
Abstract
Background:
Riedel's thyroiditis (RT) is a rare, fibroinflammatory condition which induces gradual thyroid gland destruction and adjacent soft-tissue fibrous infiltration. About one- seventh of RT cases are associated with hypoparathyroidism, necessitating long-term therapy for symptomatic hypocalcemia. The reversibility of the parathyroid hormone deficit has not been fully described.
Patient findings:
A 40-year-old woman with no prior history of thyroid disease presented with a six month history of progressive thyroid enlargement complicated by worsening dysphagia and positional dyspnea. Her past medical history was remarkable only for retroperitoneal fibrosis. Physical examination revealed a large, hard, non-mobile goiter. Thyroid indices while maintained on levothyroxine were normal, but marked asymptomatic hypocalcemia with an inappropriately normal parathyroid hormone level was noted. Thyroid imaging and fine needle aspiration were consistent with RT. Isthmectomy and subsequent serial corticosteroid and tamoxifen treatment led to rapid symptom improvement. Serum calcium and parathyroid hormone levels returned to the reference range within three months.
Summary:
We describe a case of RT in which hypoparathyroidism resolved after treatment targeted the mechanical compression and the fibroinflammatory milieu of the patient's thyroidal disease.
Conclusions:
RT can be associated with hypoparathyroidism that is clinically silent at presentation. Mechanical decompression of the goiter and immunomodulatory therapy can reverse the fibrosclerotic process and lead to rapid recovery of parathyroid gland function, as in this patient. However, in most cases hypoparathyroidism is persistent and requires continued treatment to prevent symptomatic hypocalcemia.
Introduction
R
Patient
A 40-year-old woman from East Africa presented with an enlarging goiter. She described rapid progressive thyroid enlargement over the preceding six months. This was accompanied by worsening dysphagia requiring her to take only small bites or sips; postural dyspnea with a sense of heaviness and tightness over the neck when lying supine that was relieved when lying in a lateral position; difficulty in turning her head to either side particularly while changing lanes when driving; and pain localized over the thyroid bed which radiated toward both ears. All symptoms were significantly affecting her quality of life.
The patient reported that her goiter had been incidentally discovered on physical examination approximately three years previously, at which time she had no associated symptoms. Fine needle aspiration performed at that time was unavailable at the time of presentation to our clinic, and the results were unknown to the patient.
A biochemical evaluation performed approximately 8 months prior to referral had led to the diagnosis of Hashimoto's thyroiditis (thyrotropin, 31 mIU/L; free thyroxine, 0.7 ng/dL; thyroid peroxidase antibodies, 586 IU/L), and levothyroxine 125 μg daily had been initiated. Despite this treatment, her thyroid gland had continued to enlarge. Given this enlargement and her associated symptoms, she was evaluated by a surgeon who described her thyroid gland as hard and fixed. She was subsequently referred to our institution for consideration of thyroidectomy.
The patient had lived in East Africa before immigrating to the United States nine years prior to our evaluation. She denied a family history of thyroidal illness, although iodine deficiency and goiter are endemic to most of East Africa. Her past medical history was significant for retroperitoneal fibrosis complicated by bilateral ureteral obstruction requiring surgical decompression. She had been treated with corticosteroids followed by tamoxifen for one year after surgery, without residual ureteral problems. At the time of her clinic visit, her only medications were levothyroxine and acetaminophen.
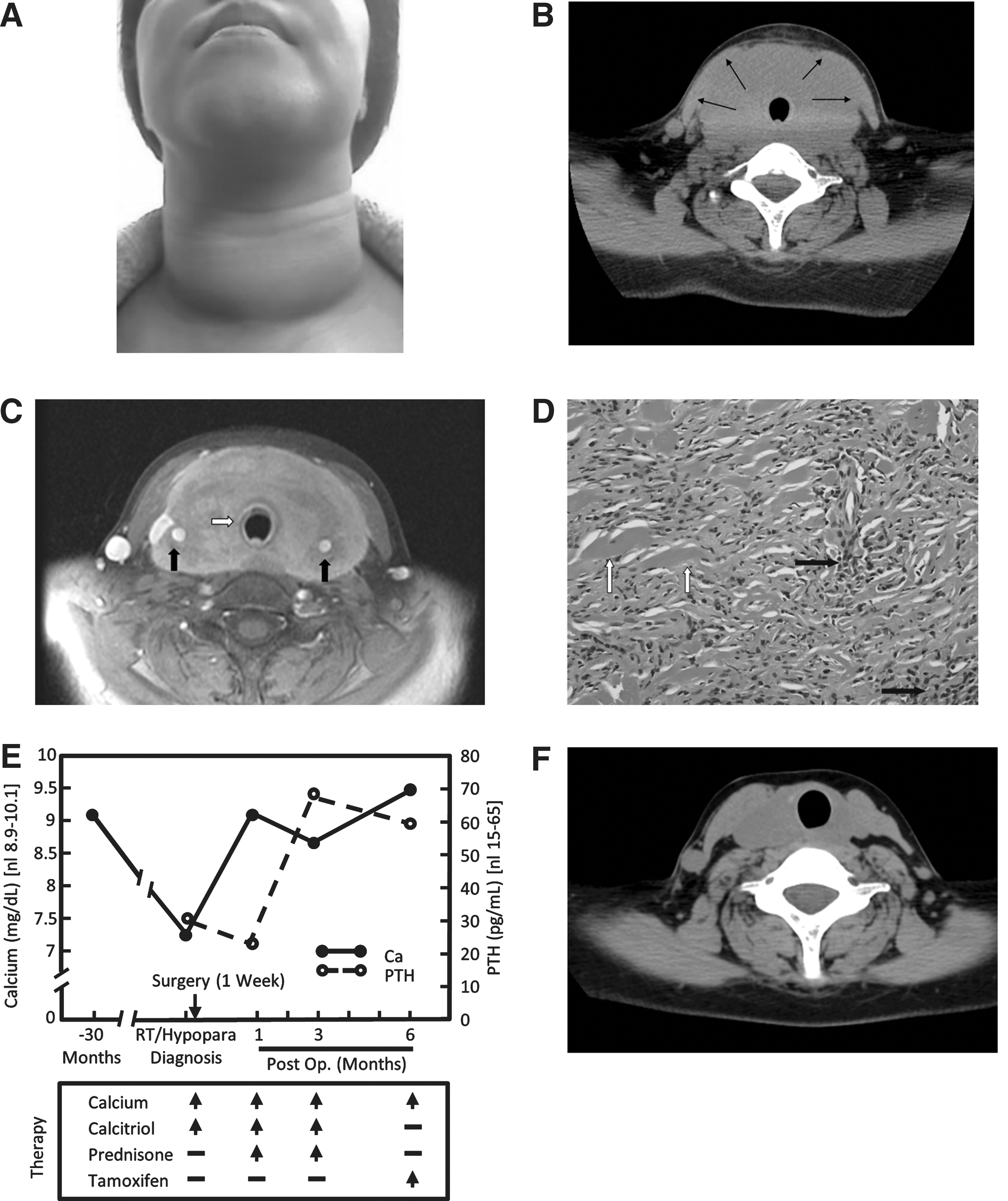
On physical examination, the patient was comfortable and in no acute distress. Physical examination revealed a large lobulated goiter that was very hard in consistency, non-tender, and limited the patient's cervical range of motion (Fig. 1A). Her attempts to swallow were slow and protracted despite taking only small sips of water. She was clinically euthyroid. Deep tendon reflexes were normal, and she had no muscle cramping during blood pressure measurement (no formal Trousseau test was performed). The remainder of her physical examination was unremarkable.
Laboratory
Biochemical data revealed the following: thyrotropin 3.9 mIU/L (0.3–5.0 mIU/L), free thyroxine 1.1 ng/dL (normal range 0.8–1.8 ng/dL), free triiodothyronine 3.3 pg/mL (normal range 2–3.5 pg/mL), and thyroid peroxidase antibodies 150 IU/mL (normal range <9 IU/mL). Notable was a markedly low serum total calcium (TCa) value of 7.3 mg/dL (normal range 8.9–10.1 mg/dL) with a concurrent phosphorus of 4.3 mg/dL (normal range 2.5–4.5 mg/dL), parathyroid hormone (PTH) 31 pg/mL (normal range 15–50 pg/mL), and a 25-OH vitamin D level of 40 ng/mL. Her albumin was 3.6 g/dL and the calculated corrected calcium was 7.7 mg/dL. After these results were available, she was questioned specifically for signs and symptoms of hypocalcemia, which she denied.
Imaging
Ultrasound demonstrated a markedly enlarged thyroid gland with a heterogeneous appearance. Computed tomography (CT) imaging revealed that the thyroid had an estimated volume of 310 cm3 with infiltration of the surrounding soft-tissue structures without a clear border (Fig. 1B, arrows). The trachea, carotid arteries, jugular veins, and the anterior portion of the esophagus were encased in this structure (Fig. 1C, arrows).
Pathology and clinical diagnosis
The physical examination and personal history of retroperitoneal fibrosis was highly suggestive of RT. Review of the previously performed outside fine needle aspiration revealed abundant follicular groups, in macro- and microfollicles, including some with Hürthle cell changes in a background of lymphoid cells. Given these collective data, our clinical diagnosis was Hashimoto's thyroiditis in conjunction with RT. In addition, the patient's serum calcium and PTH values were consistent with primary hypoparathyroidism. Given reports describing a relationship between RT and Immunoglobin G4–related disease (IgG4-RD), we performed IgG4 staining of both the thyroid tissue obtained during isthmectomy and the retroperitoneal tissue previously obtained at surgical decompression. Consistent with previous work, immunohistochemical staining of the retroperitoneal tissue demonstrated abundant IgG4-positive plasma cells in the fibroinflammatory process (greater than 30 per high power field), while immunoperoxidase studies performed on paraffin sections of the thyroid isthmus excision revealed comparatively fewer IgG4-positive plasma cells (data not shown). When considered in conjunction with the morphological features, these findings collectively support the involvement of IgG4-RD in both the thyroid and retroperitoneum.
Initial therapy
Although she was asymptomatic, the decision to treat with calcium supplementation and calcitriol was made preoperatively to prevent the development of symptomatic hypocalcemia. Levothyroxine replacement was continued. Given her compressive symptoms, she was referred for isthmectomy, which was subsequently performed with intraoperative ultrasound guidance to map and secure the carotid vessels.
Subsequent course
Thyroid pathology revealed marked fibrosis and sclerosis with chronic inflammation (Fig. 1D), and was similar to the fibrotic pattern previously identified in the retroperitoneum. These findings confirmed the diagnosis of RT. The patient was initiated on treatment with prednisone, 100 mg daily, which was slowly tapered to 20 mg daily over the course of 3 months, at which time tamoxifen was introduced at a dose of 10 mg twice daily along with continued prednisone tapering by 5 mg every 2 weeks until discontinuation. Within 1 month of surgery and glucocorticoid initiation, the patient noted significant symptomatic improvement and near complete resolution of her compressive symptoms. Three months after therapy, parathyroid function was robust (PTH 69 pg/mL, TCa 8.7 mg/dL), with calcium levels stabilizing in the normal range by 6 months (TCa 9.5 mg/dL, PTH 60 pg/mL; Fig. 1E). Due to limited dietary calcium intake, the patient was maintained on daily calcium supplementation, with her calcium level remaining normal (8.9 mg/dL) 1 year after surgery and 6 months after corticosteroid discontinuation. A CT scan obtained at that time demonstrated a significant decrease in thyroid size, with concomitant decreases in both the posterior and lateral soft tissue invasion (Fig. 1F).
Discussion
RT is a rare fibroinflammatory condition that causes gradual destruction of the thyroid gland and fibrous infiltration of adjacent soft tissues. The overall prevalence is low, with a reported rate of 0.06% of all thyroid surgeries and an outpatient prevalence of 1.06 per 100,000 patients in a single institution series (2). The clinical presentation is that of a goiter with remarkably hard consistency (comparable to wood or stone) and is often associated with compressive symptoms of dysphagia, dyspnea, neck discomfort, and/or voice changes.
Patients with RT are usually euthyroid unless there has been extensive replacement of the thyroid gland by fibrous tissue, although hypothyroidism at diagnosis has been documented in approximately 30% of cases (3). Elevated thyroid autoantibody levels have been reported in 67–80% of patients with RT (1,3) with pre-existing Hashimoto's thyroiditis or antibody generation due to thyroid gland destruction considered potential etiologies (4). On imaging by either ultrasound or CT, hypodense areas within the thyroid with infiltration of surrounding soft tissue (5,6) and encasement of the large neck vessels are common, as seen in Figure 1C. The magnetic resonance imaging appearance of focal, homogenous hypointensity in T1- and T2-weighted images is considered pathognomonic of RT (7 –9). The extent of extra-thyroidal fibrosis with involvement of the large vessels, trachea, and esophagus in addition to the soft tissues explains the surgical difficulties associated with these cases (10 –12). Given these concerns, we decided to limit surgical intervention to an isthmectomy in order to minimize the potential for surgical complications, including possible removal of residual parathyroid tissue, while still providing rapid relief of local pressure exerted over the trachea and esophagus given that subsequent medical therapy (anti-inflammatory and anti-fibrotic) was likely to further aid in the resolution RT-associated changes.
Several pathogenetic mechanisms have been proposed to explain RT. The systemic autoimmune hypothesis is most widely accepted due to the presence of antithyroidal antibodies; association with other autoimmune diseases like Graves' disease, pernicious anemia, and Hashimoto's thyroiditis; and the clinical response to therapy with glucocorticoids and tamoxifen. The association of RT with extrathyroidal distant fibrosclerosis has expanded the pathogenesis to a systemic fibroinflammatory process triggered by an as yet unknown antigen. More recently, several reports have indicated the involvement of IgG4 in RT pathophysiology (11,13). In the case described here, the association with retroperitoneal fibrosis and the presence of IgG4-positive cells in both tissues argue in favor of that association. The therapeutic response to therapy is also consistent with IgG4-RD. Given this, it is hopeful that future therapeutic advances in the IgG4-RD field will be proven beneficial to RT therapy as well.
The histologic outcome is a fibroinflammatory process involving all or a portion of the thyroid gland with areas of hyalinization and extension into surrounding tissues including the parathyroid glands and strap muscles (3,14,15). The inflammatory infiltrate is composed of lymphocytes, monocytes, granulocytes, and eosinophils without giant cells, lymphoid follicles, oncocytes, or granulomas, evidence of occlusive phlebitis due to infiltration of the small and medium sized veins by lymphocytes and plasma cells, and the absence of neoplasm.
Hypoparathyroidism has been described in association with RT (1,3,4,15). Signs and symptoms of hypoparathyroidism (muscle cramps, tetany, paresthesias, Trousseau's and Chvostek's signs) can precede or occur simultaneously with the presentation of RT. Gradual fibrotic infiltration of the parathyroid glands is thought to be the etiological mechanism. Vascular compromise with progressive ischemia related to extrinsic arterial compression may also contribute to parathyroid gland failure, given that the arterial supply to the parathyroids is usually provided by a single, very fine, and delicate vessel branching from the inferior or superior thyroid arteries (16). Although we sought to identify the parathyroid arteries in the obtained CT and magnetic resonance imaging images, their radiological signature remained below the current level of resolution.
Regarding autoimmune mechanisms, no identifiable antiparathyroid antibody was identified in one case where it was specifically sought (17).
While hypoparathyroidism is a well-recognized complication of RT, reversibility has rarely been documented. Whereas Chopra et al. (18) reported recovery of hypoparathyroid activity approximately 2 years (22 months) after partial thyroidectomy and levothyroxine replacement therapy, our data demonstrate recovery of parathyroid function can occur much more rapidly (within 3 months), perhaps reflecting the rapid impact of immunomodulatory therapy. Notably, recovery tracked closely with the precipitous decrease in size and degree of induration of the patient's goiter. Consistent with the potential for rapid parathyroid gland recovery is a report by Lo and colleagues (19), which inferred a similar phenomenon in a patient with RT due to the ability to discontinue calcitriol therapy and reduce calcium supplementation following isthmectomy and oral corticosteroid treatment over a 12-week interval. Unfortunately, however, no documentation of PTH values during the recovery phase was provided in that report.
As described, despite being hypocalcemic, our patient was asymptomatic from a calcium perspective, likely reflecting a slow diminution of her serum calcium value rather than a rapid precipitous decline. Regarding the recovery of her parathyroid function, we postulate that both relief of vascular compression after wedge resection coupled with arrest and reversal of the fibrosclerotic process with corticosteroids and tamoxifen treatment were the immediate causes. Few et al. (20) were the first to report a dramatic reduction in thyroid gland size with tamoxifen treatment in RT. Tamoxifen is a nonsteroidal antiestrogen previously used successfully for the treatment of RT (20) and retroperitoneal fibrosis (21 –23). Interestingly however, the tamoxifen-sensitive fibrotic masses seen in retroperitoneal and mediastinal fibrosis and the intrathyroidal fibrotic tissue in RT are generally estrogen receptor negative. It has thus been postulated that tamoxifen exerts its effects via inhibition of transforming growth factor–β release, resulting in the subsequent inhibition of fibroblast and epithelial cell proliferation (20,24,25).
Conclusion
Riedel's thyroiditis can be associated with hypoparathyroidism that is clinically silent at presentation. Mechanical decompression of the goiter and immunomodulatory therapy can reverse the fibrosclerotic process and lead to rapid recovery of parathyroid gland function. However, in most cases hypoparathyroidism is persistent and requires continued treatment to prevent symptomatic hypocalcemia.
Footnotes
Author Disclosure Statement
No competing financial interests exist.