
Abstract
Background:
Thyroid nodules are prevalent and mostly benign, being present in up to 67% of the population when assessed by ultrasound. Due to the variable diagnostic performance of ultrasound-guided fine-needle aspiration biopsy (USFNA) of the thyroid and the possibility of a false-negative result, current clinical guidelines recommend ultrasonographic follow-up of benign thyroid nodules. The objective of this study was to evaluate the clinical relevance of a repeat fine-needle aspiration (rFNA) in patients with an initial benign fine-needle aspiration biopsy (iFNA).
Methods:
A retrospective review was conducted of medical records of patients seen at the Mayo Clinic between January of 2003 and December of 2013 who had undergone rFNA of a nodule with benign iFNA. The outcome measured was the result of the rFNA and histopathological correlation, when available.
Results:
Three hundred and thirty-four nodules with benign iFNA underwent rFNA during the 10-year study period. The rFNA was most commonly reported as benign (85.3%), followed by suspicious (7.2%), nondiagnostic (5.7%), and malignant (1.8%). The rFNA changed clinical management in 9.5% of the cases. The prevalence of thyroid malignancy ranged from 4.1% to 1.2% based on the gold standard used (histology vs. long-term follow-up, 4.0 ± 2.3 years).
Conclusion:
In the majority of patients with a benign iFNA, results of the rFNA were unchanged. However, in a small group of patients, the rFNA may differ from the initial results, and alter management. Even so, the prevalence of malignancy remains very low, ranging from 1.2% to 4.1% depending on the gold standard.
Introduction
T
The diagnostic accuracy of USFNA of the thyroid for differentiated thyroid cancer varies among institutions, with reported false negative rates (FNR) that range between 0.7% and 11% (4,5). This diagnostic variability raises the possibility of a missed diagnosis of thyroid cancer, driving the need for close ultrasonographic follow-up of BTN. Current guidelines recommend a repeat thyroid ultrasound 6–18 months after the initial fine-needle aspiration (iFNA), and repeat fine-needle aspiration biopsy (rFNA) if there is documented nodule growth (6).
The clinical value of this approach, however, is unclear. Studies have shown that initially suspicious ultrasound features might be a better predictor of malignancy and of false-negative (FN) results than growth during follow-up (7 –9). In addition, the possible adverse outcomes of BTN during follow-up, such as death from undiagnosed thyroid cancer and need for thyroidectomy, have been scarcely investigated. A study of 2010 cytological benign nodules followed for an average of 8.5 years found no cases of death due to thyroid cancer, a FNR of 1.3%, and a need for thyroidectomy in 24% of the patients, with the most common indication being the presence of a large nodule and/or compressive symptoms in 60% of cases (10). Another study compared the rates of a new diagnosis of malignancy or need for thyroidectomy between patients with long-term versus short-term follow-up and found no significant difference in these outcomes (11). A recent prospective study that followed patients with BTN (based on ultrasound features or histology) found that in 15% of the patients the nodules demonstrated growth, while thyroid cancer was diagnosed during follow-up in only 0.3% of these nodules (12).
The main objective of the present study was to determine the clinical value of rFNA in patients with iFNA who underwent rFNA with regards to changes in clinical management and, more importantly, new diagnosis of thyroid cancer.
Methods
An electronic search was conducted of the cytology reports of all USFNA of the thyroid done at the Mayo Clinic between January 2003 and December 2013. During this period, 15,185 thyroid FNAs were completed. A total of 2540 rFNA (not necessarily of the same nodule) were performed in 1205 individual patients during the study period. Within this group, there were 334 nodules with a benign iFNA that underwent rFNA of the same nodule involving 323 patients. This cohort included patients with nodules with a benign iFNA, after excluding those cases in which the rFNA was obtained from a different nodule or in whom there was a previous history of thyroid cancer.
Clinical features are reported in percentages in cases of categorical variables and as means ± standard deviation (SD) for continuous variables. Growth during follow-up was indicated as the reason for rFNA if this was documented by the clinician or radiologist. The pathology results were correlated with the ultrasound features of the nodules to determine whether the findings of rFNA or histology corresponded to the index nodule. For example, a finding of an incidental papillary thyroid cancer in an area that did not correspond to the index nodule was not included in the analysis as a new diagnosis of thyroid cancer. In addition, in all discordant cases, a pathologist (T.J.S.), experienced in both cytopathology and surgical pathology of the thyroid, reviewed the cytology and surgical pathology slides to verify the preoperative and surgical diagnoses, including, in the latter, the presence of histologic evidence of preoperative needle tract effect characterized by fibrin clot pooling, fibro-inflammatory and histiocytic reaction, and architectural disruption of the interface between the lesion that underwent FNA and the background thyroid tissue.
The proportion of thyroid malignancy was estimated using two gold standards. First, the proportion of thyroid malignancy among all patients in the cohort was calculated; all the cases were taken into account if no malignancy diagnosis was made during follow-up (mean follow-up time of 4.0 ± 2.3 years). This proportion was also calculated among only those patients who underwent surgery (final histopathology) for any indication.
Results
A total of 334 nodules with benign iFNA in 323 patients underwent rFNAB during the 10-year study period. The mean age at the time of first biopsy was 52.3 ± 15.4 years, and 81% of the patients were women. The mean follow-up time was 4.0 ± 2.3 years (range 0.1–10.2 years). The results of the rFNA are shown in Figure 1.

Flow diagram of included patients.
The majority of patients (86 %) had no previous history of thyroid disease; Hashimoto's thyroiditis was present in 7.5%, Graves' disease in 1.8%, and other thyroid diseases in 5.1% of the patients (e.g., history of thyroid nodules). Repeat thyroid ultrasound was not performed in only two patients during follow-up.
Nodule size was available for 313 nodules, and mean size was 2.3 ± 1.3 cm. In addition, 13% of the nodules were >4 cm, and at least one suspicious ultrasound feature (hypo-echogenicity, irregular margins, microcalcifications, increased vascularity) was present in 28.4%.
Only 1% of patients complained of rapid growth at baseline or during follow-up, and most patients (93%) had serum thyrotropin (TSH) levels between 0.3 and 5.5 mIU/mL. However, 13 (4.2%) had TSH levels <0.3 mIU/mL, and seven (2.3%) had levels >5.5 IU/mL. Serum TSH levels were not available in 28 patients.
The mean time to rFNA was 3.1 ± 2.0 years. The indications for rFNA and total or partial thyroidectomy are listed in Table 1. A description of the clinical variables based on rFNA category is listed in Table 2.
rFNA, repeat fine-needle aspiration.
US, ultrasound; RCC, renal cell carcinoma.
In 49 (14.7%) patients, the rFNA changed; 29 of these patients underwent surgery, and three others were diagnosed with nonthyroid malignancies, representing 9.5% of the cases in which the rFNA changed clinical management, as shown in Figure 2. In the rest of the patients, further follow-up was continued (15 nondiagnostic cases on rFNA). Three of the patients with malignant results on rFNA biopsy underwent surgery, with histological confirmation of one case of anaplastic thyroid cancer, one case of papillary thyroid cancer, and one case of follicular thyroid cancer. Four of the nondiagnostic cases on rFNA underwent surgery, and all four cases were benign. Among the patients in whom cytology changed, there were 24 patients with “suspicious” cytology on rFNA. In 17 of these, the rFNA was read as “suspicious for neoplasm” (follicular or Hürthle cell), and in five others “suspicious for papillary thyroid cancer.” Sixteen of the 17 patients with “suspicious for neoplasm” cytology underwent surgery, and all but one (94%) had a benign histopathology, while the other one had a nonthyroid (metastatic renal cell carcinoma) malignancy. All five patients with rFNA cytology “suspicious for papillary thyroid cancer” underwent surgery, and papillary carcinoma was confirmed in one case. There was a case in which the rFNA was reported as suspicious for renal cell carcinoma, which was confirmed on histology. A detailed description of the histopathological correlation is found in Table 3 and Figure 1.
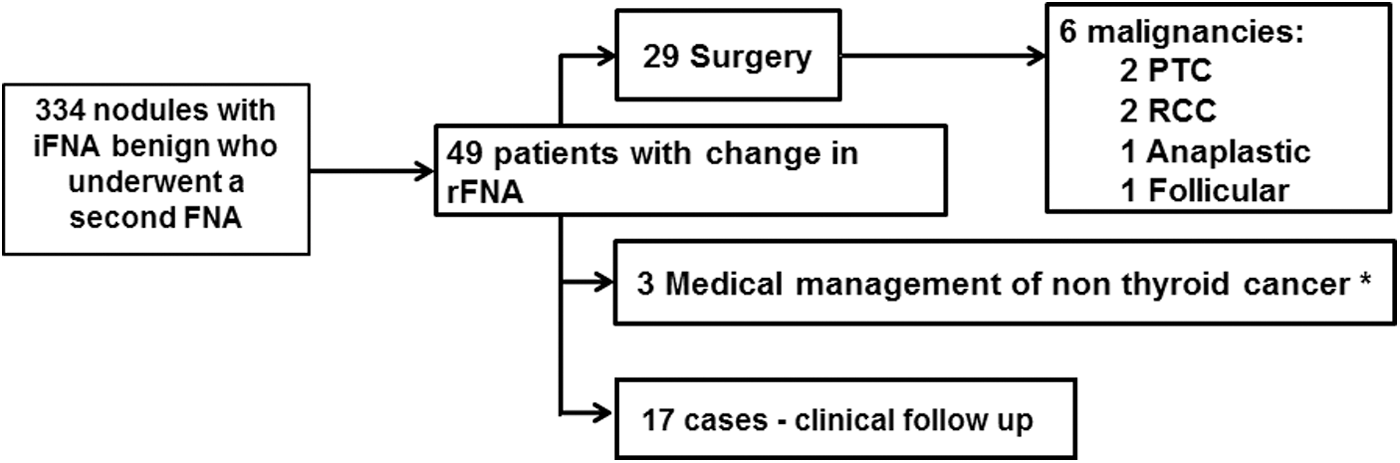
Change in medical management due to repeat fine-needle aspiration.
Anaplastic case was excluded.
One pathology report was not available.
When suspicious for malignancy and malignancy are combined.
PTC, papillary thyroid cancer; ATC, anaplastic thyroid cancer; FTC follicular thyroid cancer; CI, 95% confidence interval.
The rFNA showed malignancy in six cases, as shown in Figure 1. Among a total of 98 patients with a benign iFNA who underwent total or partial thyroidectomy (all indications), eight had documented malignancies in the index nodule on histopathology, with five of them being thyroid malignancies (three papillary thyroid cancers, one anaplastic thyroid cancer, one follicular thyroid cancer); in addition, there were two renal cell carcinomas and one lymphoma. Among these, there was a case in which iFNA was benign (cytology slides reviewed and diagnosis confirmed by T.J.S.), and 10 years later, the patient presented with rapid and painful growth of a mass in the same lobe and was found to have anaplastic thyroid cancer. This patient was excluded from the diagnostic analysis, since this was clearly a recent development given time lag and clinical change between the two biopsies. There was one case in which the index nodule had a needle track and benign histology, while a papillary thyroid cancer was found adjacent to this nodule. This case was considered as a diagnostic discrepancy due to a sampling error. A description of the various malignancies encountered in this group of patients is reported in Table 4. The proportion of patients with thyroid malignancy in the group of patients that underwent surgery was 4.1%. The proportion of patients with thyroid malignancy when considering the entire cohort was 1.2%.
No surgery performed.
Discussion
During a 10-year period, 334 nodules with benign iFNA underwent rFNA most commonly due to documented growth during follow-up (64%). The rFNA altered clinical management in 32 (9.5%) patients. The calculated proportion for thyroid cancer was 1.2% when long-term follow-up data in the entire cohort with rFNAs were used as the gold standard, and 4.1% when using surgical pathology only in the smaller subgroup that underwent surgery.
The present results are consistent with the current literature looking at rFNA in nodules with benign iFNA, demonstrating that the majority of rFNA are benign. For example, in a study looking at the value of rFNA of thyroid lesions that included an analysis of 10, 000 USFNAs, the rFNA of a benign iFNA yielded a benign diagnosis in 90.5% (13). In another study by Gabalec et al., evaluating 574 initially benign nodules, rFNA yielded a benign cytology in 87% of the cases. No cases of papillary thyroid cancer in the index nodule were found in the 153 patients with initially benign thyroid nodules who underwent surgery, although 10 incidental microcarcinomas outside the index nodule were found; among the 76 patients in which the rFNA changed to malignant/suspicious, 58 patients underwent surgery, and 13 carcinomas were detected (14). Similar results have been reported in the study by Kwak et al. in which 90% of the repeat biopsies remained benign and the FN rate was found to be 1.9%. In that study, the most common cause for repeat biopsy was nodule size of >2 cm regardless of growth (36.7%), followed by physician or patient concern (31.5%), and growth during follow-up (22.3%) (8). In comparison, the most common cause for rFNA in the present cohort was a clinical assessment of growth during follow-up.
In contrast with the present findings are the results of the study by Flanagan et al., in which of 111 patients with a benign iFNA, 57 underwent a rFNA yielding a benign result in only 60% of the cases, and changing clinical management in 16% (15). Another small study of 35 patients with benign iFNA that underwent rFNA found that the cytological diagnosis remained benign in only 20% (16).
Another interesting point is that the rate of malignancy found among those patients whose rFNA was either “suspicious for malignancy” (20%) or “suspicious for follicular neoplasm” (6.3%) was significantly lower than the expected rate of malignancy at the authors' institution in samples with the same cytological diagnosis on initial biopsy (usually ∼75% for suspicious for malignancy and ∼15% for suspicious for FN) (17). This suggests that the rFNA in these categories might have changed the management in this group of patients toward a surgical intervention that in most cases did not yield a malignant result. This observation might suggest a lower threshold in classifying a rFNA as suspicious by the pathologist, thereby subjecting an unnecessarily higher percentage of patients to surgery for benign nodules.
Methodologically, the evaluation of the diagnostic accuracy of USFNA and the value of rFNA is a challenge. First, there is a high chance of differential verification bias, since the majority of the patients would not undergo the gold standard for diagnosis, in this case histological evaluation after thyroidectomy (18). This is the case, since one of the main goals of USFNA is to identify benign thyroid nodules so that unnecessary surgery may be avoided. This inevitably will result in the use of different gold standards to establish a benign diagnosis, such as two or more negative biopsies, or the long-term follow-up of the complete cohort in which no diagnosis of thyroid cancer was made. This is evident in the present study, in which the proportion of thyroid cancer varies from 1.2% to 4.1% depending of the gold standard used. Second, there are many factors that can be related to USFNA results such as nodule characteristics (e.g., size), operator characteristics (e.g., level of experience), and cytology interpretation (e.g., level of expertise). All these variables may result in significant variability in diagnostic accuracy of USFNA and subsequent FNR in populations from different centers (14,19).
It is important to note that of all the malignancies (n = 8) identified on histology in the present cohort, three were nonthyroid malignancies (two metastases from renal cell carcinoma and one lymphoma), and one was a newly diagnosed anaplastic carcinoma. In the two cases of metastatic renal cell carcinoma, the patients had a previous history of renal cell cancer; there was an increase in the size of the nodule during follow-up, with time to rebiopsy of one year and two years, respectively. In the case of the B-cell lymphoma, the time to rebiopsy was two years, and there was evidence of growth but no previous diagnosis of malignancy. Initial FNA in this case was read as benign, with “cytological features consistent with Hashimoto's thyroiditis.”
The strengths of the present study include the large size of the cohort with long-term follow-up. The proportion of thyroid cancer in this study is consistent with previously reported results at the authors' institution (4). One of the major limitations of this study is that given its retrospective nature, there was no standardized protocol for the follow-up of the patients, and the decision to repeat thyroid ultrasound or biopsies was made by the various treating physicians and patients. A single tertiary care center's experience with thyroid nodules with benign iFNA that underwent a rFNA for clinical reasons is reported. In addition, the cohort most likely represents a high-risk population, since rFNA was only performed in those patients in whom there was a clinical indication for repeat USFNA, most commonly documented growth of the nodule during follow-up or physician/patient concern, and detailed information of the patients with an iFNA that was benign and never had a repeat biopsy is not available. Due to this limitation, the results might provide an overestimation of the changes in rFNA. There was also a reliance on the clinician's documentation to determine the reasons for rFNA and thyroidectomy, which introduces a measurement bias, since the determination of growth during follow-up was based on the clinician and/or radiologist report of significant growth, rather than on a prospective measurement and calculation of change in size or volume. In addition, care was taken to decrease the change of sampling error as the cause of a different rFNA result by including in the analysis only patients in which, to the best of the authors' knowledge, the same nodule was evaluated by rFNA. This decreases the generalizability of the results, when counseling patients with multinodular goiter, where a follow-up ultrasound might change management based on findings on different nodules.
The study was focused on patients with initially benign FNA cytologies who underwent rFNA, but the yield of rFNA in patients whose initial biopsy result were in other diagnostic categories was not studied. Repeat aspiration biopsies of thyroid nodules are usually performed in the setting of nondiagnostic results, or cases of atypia of undetermined significance (AUS) and follicular lesion of undetermined significance (FLUS), to obtain further diagnostic information that can guide management. At the authors' institution, the AUS/FLUS categories are not used, and the outcome of rFNA for previously nondiagnostic results has been previously reported (20).
Finally, the mean follow-up time of patients in this study was 4.0 ± 2.3 years, which might not provide a sufficiently long follow-up to assess clinical outcomes. A previous study that provided a mean follow-up of 8.5 years reported a mean time to thyroidectomy of 4.2 years (10).
Despite these limitations, the results indicate that in most cases in which rFNA of a nodule with a benign iFNA is performed, the results will not change management. Since at least half of the malignant results included nonthyroid malignancies in this potentially high-risk population, one should consider rFNA in patients with a known nonthyroid malignancy (particularly those that more frequently metastasize to the thyroid, such as melanoma, kidney, breast, and lung cancers) and thyroid nodules that are growing. For most other patients, growth alone, in the absence of other clinical or sonographic features of concern, rFNA cytology rarely yields a different result and may, in many cases, lead to unnecessary surgical intervention. Good communication between members of the interdisciplinary team (clinician, radiologist, and pathologist) may help circumvent some of the difficulties in the management of thyroid nodules. Based on the present findings and those of Durante et al. (12), current guidelines recommending rFNA based on change in size may need to be revisited to include development of other worrisome features beyond growth as main indication for rFNA in thyroid nodules with previous benign cytology.
Footnotes
Acknowledgment
This study was presented as an abstract at the American Thyroid Association meeting in October, 2014, Coronado, California.
Author Disclosure Statement
None of the authors has any conflicts of interest to report.