
Abstract
Background:
Qualitative lipoprotein changes, such as an increase in fasting remnants, are reported in subclinical hypothyroidism (SCH). It was hypothesized that such changes are due to reduced hepatic lipase (HL) activity in SCH: HL is an enzyme regulated by thyroid hormones, and is involved in the degradation of triglyceride (TG)-rich remnants. This study aimed to quantify remnant-like lipoproteins (RLP), small dense LDL (sdLDL), and HL activity in women with SCH, and to assess these parameters after levothyroxine replacement therapy.
Methods:
This was an observational cross-sectional study with a subsequent longitudinal follow-up. Findings in women with thyrotropin levels >4.5 mIU/L (SH group) were compared with age- and body mass index (BMI)–matched euthyroid women (control group). In addition, a subgroup analysis was undertaken in SCH women who chose to receive levothyroxine treatment (0.9 μg/kg/day) for 6 months. RLP was quantified by measuring cholesterol (RLP-C) and triglycerides (RLP-TG) after immunoaffinity chromatography, and sdLDL by automated standardized methods; HL activity was measured in post-heparin plasma.
Results:
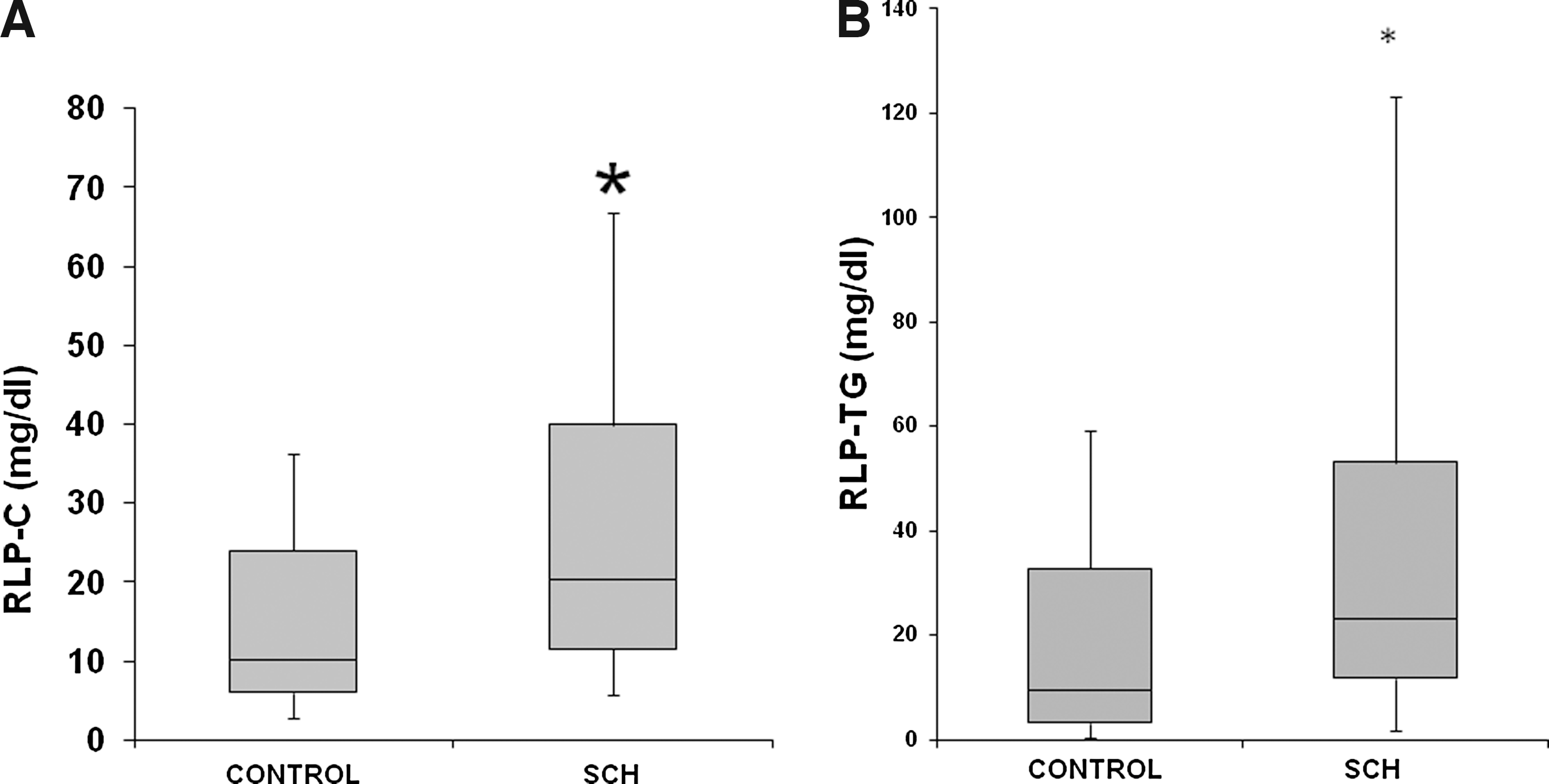
The SCH group included 37 women; 29 women were included in the control group. In addition, 22 women with SCH were included in the subgroup analysis (levothyroxine treatment). Significantly higher RLP values were observed in the SCH group than in the control group: RLP-C (median [range], mg/dL): 20.3 (5.8–66.8) versus 10.2 (2.7–36.3), p = 0.005; RLP-TG (mg/dL): 26.3 (3.2–123.3) versus 12.1 (2.5–61.6), p = 0.033. HL activity (mean ± standard deviation [SD], μmol free fatty acid/mL post-heparin plasma.h)—9.83 ± 4.25 versus 9.92 ± 5.20, p = 0.707—and sdLDL levels (mg/dL)—23.1 ± 10.7 versus 22.6 ± 8.4, p = 0.83—were similar. After levothyroxine, RLP-C decreased—21.5 (5.8–66.8) versus 17.2 (4.1–45.6), p = 0.023—and HL increased—9.75 ± 4.04 versus 11.86 ± 4.58, p = 0.012—in the subgroup of SCH women. No changes in sdLDL were observed.
Conclusions:
Women with SCH have higher RLP levels than matched controls do, but their RLP-C levels decrease significantly following levothyroxine therapy. Furthermore, HL activity also increases after levothyroxine therapy and can be interpreted as a possible explanation for the decrease in RLP-C.
Introduction
C
Women with SCH do not exhibit major alterations in their plasma lipid profile consistent with the degree of thyroid dysfunction. However, impaired lipoprotein metabolism—which is suggestive of qualitative lipid changes—might be responsible for the increased risk of coronary disease that is noted in these patients. Such qualitative changes include the increase of atherogenic particles without any alteration of the lipid profile in plasma (2). Although, low-density lipoprotein cholesterol (LDL-C) is the most established risk factor for atherosclerotic disease, residual risk still exists after LDL levels reach their target following treatment (3). A decrease in high-density lipoprotein cholesterol (HDL-C), an increase in non-HDL-C, and the presence of small dense LDL (sdLDL), remnant-like particles (RLP), and oxidized LDL may explain this residual risk. Furthermore, the assessment of lipoprotein metabolism in SCH has been poorly investigated.
Previously we demonstrated that hepatic lipase (HL) activity declines in SCH: our study population presented with high levels of triglyceride (TG)-enriched LDLs (4), which are potentially more atherogenic than typical LDL particles (2). Subsequent research using an electrophoretic qualitative method revealed the presence of intermediate or remnant lipoproteins in patients with SCH, in fasting conditions; this finding was also linked to decreased HL activity (5). In agreement with this earlier work, others also showed a reduction of TG-rich remnants in serum from patients with a deficit of thyroid hormones after three months of levothyroxine treatment (6,7). These studies predominantly involved Japanese cohorts of men and premenopausal women with various causes of hypothyroidism, and thyrotropin (TSH) was considered elevated with a cutoff value of 6 mIU/L. In another study (8), postprandial lipemia, which is also associated with an increased risk of cardiovascular disease, was also found in people with hypothyroidism.
Findings with regard to sdLDL are inconsistent. Increased levels of this LDL subfraction were reported in one study of people with SCH (9), but another observed a decrease in these particles (10). It is possible that these discrepancies were due to the methodology used for the detection of sdLDL and to factors closely related to the state of insulin sensitivity of the studied populations.
Data regarding the lipid–lipoprotein profile in SCH are controversial and limited. This can be explained by factors such as the difficulties apparent in setting an accepted cutoff value of TSH, the lack of statistical considerations that take into account confounding factors such as age (11), the degree of obesity (12) and insulin resistance (13) in participants, and the fact that the methodology used to evaluate modified lipoproteins is not readily available.
Finally, if lipoprotein alterations are due to SCH, replacement therapy with levothyroxine should also normalize lipoprotein levels, as demonstrated for remnant particles (6).
Since remnant lipoproteins might play a role in increasing the risk of cardiovascular disease in people with SCH, in the present study we aimed to quantify RLP and sdLDL by updated and validated specific methods in women with SCH, and to relate both atherogenic types of lipoproteins with HL activity and indicators of insulin resistance. Furthermore, the effects of levothyroxine replacement therapy for six months on these parameters in women with SCH were studied.
Materials and Methods
Patients
This was an observational cross-sectional study designed to evaluate the presence of lipid alterations in SCH where cases were compared to euthyroid controls. Subsequently, a cohort of those patients who agreed to be treated with levothyroxine was followed longitudinally to observe the effects of therapy on the lipid profile after reverting to an euthyroid state. The study was approved by the Local Ethical Committee, and an informed consent form was signed by all participants.
Adult women (aged ≥18 years) referred between 2010 and 2012 to the Endocrine Unit of Cesar Milstein Hospital, Buenos Aires, Argentina, because they exhibited high TSH levels were recruited to this study; the Endocrine Unit sought to rule out thyroid dysfunction. SCH was defined by a TSH level >4.5 mIU/L and a normal free thyroxine (fT4) level, using standard testing procedures. TSH and fT4 levels were checked twice during the study period, on inclusion and after 1 month, to confirm the SCH diagnosis. Women fulfilling this criterion formed the SCH group.
None of the women included in the study had previously received thyroid hormone replacement therapy or thyroid surgery. Other exclusion criteria included diabetes mellitus, acute critical illness, or use of hypolipemic drugs, estrogen replacement therapy, or drugs that may affect thyroid function (amiodarone, tyrosine kinase inhibitors, lithium, interferon-alpha, insulin sensitizers), or other factors that contraindicated levothyroxine use. Pregnancy and lactation and failure to sign the informed consent form were also considered as exclusion criteria.
The control group included women referred to the Endocrine Unit for symptoms such as asthenia, weight gain, or hair loss, in whom normal TSH and fT4 levels were demonstrated using the same standard methodology as used for the women with SCH. Women in the SCH and control groups were matched by age (range ±1 year), menopausal status (1 year with no menses constituted postmenopausal state), insulin sensitivity (measured by homeostasis model assessment for insulin resistance [HOMA-IR]), and body mass index (BMI; range ±1 kg/m2).
Those with SCH who agreed to participate in the subgroup analysis received levothyroxine treatment at 0.9 μg/kg/day. Biochemical analyses were performed before treatment commenced (SCHpre), then repeated after 6 months of levothyroxine therapy, at which point the endpoints were re-evaluated (SCHpost).
Samples
After 12-h overnight fasting, blood samples were taken. Serum was separated by centrifugation, and the samples were kept at 4°C for 24 h for the evaluation of lipid and lipoprotein profiles (using standard methods), or stored at −70°C for up to 1 year for further determination of TSH, fT4, insulin, RLP-C, RLP-TG, and sdLDL profiles. Glucose determinations were done immediately after blood extraction.
Heparin (60 IU/kg body weight) was administered intravenously for the determination of HL activity. Venous blood was taken 10 min later from the contralateral arm; samples were kept on ice. The post-heparin plasma sample (PHP) was obtained by centrifugation and kept at −70°C for processing within 30 days.
Measurements
Total cholesterol (Total-C), TG, and fasting glucose were measured using commercial enzymatic kits (Roche Diagnostics, Mannheim, Germany) using a COBAS® C-501 autoanalyzer, coefficient of variation (CV) intra-assay <1.9%, CV inter-assay <2.4%, averaging CV values of these parameters. HDL-C and total LDL-C were determined by standardized selective precipitation methods, CV intra-assay <2.0% and CV inter-assay <3.0%. Serum apolipoprotein (apo) A-I and apo-B 100 were determined by immunoturbidimetry (Roche Diagnostics), CV intra-assay <1.9% and inter-assay <2.5%, for the two parameters. Insulin was measured with Immulite®/Immulite® 1000 Insulin (Siemens, Munich, Germany). In order to estimate insulin resistance, the HOMA-IR was calculated as fasting insulin (mIU/mL) × fasting glucose (mmol/L)/22.5. The TG/HDL-C index was also used as a surrogate marker of insulin resistance.
fT4, TSH, antithyroglobulin, and antithyroid peroxidase were measured by chemiluminescence (DPC; Immulite, Los Angeles, CA); the normal range for fT4 was 0.8–1.9 ng/dL; intra- and inter-assay CV were 5.8% and 6.7%, respectively; the normal range for TSH was 0.3–4.5 mIU/L; intra- and inter-assay CV were 2.3% and 3%, respectively.
RLP were determined at Gunma University, Japan, using a method described by Nakajima et al. (14). Briefly, serum was mixed with RLP Immunoseparation Reagent (JIMRO-II; Japan Immunoresearch Laboratories, Takasaki, Japan) on an automated RLP mixer for 2 h at room temperature. After incubation, cholesterol and TG were measured in the unbound fraction (RLP fraction) by enzymatic methods. For RLP-C, the within-run and run-to-run imprecisions (CV) of the assay were ∼6% and 10%, respectively. The within-run imprecisions of RLP-TG with Determiner LTGII (n = 10) were CV = 5.0% (RLP-TG: 4.0 ± 0.9 mg/dL), CV = 2.8% (RLP-TG: 39.8 ± 1.1 mg/dL), and CV = 0.8% (RLP-TG: 101.2 ± 0.9 mg/dL), respectively. The ratio of RLP-TG/TG was calculated as an indicator of lipolytic activity.
In addition, sdLDL was measured using a standardized method on an automated analyzer (Hitachi 911; Hitachi, Tokyo, Japan), involving precipitation followed by centrifugation and the measurement of cholesterol concentrations. The kits used for these tests (LDL-C and sdLDL-C) were provided by Denka Seiken, Tokyo, Japan (15). Within- and between-run CVs for sdLDL-C were 4.99% and 4.67%, respectively.
Activity of HL in PHP was determined by measuring the oleic acid produced by the enzyme-catalyzed hydrolysis of an emulsion containing [3H]-triolein (Amersham TRA 191; Amersham, Buckinghamshire, United Kingdom) according to the Nilsson–Ehle method (modified) (16). Results were expressed as μmol of FFAs per mL of PHP per hour (16). Using triplicate analysis, the intra-assay CV was 4% and the interassay CV was 9%. Due to the complexity of this assay, the CV is considered quite satisfactory.
Statistical methods
Student's t-tests or Mann–Whitney U-tests were employed for analysis of normally distributed or nonparametric data, respectively. Pre- versus post-thyroxine replacement data were analyzed with a paired Student's t-test or Wilcoxon signed-rank sum test, accordingly. Correlations between variables were determined using Pearson's or Spearman's tests, depending on the distribution of the parameters. Differences were considered significant at p < 0.05. IBM SPSS Statistics for Windows v20 (IBM Corp., Armonk, NY) was used for statistical analyses.
Results
Demographics and baseline characteristics
Thirty-seven women with SCH (M age = 61 years; range 30–75 years) and 29 control group participants were included in the study. Demographic and clinical parameters are presented in Table 1. There were no significant differences between the SCH and control groups in terms of age (p = 0.521), weight (p = 0.625), BMI (p = 0.878), or waist circumference (p = 0.433). Both groups had similar postmenopausal status (SH 74%; controls 72%). As per the definition, women with SCH exhibited increased TSH levels (p = 0.001) compared with levels observed in controls, and fT4 levels were within normal limits. The main cause of SCH was interpreted as chronic autoimmune thyroiditis, since thyroid autoantibodies were positive in 60% of the SCH group.
Student's t-tests or Mann–Whitney U-tests were employed for analysis of normally distributed or nonparametric data, respectively. Pre- versus post-thyroxine replacement data were analyzed with paired Student's t-tests or Wilcoxon signed-rank sum tests, accordingly. Differences were considered significant at p < 0.05.
ApoA, apolipoprotein A; ApoB, apolipoprotein B; BMI, body mass index; FFA, free fatty acids; fT4, free thyroxine; HDL, high-density lipoprotein; HL, hepatic lipase; HOMA-IR, homeostasis model assessment for insulin resistance; LDL, low-density lipoprotein; PHP, post-heparin plasma; RLP, remnant-like lipoprotein particle; sdLDL, small dense low-density lipoprotein; TG, triglycerides; TSH, thyrotropin; NR, not reported.
Cross-sectional study
No differences were observed between groups regarding markers of lipids, lipoproteins profiles, and insulin resistance. However, women with SCH presented with lower apoAI values than controls (p = 0.049; Table 1).
RLP, sdLDL, and HL activity determinations
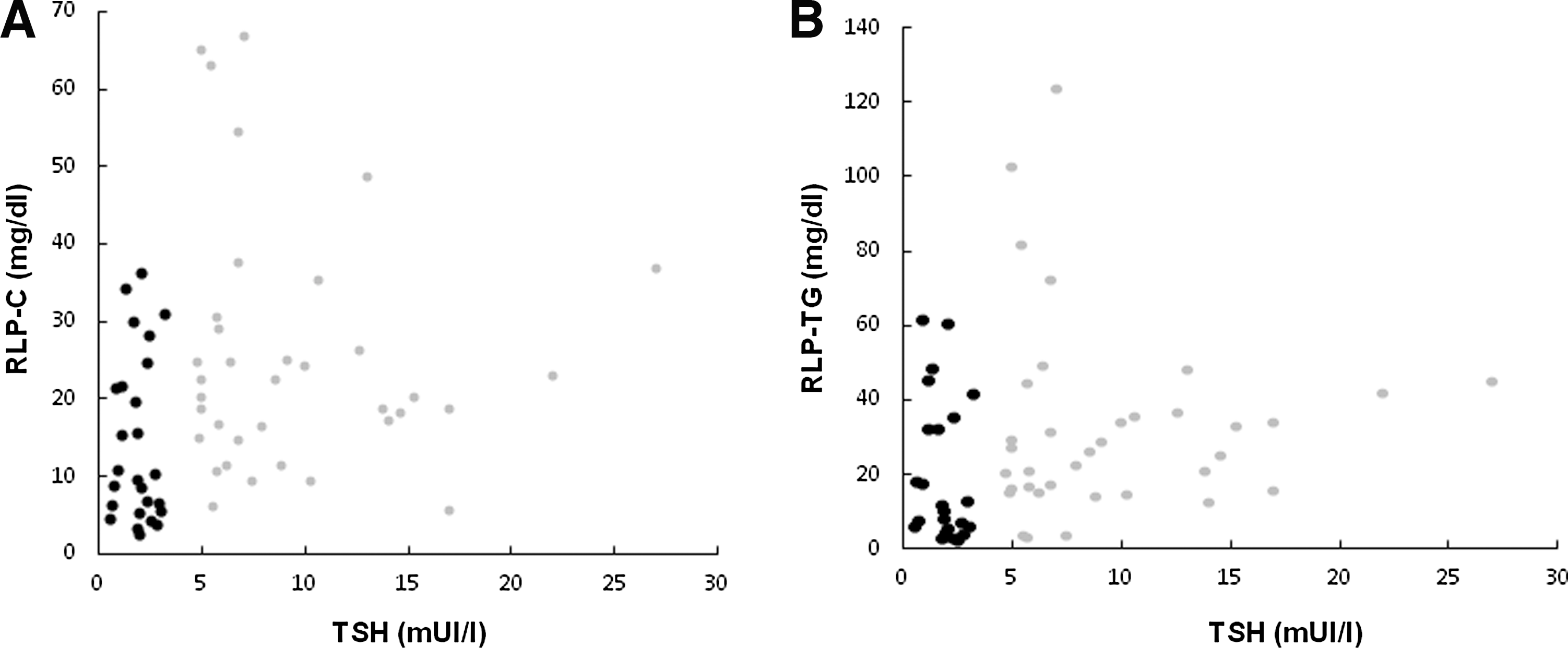
Women with SCH presented with higher values of RLP-C (p = 0.005) and RLP-TG (p = 0.033) than controls did (Fig. 1A and B, respectively). The Spearman correlation between TSH and RPL-C and RLP-TG in the control and SCH groups was r = 0.311, p = 0.014, and r = 0.265, p = 0.039, respectively (Fig. 2A and B). Moreover, the RLP-TG/TG ratio was increased in the SCH group (SCH: 0.23 [0.04–0.96] vs. control group 0.14 [0.04–0.43]; p = 0.05). Meanwhile, no differences were observed in sdLDL levels (SCH: 23.1 ± 10.7 vs. controls: 22.6 ± 8.4 mg/dL; p = 0.830) or in HL activity (SCH: 9.83 ± 4.25 vs. 9.92 ± 5.20 μmol FFA/mlPHP.h; p = 0.707; Table 1).
(
(
Longitudinal study
Of the original cohort of 37 women with SCH, 28 agreed to participate in the longitudinal study where levothyroxine was administered (SCHpre and SCHpost groups). However, five patients were lost to follow-up: one patient who experienced palpitations (considered related to levothyroxine treatment) and four who never returned for re-evaluation at 6 months. Another patient was withdrawn from the longitudinal study because she developed type 2 diabetes mellitus. Therefore, 22 patients were included in the longitudinal (subgroup) analysis. These patients received levothyroxine treatment for 6 months (final mean dose: 61 ± 17 μg/24 h; range 25–75 μg/24 h).
At the end of the treatment period, a decrease in TSH levels (p = 0.001) and an increase in T4 levels (p = 0.002) were observed (Table 1). The women with SCH had attained stable TSH values (range 0.3–4.5 mIU/L). In addition, following levothyroxine treatment, a decrease in HDL-C levels was observed (p = 0.04; Table 1).
RLP, sdLDL, and HL activity determinations
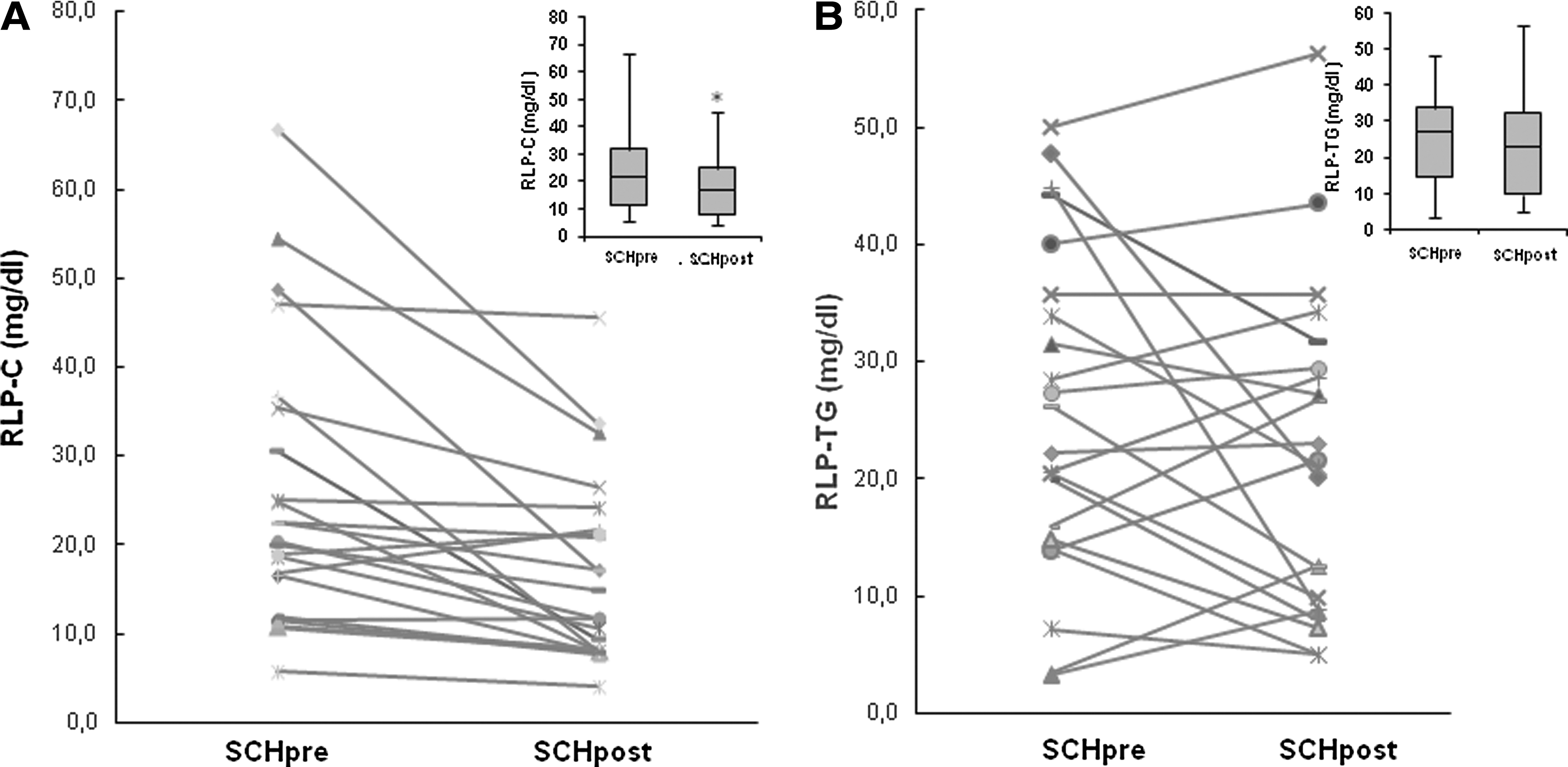
In reference to remnant lipoproteins, a decrease in RLP-C (p = 0.023) was found in the SCHpost data compared with SCHpre data, without significant changes in RLP-TG (p = 0.502; Fig. 3A and B, respectively). Again, no differences were observed in sdLDL levels (SCHpre: 25.1 ± 12.7 vs. SCHpost: 26.3 ± 12.3 mg/dL; p = 0.833).
(
Finally, as seen in Figure 4, women with SCH presented with an increase in HL activity after 6 months of levothyroxine treatment (p = 0.012). In addition, HL activity negatively correlated with RLP-C (r = –0.421, p = 0.009) and RLP-TG (r = –0.358, p = 0.030), though no differences were observed in the RLP-TG/TG ratio in women with SCH after levothyroxine treatment (SCHpre: 0.21 [0.04–0.36] vs. SCHpost 0.18 [0.07–0.47]; p = 0.455).
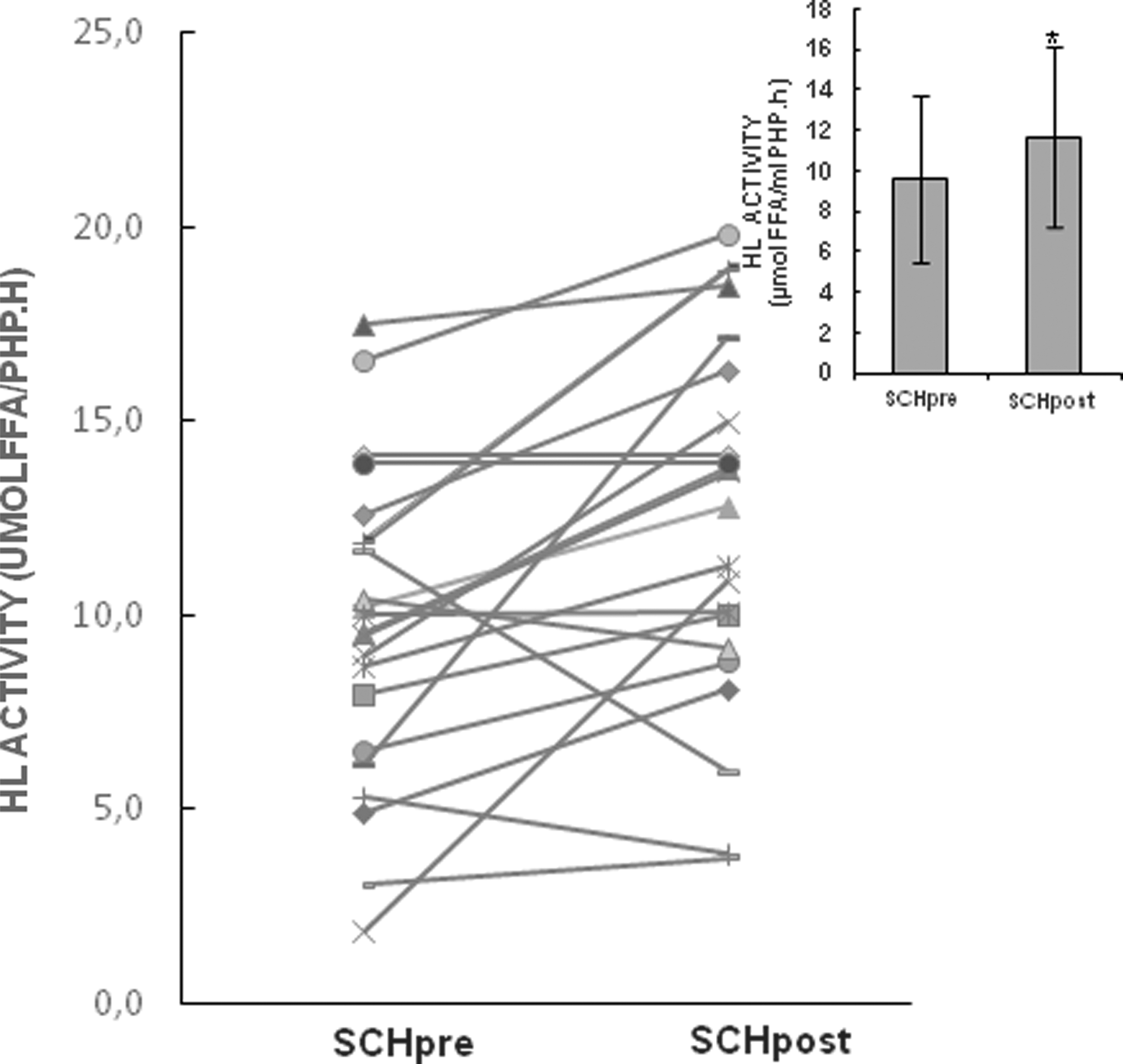
Hepatic lipase (HL) activity (μmolFFA/mlPHP.h; M ± SD for box plots and mean for individual data) in SCH patients before (SCHpre) and after 6 months of levothyroxine treatment (SCHpost) SCHpre (n = 22): 9.75 ± 4.04 versus SCHpost (n = 22): 11.86 ± 4.58 μmol FFA/mlPHP.h; p = 0.012, Student's t test.
Discussion
The findings of the present study show that women with SCH have increased levels of RLP compared with euthyroid women. Furthermore, RLP-C decreases following treatment with levothyroxine. HL activity also increases after levothyroxine treatment in women with SCH, and this rise could be interpreted as a possible explanation for the decrease in RLP-C.
These findings extend those of Ito et al. (7), who first described a decrease of RLP levels with levothyroxine therapy; the results herein show that the observations of Ito et al. also apply to SCH patients outside Japan. Moreover, the spectrum of patients has now broadened to include insulin-sensitive, postmenopausal women with TSH levels >4.5 mIU/L.
The RLP are components of highly modified TG-rich particles that result from the lipolysis of chylomicrons and very low density lipoprotein (VLDL) (17,18). These remnants have been described as being potentially atherogenic because they may induce both foam-cell formation and inflammation (2). Their plasma levels can be increased due to overproduction of VLDL, or due to delayed clearance of the remnants. The relevance of the lipoprotein remnant as a cardiovascular risk factor has been already confirmed in a study involving 560 patients with coronary artery disease who had LDL-C levels <100 mg/dL on lipid-lowering therapy (19). This study showed that RLP-C was superior to non-HDL-C for predicting cardiovascular events, suggesting that remnant lipoproteins may play an important role in residual risk for such events and should be checked in at-risk patients (19). However, the isolation of RLP by immunoseparation methods is usually only performed in highly skilled lipid laboratories and is not in widespread use. Interestingly, non-fasting TGs (a surrogate of remnant lipoproteins) appear to be an excellent marker for ischemic heart disease, which implies that the elevated cholesterol content of TG-rich lipoprotein particles is involved in the atherogenic process (3). Therefore, non-fasting TGs have been proposed as a new marker for cardiovascular risk.
While most epidemiological studies have reported heightened cardiovascular morbidity/mortality rates in patients with SCH, especially in those aged <65 years—and this has been acknowledged in recent guidelines (20,21)—several of these studies (22 –24) reported no differences in lipid profiles between SCH patients and the general population. Therefore, although the pathogenic implication of increased RLP found in SCH remains to be determined, the presence of these increased lipoproteins in the serum of patients with SCH may play a role in the excessive cardiovascular risk in such patients.
The increased levels of RLP found in patients with SCH in the present study might be explained on the one hand by overproduction of TG-rich particles by the liver, as described by Gjedde et al. (25). These investigators observed that in overt hypothyroid patients, despite increased TG levels, lipolysis appeared to be unmodified. The presence of insulin resistance could be further complicating the lipid profile through this pathway. However, this was not the case in the present population of relatively insulin-sensitive patients and controls. Other authors have also described that intravascular metabolism of TG-rich lipoproteins was normal in hypothyroidism (26).
On the other hand, the current findings of an increase in RLP could be also interpreted in light of a decreased clearance. Thyroid hormones are known to upregulate the expression of the LDL receptor, which is also responsible for remnant particle uptake (1). More recently, other mechanisms of lipid clearance have been reported in animal models. Autophagy of lipid droplets, which is a major pathway of lipid mobilization in hepatocytes, was induced by triiodothyronine in cultured liver cell lines (27). Furthermore hepatic LDL receptor-related protein 1 (LRP1), a major hepatic TG-rich lipoprotein clearance receptor, has also been found to be regulated by thyroid hormone in mice (28). Altogether, decreased hepatic LRP1 and lipophagy might be associated with reduced clearance of circulating RLP, thereby altering the serum lipid profile in hypothyroidism. Moreover, women with SCH presented with a heightened RLP-TG/TG ratio, which has been proposed as an indicator of delayed remnant lipoprotein metabolism (29). This concept is consistent with a decreased activity of HL, the enzyme involved in the degradation of TG-rich remnants. A description of the reduced activity of HL in overt hypothyroidism was provided by Valdemarsson et al. (30), and its decrease was previously described in patients with SCH, together with a negative correlation between a higher TG/C ratio of the isolated LDL particles (4). Although no differences were found in HL activity between the SCH and euthyroid groups in the present study, levothyroxine replacement therapy significantly increased HL activity. The recovery of HL activity and the inverse correlation found between HL activity and RLP-C and RLP-TG could be interpreted as another possible explanation for the accumulation of RLP in SCH. In any case, it will be necessary to deepen further the evaluation of HL activity in patients with SCH considering the whole hormonal status, since the enzyme is very sensitive to hormonal regulation, namely sex steroids and glucocorticoids, which may together with thyroid hormone induce variations in its activity (31).
A slight but significant increase in body weight occurred in patients with SCH following restoration of euthyroidism. Accordingly, a significant decrease of HDL-C was observed. Despite weight gain, RLP-C levels decreased with levothyroxine therapy in this time period, indicating that a specific metabolic pathway, namely increased HL activity, was being activated.
With regard to our findings of normal sdLDL-C levels in the SCH cohort, most of the reports on this topic agree that sdLDL levels are either reduced (10,32) or normal (33) in affected individuals. A decrease in HL activity might explain the normal sdLDL levels found in hypothyroidism, and it can be argued that this would compensate the atherogenic potential of increased RLP levels. However, the presence of higher levels of TG-rich particles in hypothyroid patients might also be related to larger LDL particles with an impaired conformation, which are not easily recognized by the LDL receptor (4).
The limitations of this study include the lack of a placebo arm, the inclusion of which would have enabled this study to be categorized as a randomized control trial. In addition, it is acknowledged that it would have been helpful to repeat the biochemical parameter testing in the women with SCH who did not receive six months of levothyroxine treatment. In any future study, the measurement of Lp(a) levels in participants should also be considered. Furthermore, although patients were advised to maintain their dietary habits during the treatment period, this was not easy to accomplish (probably due to the extended length of the treatment period). Another limiting aspect is that the study was exclusively undertaken in women, but due to the epidemiology of SCH, a decision was made to focus the analysis on females, who are more commonly affected.
With regards to the different results observed between RLP-TG and RLP-C following treatment, it must be taken into account that even when RLP are loaded with both (i.e., cholesterol and TG), RLP-C is a more stable parameter compared to RLP-TG. Remnant cholesterol correlates significantly with non-fasting triglyceride levels, which reflects the circulating remnants particles (34). Moreover, it is important to mention that RLP-C and RLP-TG are not always correlated (35,36). The reasons for this discrepancy are not known and await further investigation.
Conclusions
In conclusion, women with SCH have increased levels of RLP compared with euthyroid women, and RLP-C levels in particular decrease following treatment with levothyroxine. Furthermore, HL activity also increases after levothyroxine treatment, and this could be interpreted as one possible explanation for the decrease of RLP-C, in addition to hepatic overproduction of triglyceride-rich precursor particles and a decrease in the specific receptors. These findings highlight the atherogenic impact of impaired lipoprotein metabolism despite normal plasma lipid levels in SCH and contribute to improving our understanding of the pathophysiological mechanisms of lipid metabolism associated with mild hypothyroidism, while confirming the effectiveness of levothyroxine treatment.
Footnotes
Acknowledgments
Merck Serono kindly provided levothyroxine for the treatment of patients with SCH. We thank Fishawack Communications GmbH for providing editorial assistance. Part of this study was funded with a Grant from University of Buenos Aires, UBACyT, Argentina.
Author Disclosure Statement
We declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.