
Abstract
Background:
The BRAFV600E mutation is a promising prognostic biomarker for patients with papillary thyroid carcinoma (PTC), but its prevalence differs widely among different geographic regions. A recent study reported that loss of the Cleavage and Polyadenylation Specificity Factor Subunit 2 (CPSF2) gene was associated with increased cellular invasion, cancer stem cells, and aggressiveness of PTC. This study aimed at evaluating CPSF2 protein expression as a prognostic marker for PTC in a region with a high prevalence of the BRAFV600E mutation, Korea.
Methods:
This study included 159 patients with classical PTC who underwent a total thyroidectomy and received ablative doses of 131I. The expression of CPSF2 protein was evaluated by immunohistochemistry and graded semi-quantitatively. The presence of the BRAFV600E mutation was evaluated by direct sequencing.
Results:
Negative protein expression of CPSF2 was observed in 34 (21.3%) of the 159 PTCs. In multivariate analysis, negative CPSF2 expression was significantly associated with cervical lymph node metastasis (odds ratio [OR]=2.56, p=0.28), and distant metastasis (OR=3.48, p=0.02). After adjusting for age, sex, tumor size, extrathyroidal invasion, lymphovascular invasion, and the BRAFV600E mutation, the CPSF2-negative group had a significantly lower recurrence-free survival compared to the CPSF2-positive group (hazard ratio=2.14, p=0.03).
Conclusion:
Negative protein expression of CPSF2 is independently associated with a poor clinical outcome in PTC. CPSF2 could be a useful prognostic marker for PTC in regions with a high prevalence of the BRAFV600E mutation.
Introduction
M
Cleavage and Polyadenylation Specificity Factor Subunit 2 (CPSF2) is the 100 kDa subunit of CPSF, which is involved in cleavage of the 3′ signaling region from a newly synthesized pre-messenger RNA (pre-mRNA) molecule during the process of gene transcription. The exact function of CPSF2 is still unknown, while its presence is essential for the pre-mRNA maturation process (15 –17). On the basis of genome-wide expression analysis, a recent study identified that the loss of CPSF2 gene expression is related to PTC-associated mortality in PTC samples (18). Another study reported that CPSF2 knockdown increases cellular invasion and expression of the thyroid cancer stem-like markers CD44 and CD133, and that the loss of CPSF2 gene expression is also associated with more advanced PTC (17).
This study evaluated the protein expression of CPSF2 using immunohistochemistry (IHC), and analyzed whether the expression of CPSF2 could be a useful indicator for predicting PTC metastasis and recurrence, especially in regions with a high prevalence of the BRAFV600E mutation.
Materials and Methods
Patients
The study included a total of 160 patients with classical PTC who underwent a total thyroidectomy between 2004 and 2005 according to the protocol established by the Endocrinology Division at the Asan Medical Center (Seoul, Korea) as previously described (12). The clinicopathological features of PTC were reviewed from the database after approval from the Institutional Research Board at the Asan Medical Center. Pathological staging was performed according to the Tumor, Lymph Node, Metastasis (TNM) classification system of the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC).
Tissue samples and construction of tissue microarray blocks
Histopathology and immunohistology of thyroid cancer specimens were reviewed by two experienced pathologists (Y.P. and D.E.S.). During the evaluation of the results of the immunohistochemical studies, a few discrepant cases were reviewed jointly for consensus by Y.P. and D.E.S. The specimens were fixed in formalin, and processed by the usual technique with paraffin embedding and hematoxylin and eosin staining. Formalin-fixed, paraffin-embedded tissue samples were arrayed using a tissue-arraying instrument (MTAII; Beecher Instruments, Silver Spring, MD). Briefly, the designated zone on each donor block was punched with a tissue cylinder (2.0 mm in diameter), and the sample was transferred to a recipient block. Two core samples were retrieved from each donor block.
DNA isolation and evaluation of the BRAFV600E mutation
DNA was extracted from paraffin-embedded tissue samples, and the presence of the BRAFV600E mutation was evaluated by polymerase chain reaction (PCR) amplification and direct sequencing as previously reported (12). Each DNA sample was analyzed at least twice to confirm the status of the BRAFV600E mutation. BRAFV600E mutation analysis was completed in 158 of the 160 PTC samples.
Immunohistochemical analysis and definition of CPSF2 protein expression
The degree of CPSF2 protein expression was evaluated by IHC with a rabbit polyclonal anti-CPSF2 antibody (1:25 dilution; Abcam, Cambridge, MA). Immunohistochemical staining was performed on 4-μm-thick TMA sections, using a BenchMark XT automatic immunostaining device (Ventana Medical Systems, Tucson, AZ) with the OptiView DAB IHC Detection Kit (Ventana Medical Systems) according to the manufacturer's instructions. IHC for CPSF2 was completed in 159 of 160 PTC samples. One sample of PTC was excluded from the analysis due to loss of the tissue cores. Nuclear staining intensity was graded semi-quantitatively by experienced pathologists as follows: 0, negative; 1+, weak; 2+, moderate; 3+, strong (Supplementary Fig. S1; Supplementary Data are available online at
Follow-up protocol
Patients were treated according to the treatment and follow-up strategy, which has been previously described (19). “Recurrence” was defined as the appearance of pathologically proven malignant tissue and/or the appearance of metastatic lesions. “Loco-regional recurrence” was defined as a recurrence in the neck lymph nodes (LN) or the operative bed, and “distant recurrence” was defined as a recurrence in the lungs, bones, and/or brain during the follow-up period.
Statistics
All statistical analyses were conducted by using R (v3.10) and R libraries survival (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline clinicopathological characteristics of study subjects
The mean age of the study participants was 47.4 years old (Table 1). Of 159 patients, 130 were female (81.7%) and 29 were male (19.3%). The mean tumor size was 2.6 cm. Cervical LN metastasis was found at the time of diagnosis in 68 patients (42.8%).
The percentages of subject numbers are presented in parentheses.
CPSF2, cleavage and polyadenylation specific factor 2; LN, lymph node.
Distant metastasis was found in five patients (3.1%) at the time of the initial diagnosis. Among the 154 patients without a distant metastasis at initial diagnosis, 23 patients had locoregional recurrence, and 13 patients had a distant recurrence during the median 8.3 years follow-up after diagnosis.
The presence of the BRAFV600E mutation was found in 112 (71.3%) of 157 patients who completed the mutational analysis.
Association between CPSF2 expression and clinicopathological parameters in PTC
The intensity scores of protein expression of CPSF2 were as follows: 0, 3 (1.8%); 1+, 31 (19.5%); 2+, 118 (74.2%); and 3+, 7 (4.4%) of the specimens. Since 0 and 1+ were considered to indicate negative expression in this study, 34 PTCs (21.4%) were grouped as the CPSF2-negative group, and 125 (78.6%) grouped as the CPSF2-positive group (Table 1). There were more male patients in the CPSF2-negative group (32.4%) compared with the CPSF2-positive group (14.4%, p=0.024). The incidence of cervical LN metastasis (58.8%, p=0.050) and distant metastasis (23.5%, p=0.027) was significantly higher in the CPSF2-negative group than in the CPSF2-positive group. The BRAFV600E mutation was present in 112 patients (71.3%). The mutation was significantly associated with CPSF2 positivity (p=0.032), being present in 93 (75.6%) patients in the CPSF2-positive group versus 19 (55.9%) in the CPSF2-negative group. There was no significant difference in age, tumor size, extrathyroidal invasion, or lymphovascular invasion between the two groups.
Negative CPSF2 expression and cervical LN metastasis of PTCs
To identify the prognostic factors associated with cervical LN metastasis, univariate and multivariate analyses were performed using a logistic regression model (Table 2). A tumor size (≥4.0 cm) and CPSF2 negativity were significantly associated with cervical LN metastasis in univariate analysis. In multivariate analysis, the BRAFV600E mutation (OR=2.44; [CI 1.11–5.36]; p=0.026) and CPSF2 negativity (OR=2.56; [CI 1.11–5.94]; p=0.028) were significantly associated with cervical LN metastasis from PTC.
OR, odds ratio; CI, confidence interval; PTC, papillary thyroid carcinoma.
Negative CPSF2 expression and distant metastasis of PTC
The clinicopathological factors associated with distant metastasis (5 synchronous, 13 metachronous) were evaluated (Table 3). The statistical analysis was inapplicable to patients with cervical LN metastasis, because all patients with a distant metastasis had a cervical LN metastasis. A distant PTC metastasis was significantly associated with negative CPSF2 expression in both the univariate (OR=3.54; [CI 1.27–9.84]; p=0.015) and multivariate analyses (OR=3.48; [CI 1.25–9.67]; p=0.017).
Prediction of recurrent PTC by the CPSF2 expression status
The median follow-up period of the study subjects was 8.3 years after the initial diagnosis, and recurrences were detected in 36 of the 154 patients lacking a distant metastasis when initially diagnosed.
During the follow-up interval, there were significantly more recurrent PTCs in the CPSF2-negative group compared with the CPSF2-positive group (p=0.004; Fig. 1). In the unadjusted group, the hazard ratio for recurrence in CPSF2-negative PTC was 2.59 with reference to the CPSF2-positive PTC (p=0.006, Table 4, unadjusted). After adjusting for age, sex, tumor size, extrathyroidal invasion, and lymphovascular invasion, the CPSF2-negative group was still significantly associated with a higher recurrence rate compared with the CPSF2-positive group (Table 4, Models 1 and 2).
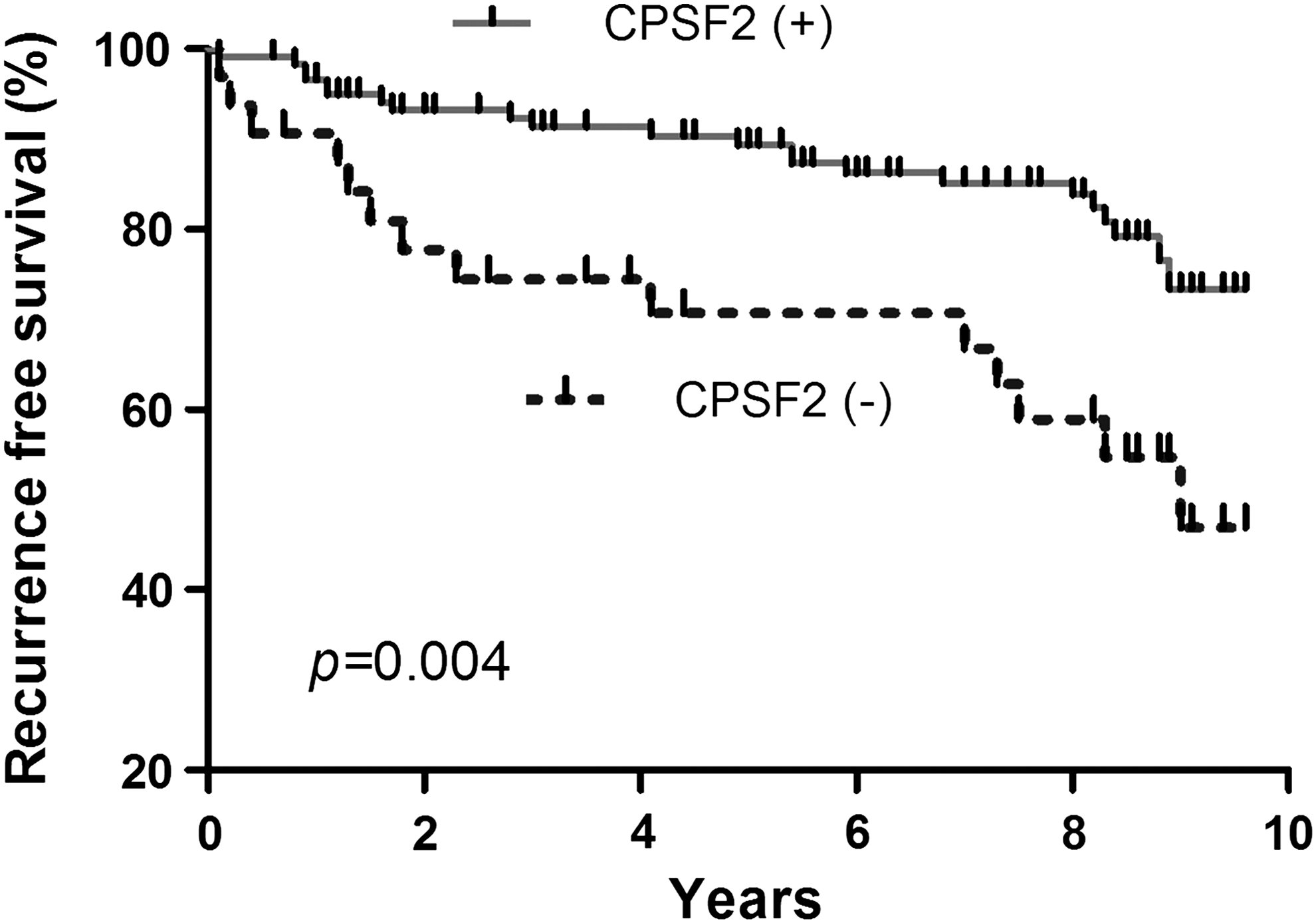
Recurrence-free survival according to the CPSF2 protein expression status. The Kaplan–Meier method was used to establish survival curves, and log-rank testing was used to compare recurrence-free survival between groups. CPSF2, cleavage and polyadenylation specific factor 2.
Model 1 is adjusted for age and sex. Model 2 is adjusted by Model 1, tumor size, extrathyroidal extension, and lymphovascular invasion. Model 3A is adjusted by Model 2 and the BRAF V600E mutation status. Model 3B is adjusted by Model 2 and cervical lymph node metastasis.
p-Values were calculated using a Cox proportional hazard model.
HR, hazard ratio.
In Model 3A (Table 4), which was adjusted for BRAFV600E mutation status in Model 2, the recurrence rate from PTCs was significantly higher in the CPSF2-negative group than in the CPSF2-positive group (HR=2.14, p=0.029). In Model 3B (Table 4), which was adjusted for cervical LN metastasis in Model 2, there were no statistically significant differences in recurrence-free survival between the CPSF2-positive and the CPSF2-negative groups (HR=1.59, p=0.247).
Discussion
This study evaluated the protein expression of CPSF2 by IHC and analyzed whether it could be a useful prognostic marker for PTC, especially in a region with a high prevalence of the BRAFV600E mutation such as Korea. The results suggest that patients with negative CPSF2 protein expression have a high frequency of cervical LN metastasis and distant metastasis regardless of the BRAFV600E mutation status. The CPSF2-negative group was also significantly associated with a higher recurrence rate and a lower disease-free survival compared to the CPSF2-positive group. After adjusting for age, sex, tumor size, extrathyroidal invasion, lymphovascular invasion, and BRAFV600E mutation status, the CPSF2-negative group was still significantly associated with a higher recurrence rate compared with the CPSF2-positive group.
CPSF2 is the 100 kDa subunit of CPSF, which consists of four polypeptides (160, 100, 73, and 30 kDa) (17,20). CPSF is a multi-subunit factor that recognizes the poly(A) signal sequence AAUAAA (21,22) and, as the name implies, is required for both cleavage and polyadenylation of mRNAs (21,23 –25). CPSF is involved in the cleavage of the 3′ signaling region from a newly synthesized pre-mRNA molecule in the process of gene transcription and plays a key role in nuclear export, translational initiation, and transcript stability (16,26). The exact function of CPSF2 is still unknown. However, its presence is essential for the pre-mRNA maturation process (15,16). Most mRNAs receive a polyadenylated tail post-transcriptionally, and this tail is added by two coupled reactions: endonucleolytic cleavage at the polyadenylate site followed by the polyadenylation of the upstream cleaved product (27). Alternative polyadenylation (APA) has been widely used to regulate gene expression. More than 50% of human genes have multiple polyadenylated sites and are the targets of APA. APA affects gene expression by producing different protein isoforms, or controlling the length of the 3′-UTR, which often harbors microRNA binding sites, thus altering the amount of protein generated by mRNA (17).
The results presented here suggest that PTC patients with negative CPSF2 protein expression had an independently higher frequency of cervical LN metastasis, distant metastasis, and tumor recurrence compared with patients with positive CPSF2 expression. A recent study using genome-wide expression analysis in PTC samples suggested that the loss of CPSF2 gene expression is correlated with PTC-associated mortality (18). Another study reported that CPSF2 knockdown increases cellular invasion and expression of thyroid cancer stem-like markers CD44 and CD 133, which could promote tumor recurrence and metastasis. Furthermore, the loss of CPSF2 gene expression is associated with more advanced PTC (17). There could be several possible mechanisms involved in decreased CPSF2 protein expression in aggressive PTC. Dysregulated microRNA targeting CPSF2 mRNA for suppression or epigenetic changes at the CPSF2 locus might alter the expression of CPSF2. Consistent with a previous report and the present findings, a decrease in tumor-suppressing functions in PTC with low CPSF2 expression may induce tumor invasion and transition to cancer stem-like cells (17).
In multivariate analysis, the presence of the BRAFV600E mutation and CPSF2 negativity were both significantly associated with cervical LN metastasis of PTC. On the other hand, the BRAFV600E mutation was significantly associated with CPSF2 positivity. Possible explanation for the apparent discrepancy of these results include that the cervical LN metastasis of PTC may have a stronger association with CPSF2 negativity than the presence of the BRAFV600E mutation in the studied subjects. Many studies have shown a high prevalence of the BRAFV600E mutation in Korean PTC patients ranging from 70% to 80% (12,14,28,29). Therefore, the value of the BRAFV600E mutation as a molecular marker in Korean patients with PTC may not be of clinical use as a prognostic marker (9,14). Further studies are required to explore the potential interactions between the BRAFV600E mutation and CPSF2 negativity in PTC, and between CSPF2 negativity and cervical LN metastasis in BRAFV600E mutation-prevalent regions.
The present study has several limitations. First, only patients who underwent total thyroidectomy at the authors' institution were included, thus presenting only limited information that may not be readily generalized to the entire Korean population. Second, the median follow-up period of 8.3 years is a relatively short to detect distant metastasis and PTC recurrence. Third, the intensity of CPSF2 protein expression was graded semi-quantitatively. Despite these limitations, this study is the first to evaluate the relationship between the protein expression of CPSF2 and the prognosis for PTC.
In conclusion, negative CPSF2 protein expression is independently associated with a poor clinical outcome in PTC patients. Therefore, the expression of CPSF2 could be useful as a prognostic marker for PTC, particularly in regions with a high prevalence of the BRAFV600E mutation. The role and mechanism by which CPSF2 promotes thyroid cancer progression and distant metastasis should be explored in further studies.
Footnotes
Acknowledgments
This study was supported by a grant (No. 2014-598) from the Asan Institute for Life Sciences, Seoul, Korea.
Author Disclosure Statement
No competing financial interests exist.