence, was relatively small and hence the power of the study is low. This again emphasizes the need for meta-analyses and larger (population-based) studies pertaining to this matter. In the single population-based study assessing prevalence and incidence-rates of TAO, the majority of TAO patients (87%) had hyperthyroidism, whereas 7% were euthyroid and 6% were hypothyroid. In most hyperthyroid patients, thyroid dysfunction had developed prior or simultaneously with TAO. TAO was symmetric with no side difference in approximately half of the patients, whereas the other half had some degree of asymmetry, with 5% presenting entirely unilateral disease. In comparison, in our study, a higher frequency of a unilateral manifestation of TAO was noted in patients with eu-/hypothyroid TAO, and in the multivariate analysis, the odds of a unilateral manifestation of TAO was seven-fold higher in eu-/hypothyroid than in initially hyperthyroid TAO. Even though the definition of unilateral TAO was more stringent in the present study, this is in line with another recent report (6), which documented a side difference of three millimeters or more in 23% of patients with eu-/hypothyroid TAO versus in 4.8% of patients who were hyperthyroid. Moreover, the phenotype of TAO was milder, showed less inflammation, and was more frequently unilateral in patients with euthyroid or primarily hypothyroid TAO. Two-thirds of these patients had mild TAO and no case of sight-threatening disease was observed. In contrast, the majority of patients with initially hyperthyroid TAO had moderate-to-severe disease and more than 5% had optic neuropathy. Consequently, these patients more often needed immunosuppression and surgery to treat their TAO. On the other hand, there were also patients with eu-/hypothyroid TAO who required intravenous steroids to avoid progression to more severe forms. Regarding orbital decompression, decision for surgery frequently relied on personal preference, QoL, and/or patients' individual burden.
Quality of life and work impairment
In our study, patients with initially hyperthyroid TAO were four and five times more frequently on sick leave and work disabled than patients with primarily euthyroid /hypothyroid TAO. It has been shown previously that impaired working capacity is attributed to functional limitations such as diplopia and/or impaired visual acuity in patients with TAO (33). Therefore, it can be assumed that patients with eu-/hypothyroid TAO were less severely impaired in their earning capacity as they were less frequently affected by active and/or severe TAO. In line with this, patients with initially euthyroid /hypothyroid TAO reported a better quality of life (i.e., the functional aspects of the disease. Overall, they scored significantly higher on the VF score, since the vast majority had mild and inactive TAO. Indeed, diplopia and a sight-threatening disease are primarily associated with functional impairment as measured by this score (27,44,45). In contrast, there were no significant differences between the AP scores of patients with euthyroid or hypothyroid TAO versus those with initially hyperthyroid TAO. In conclusion, novel clinical and psychosocial data are presented for the first time in patients with eu-/hypothyroid TAO.
Footnotes
Acknowledgments
Katharina A. Ponto is funded by the Federal Ministry of Education and Research (BMBF 01EO1003). The authors are most grateful to Elisa Kolbe (study nurse) and Michael Kanitz (lab technician), Thyroid Research Lab, JGU Medical Center, for data collection.
Author Disclosure Statement
No competing financial interests exist.