
Abstract

Over the past decade, transaxillary robot-assisted thyroidectomy (TRAT) has played a growing role in the management of thyroid nodules. TRAT offers the benefit of avoiding neck scarring, and is also considered safe and effective for treating small symptomatic goiters, Graves' disease, and thyroid carcinomas in experienced hands (1). Despite thousands of patients being operated on in Asia for a long time, few cases of ectopic subcutaneous thyroid tissue (STI) presenting as new palpable masses several years after the original endoscopic thyroid surgery have recently been described (2,3). In our center, 60 patients underwent a gasless TRAT between 2011 and 2014. Twenty of these patients had papillary carcinomas, and 19 of them subsequently underwent radioiodine therapy (RIT). 131I whole-body scans (WBSs) performed after RIT revealed that two of these patients had an abnormal uptake located in the surgical pathway, thus suggesting STI.
The two patients, women aged 33 and 39 years (see Fig. 1, panels 1 and 2, respectively), each presented initially with a single thyroid nodule (30 and 40 mm, respectively) in the right lobe, with nonsuspicious ultrasonography and cytological characteristics, but they reported some cervical discomfort. They underwent unilateral TRA lobectomy. In both instances, the histopathological examinations revealed differentiated papillary carcinomas without capsular invasion; the lesion accounted for as much as 60% of the volume of a colloid nodule in patient 2. TRA completion thyroidectomy on the contralateral side, and adjuvant RIT (3.7 GBq after levothyroxine withdrawal) were performed three months later. In both patients, 131I WBS (Fig. 1, panels 1a, 2a) and single photon emission computed tomography (CT; Fig. 1, panels 1cd, 2cd) displayed usual uptake by the orthotopic residual thyroid tissue but abnormal right chest wall uptake (arrows), located in the subcutaneous tissues used for the first surgical TRA pathway. Fine-needle aspiration of the lesions was not possible because CT and ultrasonography were unable to identify the disseminated thyroid tissue clearly. At the time of the first RIT, the thyroglobulin levels were 47 and 4.62 ng/mL, respectively (thyrotropin values were 37 and 71.5 mIU/mL, and the antithyroglobulin antibodies were negative). The WBSs after the second RIT (3.7 GBq after recombinant human thyrotropin stimulation), performed to assure the disappearance of the STI, did not show any uptake (1b, 2b). Stimulated thyroglobulin and antithyroglobulin antibodies were undetectable. These markers remained undetectable at 18 and 36 months after the first RIT.
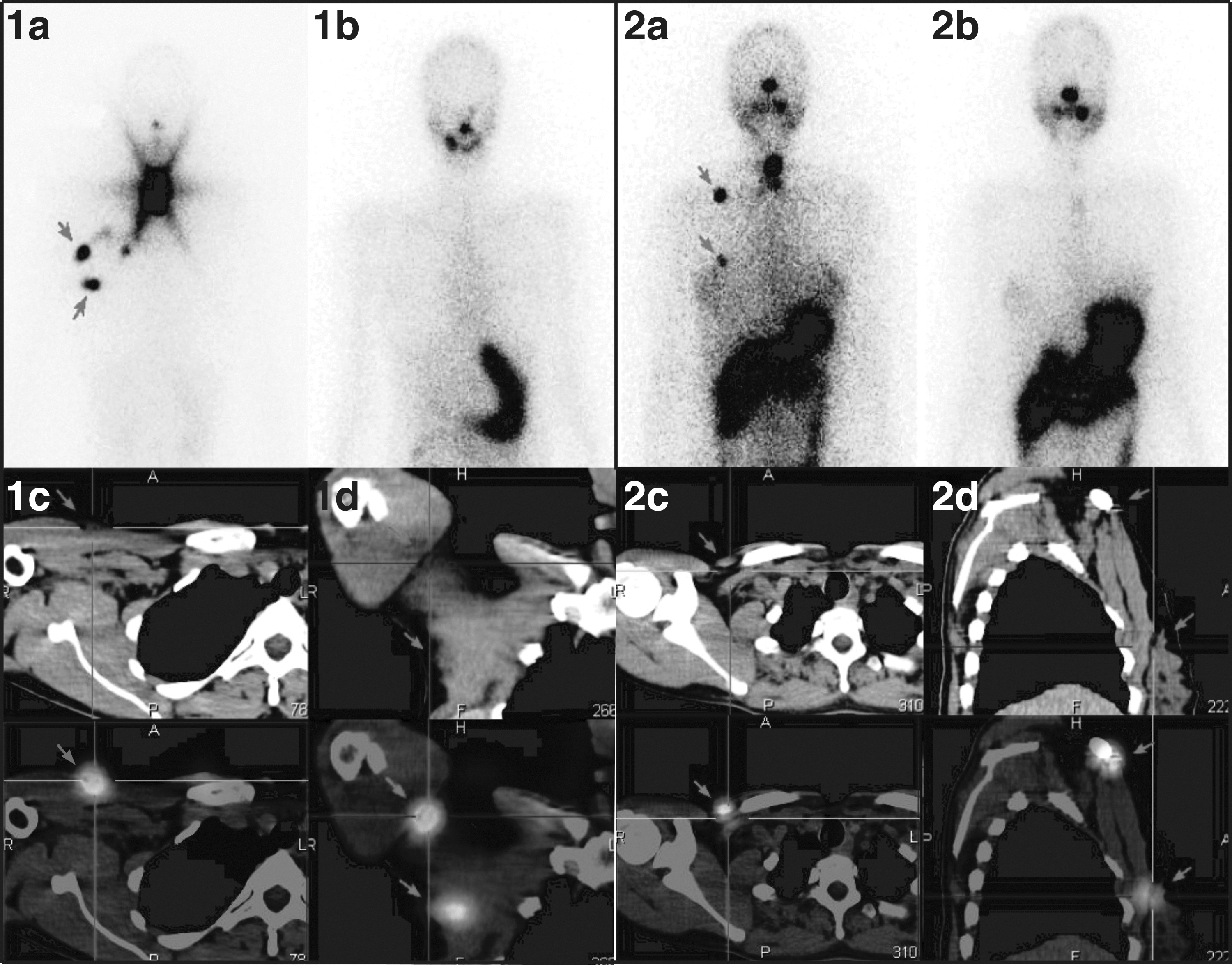
Imaging studies of the patients with subcutaneous implantation of thyroid tissue after transaxillary robotic thyroidectomy. Panel 1: patient 1; panel 2: patient 2. Whole body scan acquired two days after the first radioiodine therapy (RIT; 3.7 GBq after levothyroxine withdrawal; 1a, 2a) shows ectopic thyroid tissue (arrows). The ectopic thyroid tissue is no longer detectable on scans performed after a second RIT (3.7 GBq after recombinant human thyrotropin stimulation; 1b, 2b). Single photon emission computed tomography performed at the time of the first RIT demonstrates ectopic 131I uptake without clear underlying lesions (arrows): axial (1c, 2c), coronal (1d), and sagittal plane (2d).
The post-therapy scan after the initial RIT enabled us to discover STIs not detectable clinically or with other imaging modalities in our two patients, and allowed to destroy the disseminated cells. Dissemination secondary to thyroid capsule rupture is probably the cause of the STI (4), and it may be associated with the size of the nodules and the learning curve of the surgeon. Considering the increasing number of TRAs performed, we need to keep in mind that a small subset of patients develops STIs after TRA. As illustrated by our patients, these STIs may only be detectable through the demonstration of ectopic tissue uptake on diagnostic or post-therapy scans. Given the uncertainty of whether the ectopic tissue reflects disseminated benign tissue or thyroid cancer cells, this may be a relative indication for remnant ablation. Awareness that some patients may develop STIs is also of relevance for individuals undergoing TRA for benign disorders and may, in selected instances, require evaluation with dedicated imaging techniques.