
Abstract
Background:
Multiple gene mutations in thyroid nodules are rare. The presence of several oncogenic mutations could be associated with aggressive biological behavior of tumors.
Patient findings:
A 60-year-old female presented to her physician after she felt a lump in her neck. On ultrasound, she was found to have a 1.4 cm × 0.8 cm × 1.3 cm nodule in the isthmus and a 0.5 cm × 0.6 cm ×0.6 cm nodule with irregular margins and hypoechogenicity in the right thyroid lobe, warranting fine-needle aspiration (FNA). Cytological examination of the smaller nodule yielded a diagnosis of atypia of undetermined significance (AUS/FLUS, Bethesda Category III). The aspirate was submitted for molecular testing using the next-generation sequencing ThyroSeq® v2 panel. The test revealed four distinct mutations: BRAF (p.V600E), TERT (C228T), PIK3CA (p.H1047R), and AKT1 (p.E17K). Presence of multiple oncogenic mutations in the FNA specimen was highly indicative of cancer, and suggestive of a cancer with propensity toward more aggressive biological behavior. Four weeks after the FNA results were available, the patient underwent total thyroidectomy. This was followed by radioactive iodine ablation after the final pathology revealed a 0.5 cm papillary thyroid carcinoma (PTC) with extrathyroidal extension and positive resection margins (pT3 stage).
Summary:
Herein, the first case of four mutations preoperatively detected in a subcentimeter thyroid nodule that was confirmed to be a PTC with aggressive biological behavior is reported.
Conclusions:
The judicious indication of FNA and use of molecular screening can potentially help in predicting aggressive behavior of small-sized thyroid cancers and in identifying patients who may benefit from early and more extensive therapy.
Introduction
T
In addition to its utility as a diagnostic tool, gene mutation panels such as the ThyroSeq® multigene panel may also be used to assess the potential for aggressiveness of a thyroid cancer. While a single driver mutation, such as BRAF or RAS, may be sufficient to initiate thyroid tumor development, aggressive or poorly differentiated tumors acquire and accumulate additional mutations that promote tumor progression (4,6). Tumors with multiple mutations more often have lung metastases (BRAF and TP53) and local recurrence (BRAF, TP53, and PIK3CA) (4). Here, the case is presented of a patient with four oncogenic mutations in a single nodule that had propensity for aggressive biological behavior.
Patient
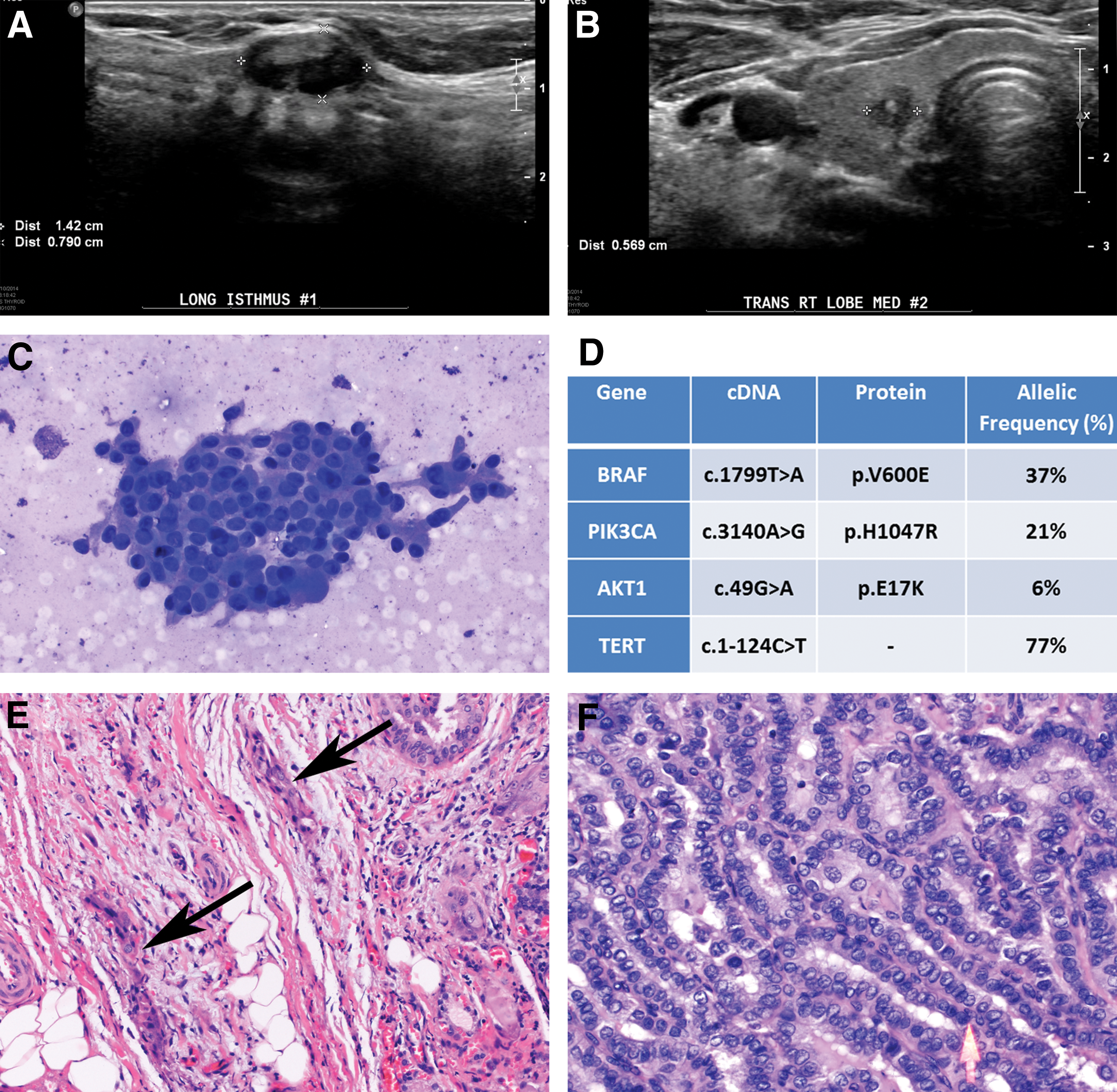
A 60-year-old female with a history of migraine headaches, depression, and anxiety presented to her family doctor after she noticed a small lump in the left side of her neck. Physical exam suggested a small lymph node on the anterior border of the left sternocleidomastoid that was confirmed by neck ultrasound. Thyroid function tests were normal. Three months later, the patient noticed another lump, this time in the thyroid region, and was referred to Endocrinology. No risk factors for thyroid cancer were noted in her history. A 1–1.5 cm isthmus nodule was felt on physical exam. Thyroid ultrasound confirmed a 1.4 cm × 0.8 cm × 1.3 cm mixed solid and cystic nodule in the isthmus (Fig. 1A) and also revealed a 0.5 cm × 0.6 cm × 0.6 cm solid thyroid hypoechoic nodule with irregular borders and a possible central calcification in the right thyroid lobe (Fig. 1B).
(
Access was not available to the images of the initial neck ultrasound, and therefore it could not be determined whether these nodules were previously present. Considering the size of the larger nodule and the suspicious characteristics of the smaller one, FNA of both nodules was performed. Cytological examination of the 1.4 cm isthmus nodule yielded a benign diagnosis, whereas the examination of the 0.6 cm right-lobe nodule yielded a diagnosis of atypia of undetermined significance (AUS/FLUS, Bethesda Category III). This was based on scant cellularity and focal cytological atypia characterized by enlarged hyperchromatic cells with increased nucleus to cytoplasmic ratio and nuclear elongation with grooving (Fig. 1C). A second population of atypical cells with Hürthle cell–like features and nuclear abnormalities was also noted. As per the authors' institution's protocol, this AUS/FLUS category III FNA specimen was sent for molecular testing to refine the diagnosis. The ThyroSeq® v2 test, performed at the University of Pittsburgh, identified the presence of four mutations—BRAF (p.V600E), TERT (C228T), PIK3CA (p.H1047R), and AKT1 (p.E17K)—at various frequencies (Fig. 1D).
Since BRAFV600E positivity by itself is highly indicative of malignant thyroid tumors, particularly PTC, and the simultaneous presence of other hotspot mutations in TERT, PIK3CA, or AKT1 have been reported in association with aggressive and/or dedifferentiated thyroid cancers (4,6,7), the result of molecular testing was highly suspicious for an aggressive form of thyroid cancer (2). Based on the results of molecular testing and after discussion with the patient, a total thyroidectomy with central compartment lymph node dissection (level 6) was performed. Surgical pathology examination revealed a 0.5 cm PTC in the right thyroid lobe with extrathyroidal extension and positive resection margins (Fig. 1E). The tumor had a classical papillary histology with well-developed nuclear features of PTC, without evidence of poorly differentiated or anaplastic areas (Fig. 1F). Examination of the three level 6 right lymph nodes removed revealed no tumoral involvement. The original lymph node felt on the left side of her neck was found be benign fibro-adipose tissue. A 123I whole body scan, performed after Thyrogen® stimulation, did not show residual uptake at the thyroid bed or at distant sites. The patient was treated with 89.3 mCi of 131I. The whole body scan seven days after treatment showed residual uptake in the thyroid bed. The patient is doing well and remains on levothyroxine replacement.
Discussion
The tumor reported here had four well-characterized oncogenic mutations based on ThyroSeq® v2 testing. The ThyroSeq® v2 is a targeted next-generation sequencing test that assesses the presence of point mutations in 14 thyroid cancer–related genes and gene rearrangements in 42 thyroid cancer–related genes, along with measuring expression levels of eight control genes to allow for assessment of the cell lineage of the collected sample (5). The BRAFV600E mutation is the most common mutation associated with classical PTC (8,9). This mutation has been linked to poorer clinical prognosis (10), although it is likely that, in isolation, the BRAFV600E mutation does not possess sufficient specificity to identify PTCs with unfavorable outcomes.
More recently, TERT promoter region mutations (C228T and C250T) have been found in more aggressive thyroid tumors (7,11), and recent data from a large series found TERT mutations to be an independent predictor of development of recurrence and distant metastases, as well as tumor-related mortality in well-differentiated papillary and follicular thyroid cancers (12). Furthermore, tumors with co-existing BRAF and TERT mutations may have higher recurrence rates within the first two years of diagnosis compared with patients harboring neither of these mutations in isolation (13). Two other mutations found in this FNA sample, PIK3CA and AKT1, are rare in well-differentiated thyroid cancers and considered to be a late event arising during tumor expansion and dedifferentiation. In the recent The Cancer Genome Atlas (TCGA) study, involving approximately 400 patients with well-differentiated PTCs, only three (0.8%) tumors were found to carry an AKT1 mutation, and two (0.5%) a PIK3CA mutation (14). These five (1.3%) tumors also had a BRAFV600E mutation, and none of the tumors in the TCGA data set showed a co-occurrence of BRAF, PIK3CA, or AKT1 mutations. This indicates, as discussed, that multiple mutations are rare in PTCs, and supports previous observations showing a more frequent occurrence of multiple mutations, typically BRAF and PIK3CA or BRAF and AKT1, in more advanced, poorly differentiated, and iodine-refractory thyroid cancers (4,6). Interestingly, in this sample, the BRAF mutation was found with an allelic frequency of 37%, which corresponds to 74% of cells in the sample being positive for this mutation, whereas PIK3CA mutation was seen with an allelic frequency of 21% and the AKT1 mutation with an allelic frequency of 6% (Fig. 1D), which may suggest that the latter two mutations arose later during tumor progression.
In the present patient, despite the relatively small tumor size, the analysis of the DNA sample collected during the tumor nodule sampling revealed not only BRAF and TERT mutations, but also pathogenic PIK3CA and AKT1 mutations. The presence of the four mutations in a single tumor predicted a potential for highly aggressive disease, leading to the offer of total thyroidectomy as the initial surgical approach. The resected tumor, although only 0.5 cm in size, demonstrated extension into adjacent perithyroidal tissue, and although long-term data are limited, it is likely that if not removed, this tumor could undergo dedifferentiation and spread to distant sites. Current guidelines do not recommend 131I therapy in unifocal thyroid cancers <1 cm without other risk features (15). This patient, however, had extrathyroidal extension of the tumor, and positive margins, which may, per se, indicate a higher risk of recurrence and may call for selective use of radioiodine therapy. In addition, although current guidelines do not yet incorporate management based on the presence of genetic mutations, the mutations detected in this relatively small tumor are associated with more aggressive cancer behavior, as discussed above. Whether these patients will truly benefit from more aggressive surgery and radioiodine therapy is yet to be determined.
To the authors' knowledge, this is the first reported case of four oncogenic driver mutations documented in a single thyroid nodule. The detection of multiple gene mutations was decisive in the planning of thyroidectomy, which was later proven to be the most appropriate approach considering the presence of extrathyroidal extension at final pathology. Thus, this report supports the concept that the presence of multiple mutations in PTCs is associated with more aggressive tumor behavior. It also demonstrates the potential impact of molecular screening of even small-sized thyroid nodules in identifying candidates for more aggressive therapy, although the benefits of such approach are yet to be determined. Finally, this case highlights the importance of using multigene panels for tumor prognostication, as detection of a single gene mutation, such as BRAF, may not be sufficient to identify thyroid cancers with more aggressive biological behavior.
Footnotes
Author Disclosure Statement
Y.E.N., employer, University of Pittsburgh Medical Center, has a service agreement with CBLPath/Sonic Health Care Company to offer ThyroSeq® for commercial use. R.T.S., A.K., K.A., and M.L.C have nothing to disclose.