
Abstract
Background:
This study aimed to analyze the temporal changes of the clinicopathologic characteristics, and the long-term outcomes, of various types of anaplastic thyroid cancer (ATC) and poorly differentiated thyroid cancer (PDTC).
Methods:
A retrospective analysis was conducted on patients with ATC and PDTC who were treated from 1985 to 2013. The outcome measures included the clinical response to treatment and the survival rates of three separate thyroid cancer groups: ATC, PDTC, and differentiated thyroid cancer (DTC) with anaplastic foci.
Results:
The five-year disease-specific survival rate was significantly higher, both in DTC with anaplastic foci and in PTDC (81.3% and 65.8%, respectively), than it was in ATC (14.3%; p < 0.001). The proportion of cases of DTC with anaplastic foci has been increasing over time, while that of ATC has decreased. The survival rate was found to be significantly higher in resectable tumors (71.4% and 26.5%, respectively; p < 0 .001). In ATC, external beam radiation therapy showed longer survival rates than did surgery-based treatment in unresectable tumors (19.2 vs. 7.7 months, p = 0.006). Adjuvant treatment with external beam radiation or radioactive iodine increased survival duration in PDTC and in DTC with anaplastic foci. Lymphatic invasion was the most significant postoperative prognosticator in ATC (p = 0.013).
Conclusions:
The choice of treatment of ATC and PDTC could be modified according to resectability and lymphatic invasion of the cancer.
Introduction
T
Although ATC is one of the most virulent and aggressive of all malignancies, showing extremely short survival outcomes regardless of treatment modality (8,9), tumors with small anaplastic foci in the background of DTC have been reported to have better prognoses (7). Moreover, PDTC has a better prognosis than does ATC, although treatment-refractory disease can occur, not infrequently with death as the outcome (10). Given these reported better outcomes of tumors with anaplastic foci in the background of DTC and of PDTC (7), and the various differing prognoses according to the histologic components, the evaluation of the clinicopathologic characteristics of the changes and the outcomes of ATC or PDTC has become important for appropriate management. However, until recently, only a limited number of studies regarding the various types of ATC and PDTC have been reported.
Therefore, this study aimed to analyze the temporal changes of the clinicopathologic characteristics of ATC or PDTC according to their histologic components, and to compare their survival outcomes and related factors.
Materials and Methods
Subjects
A retrospective chart review was performed on 184 patients who were diagnosed with ATC or PDTC at Seoul National University Hospital from January 1985 to December 2013. The medical records were reviewed, including year of diagnosis, sex, age at diagnosis, blood chemistry, tumor pathology, stage, method of treatment, and follow-up and survival duration from the date of diagnosis. Tumor size was defined either as the maximal diameter of the surgical specimen or the size as measured by imaging modalities (usually computed tomography [CT] scan). To evaluate the time trend regarding diagnosis, treatment, and survival outcomes, the subjects were divided according to the study period as follows: (i) from 1985 to 1994, (ii) from 1995 to 2004, and (iii) from 2005 to 2013. This study was conducted in accordance with the principles of the Declaration of Helsinki, and approved by the Institutional Review Board of Seoul National University Hospital (No. B-1405-096-580).
Definition of pathologic findings and categorization
Pure ATC was defined as a tumor with no demonstrable areas of coexisting DTC. ATC arising from DTC was defined as a tumor in which >10% of its volume was occupied by undifferentiated cells, while DTC with anaplastic foci was defined as a tumor in which <10% of the tumor volume was occupied by undifferentiated cells in the background of differentiated cancer. Because there is not yet a definitive established pathologic definition of these categories, the definitions adopted in this study were based on the experience of clinicians and pathologists. The ATC component in tumors mixed with DTC was defined based on the following features: the nuclei without the characteristic features of DTC and showing a greater ratio of nucleus/cytoplasm, nuclear pleomorphism other than the features of DTC, and a more solid growth pattern with or without p53 expression. Recurred ATC from DTC was defined as a recurrent tumor with undifferentiated cells in a patient who was diagnosed as DTC at the first operation, but with a DTC component detected in the recurrent tumor. PDTC was defined on the basis of the Turin proposal for the use of uniform diagnostic criteria (11). For the purposes of accurate diagnosis, previous pathologic specimens were re-evaluated by a pathologist (J.K.W.) in 22 (57.9%) of cases where the slides were available and confirmed as PDTC if showing a solid/trabecular/insular growth pattern with the absence of conventional nuclear features of papillary carcinoma, and the presence of at least one of the following features: tumor necrosis, mitotic count ≥3/10 HPF, or convoluted nuclei. Based on the primary diagnosis, pure ATC, ATC arising from DTC, and recurrent ATC from DTC were combined as one ATC group. Therefore, patients were thus categorized into three groups: ATC, DTC with anaplastic foci, and PDTC.
Treatment and survival outcomes
The resectability of the tumor was determined by interpretation of the preoperative CT scan or magnetic resonance imaging (MRI) by two independent experienced head and neck surgeons who were blinded to the clinical data. A resectable tumor was defined as a tumor that was expected to be completely removed with an adequate safety margin. An unresectable tumor was defined as a tumor invading extensively into the laryngotracheal, esophageal or prevertebral space, or the carotid arteries or jugular veins, which could not be resected even with aggressive surgery (i.e., total laryngectomy, tracheal resection and anastomosis, pharyngoesophagectomy with reconstruction, and vascular reconstruction). There was no standardized treatment and follow-up strategy. Surgical removal, external beam radiation therapy (EBRT), radioactive iodine (RAI) therapy, or chemotherapy was given based on each patient's individual status and the patient's own decision. Treatments were categorized according to the first-line treatment modality given as follows: (i) operation (OP)-based (surgical treatment with or without adjuvant therapies, n = 137), (ii) EBRT-based (EBRT with or without chemotherapy, n = 19), (iii) chemotherapy (n = 7), and (iv) none (n = 21). A total of 124 patients (67.4%) were treated with curative intent (122 patients by surgical resection and two by EBRT). Among 137 patients who received an OP-based treatment, total thyroidectomy (n = 110, including two cases of total laryngectomy) or near- or subtotal thyroidectomy (n = 12) was performed to remove the tumors as completely as possible, while palliative debulking surgery for decompression was performed in 15 patients (7.8%) to control tumor bleeding or airway obstruction. Adjuvant EBRT was performed in 77 patients after the operation. Among the 19 patients who received EBRT-based treatment, two patients were treated with curative intent, and subsequently received adjuvant chemotherapy. The remaining 17 patients were treated with palliative intent. Of these, one patient received adjuvant chemotherapy. Radioactive iodine therapy was performed in 28 patients.
Data regarding disease-specific mortality were reviewed based on the medical records or the Statistics Korea national database, and one-year, two-year, and five-year disease-specific survival rates were calculated.
Statistical analysis
Continuous outcomes were analyzed using independent t-tests between groups of two, and one-way analysis of variance (ANOVA) among groups of three or more. Dichotomous outcomes were analyzed using the chi-square test for trend and logistic regression analysis. Survival curves were compared using a log-rank test. Cumulative recurrence and mortality rates were calculated by life table, and a log-rank test was performed to analyze the changes in outcome. Cox regression analysis was performed to assess the difference in risk factors for survival, and values were presented as hazard ratios (HR), confidence intervals (CI), and p-values. In multivariate analysis, the models were divided according to the preoperative, intraoperative, and postoperative findings, which were adjusted with the pre-existing risk factor of ATC. All statistical analyses were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). Statistical significance was defined as p < 0.05.
Results
General characteristics and differences according to the time of diagnosis
A total of 184 patients were included in this study. The mean age at diagnosis was 59.4 ± 15.0 years, and the male-to-female ratio was 1:2.12. The median follow-up duration was 38.9 months (range 1–207 months). Among 137 patients who received OP-based treatment, total thyroidectomy (n = 110, including two cases of total laryngectomy) or near- or subtotal thyroidectomy (n = 12) was performed to remove the tumors as completely as possible, while palliative debulking surgery for decompression was performed in 15 patients (7.8%) to control tumor bleeding or airway obstruction. Adjuvant EBRT was performed in 77 patients after the operation. Tracheostomy for palliative airway management was undertaken in 27 patients, but tracheostomy alone was not considered as a treatment. Among the 19 patients who received EBRT-based treatment, two patients were treated with curative intent, and they received adjuvant chemotherapy. The remaining 17 patients were treated with palliative intent, and among these, one patient received adjuvant chemotherapy.
Age at diagnosis and sex ratio did not differ among the three time periods (Table 1). The absolute number of patients in all three diagnostic groups increased over time. However, the relative proportion of patients with ATC decreased significantly (p < 0.001), while that of DTC with anaplastic foci increased, and that of PDTC remains unchanged over time. Patients who underwent surgery and those with a resectable tumor also significantly increased during the time periods (p < 0.001 and p = 0.001, respectively). Preexisting known goiter or tumor was more prevalent in the period 1985–2004 than in the period 2005–2013 (p = 0.002). Tumor size and nodal status were not significantly different among the three time periods, although there was a trend of a decrease in tumor size and positive lymph nodes. OP-based treatment and survival rate were significantly increased during the time periods (p < 0.001 and p < 0.001, respectively).
Proportion of the patients among the OP-based treatment and pathologic review was possible.
ATC, anaplastic thyroid cancer; PDTC, poorly differentiated thyroid cancer; DTC, differentiated thyroid cancer; OP-based, operation based; EBRT, external beam radiation therapy; YSR, year survival rate.
Statistical significance was defined as p < 0.005 (bold).
Comparison of clinical pathologic characteristics and survival among the different pathologic groups
When comparing the five-year disease-specific survival, ATC showed significantly lower survival rates compared with those in DTC with anaplastic foci and PDTC (Fig. 1, Table 2, and Supplementary Table S1; Supplementary Data are available online at
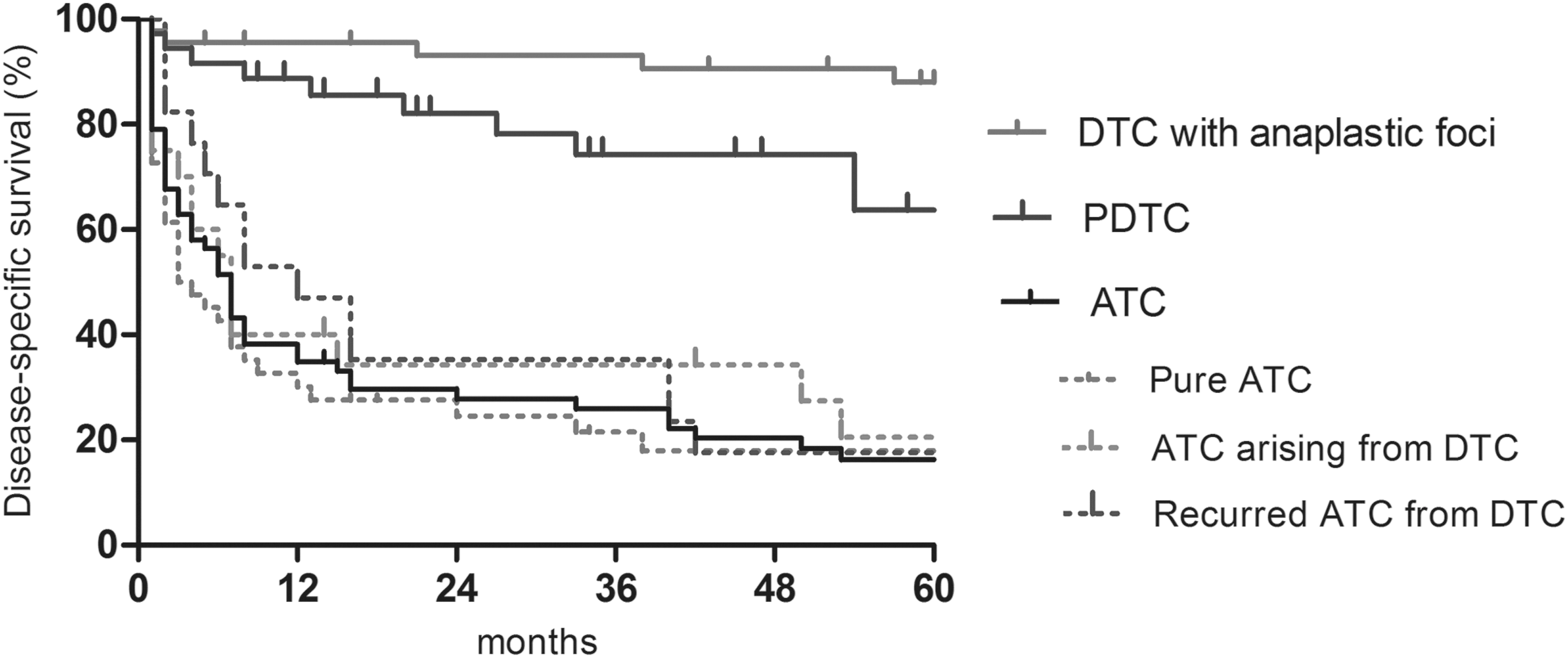
Comparison of disease-specific survival according to diagnosis. DTC, differentiated thyroid cancer; PDTC, poorly differentiated thyroid cancer; ATC, anaplastic thyroid cancer.
Resectability, tumor size, T category, nodal status, and distant metastasis were evaluated among the patients whose imaging modalities were available.
Age at diagnosis was older in ATC, and sex ratio showed no significant difference among the three pathologic groups (p < 0.001 and 0.983, respectively). A previous history of goiter was more prevalent in ATC (36.7%) than it was in PDTC (26.3%) and DTC with anaplastic foci (4.2%; p < 0.001). Small resectable tumors with less advanced stages were more prevalent in DTC with anaplastic foci, followed by PDTC (Table 2). When comparing the clinicopathologic factors between survival and non-survival, T category, M category, resectability, tracheal invasion, treatment modality, and lymphatic invasion were significantly different in ATC (p = 0.027, 0.008, 0.002, 0.024, 0.039, and 0.007, respectively). Age, resectability, tracheal invasion, and treatment modality were different in PDTC (p = 0.002, 0.006, 0.026, and 0.010, respectively), while age, resectability, treatment modality, lymphatic invasion, vascular invasion, and positive resection margin are different variables between survivor and non-survivor in DTC with anaplastic foci (p < 0.001, p = 0.032, 0.032, 0.001, 0.002, and 0.011, respectively; Table 3).
Statistically significant (p = 0.027, 0.008, 0.002, 0.024, 0.039, and 0.007 in T4b category, distant metastasis, resectability, treatment modality, and lymphatic invasion of ATC, respectively; p = 0.002, 0.006, and 0.010 in age, resectability, and treatment modality of PDTC, respectively; p < 0.001, p = 0.018, 0.032, 0.032, 0.001, 0.002, and 0.011 in age, sex, resectability, treatment modality, lymphatic invasion, vascular invasion, and positive resection margin of DTC with anaplastic foci, respectively).
WBC, white blood cells; NA, not available.
Survival outcomes according to the treatment methods in ATC
Survival outcomes were significantly higher in those patients with resectable tumors than in those with unresectable tumors (Supplementary Fig. S1). In resectable tumors, those treated solely with surgery and those with surgery and adjuvant EBRT (n = 31) showed no significant difference in their clinicopathologic characteristics. Although survival was not significantly different between the two groups, the median survival duration was longer in those patients treated with additional EBRT (25.9 vs. 43.6 months, p = 0.345; Fig. 2A, Table 4, and Supplementary Table S2). Among 38 patients with unresectable tumors, survival rates were significantly different according to the treatment modality (Fig. 2B), and patients who underwent EBRT-based treatment showed the longest median survival of 19.2 months (p = 0.007; Table 4, and Supplementary Table S2). Multivariate analysis revealed that resectability (unresectable tumor, OR = 1.39 [CI 1.21–1.74]) and tracheal invasion (OR = 4.45 [CI 2.32–9.33]) were the most significant factors in the preoperative findings (p = 0.004 and 0.042, respectively), while lymphatic invasion (OR = 4.87 [CI 1.40–16.97]) was the most significant factor in the postoperative findings (p = 0.013; Table 5).
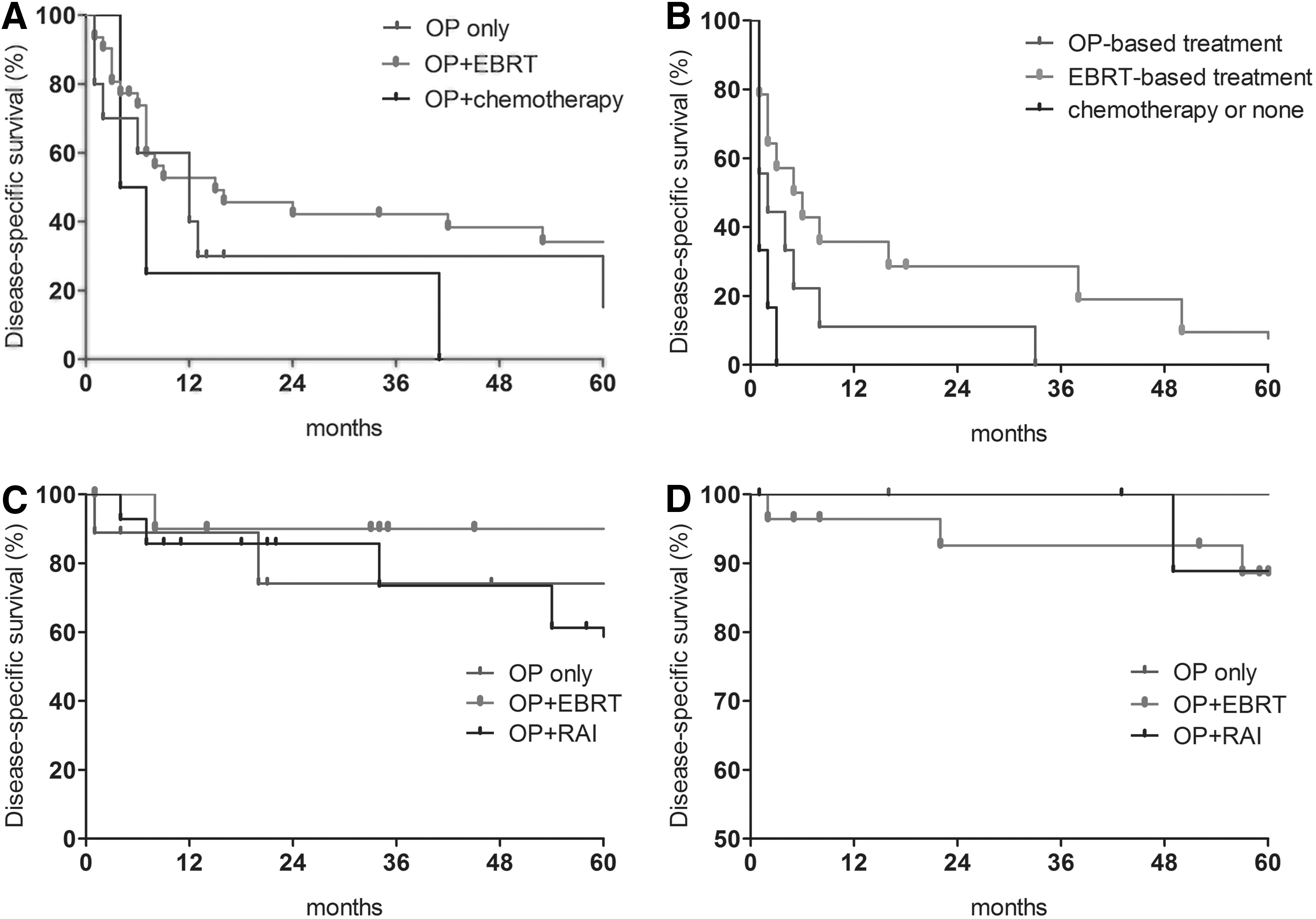
Disease-specific survival according to the treatment modalities applied: (
Adjusted with age, sex, WBC count, and staging in ATC, and adjusted with age, sex, and staging in PDTC and DTC with anaplastic foci.
HR, hazard ratio; CI, confidence interval.
Statistical significance was defined as p < 0.005 (bold).
Cox regression analysis with characteristics entry to the cohort.
Model 1: Resectability was adjusted with age, tumor size, WBC count, and N staging.
Model 2: Preoperative imaging findings were adjusted with age, tumor size, WBC count, and N staging.
Model 3: Postoperative pathologic findings were adjusted with age, tumor size, WBC count, and N staging.
Statistical significance was defined as p < 0.005 (bold).
Survival outcomes according to treatment methods in PDTC
The one- and two-year survival rate was 87.9% and 84.3%, respectively, in patients with PDTC (median survival was 54.9 months; Table 2). Adjuvant treatment after surgery showed increased disease-specific survival (OP only [n = 9], 77.8%; OP + EBRT [n = 11), 90.0%; OP + RAI [n = 14], 57.1%), although this did not reach statistical significance (p = 0.236; Fig. 2C, Table 4, and Supplementary Table S2). Survival difference between OP + EBRT and OP + RAI also showed no statistical difference (p = 0.104). Age (OR = 1.07 [CI 1.02–1.13]) and resectability (unresectable tumor, OR = 8.32 [CI 2.21–31.35]) were the significant prognostic factors for survival in univariate analysis (p = 0.012 and 0.002, respectively). Multivariate analysis revealed that resectability was the only significant prognosticator (unresectable tumor, OR = 11.40 [CI 2.65–49.10], p = 0.001; Supplementary Table S3).
Survival outcomes according to treatment methods in DTC with anaplastic foci
The one- and two-year survival rates were 97.7% and 95.3%, respectively, for DTC with anaplastic foci (with a median survival of 71.8 months; Table 2). Adjuvant treatment after surgery also showed increased disease-specific survival (OP only [n = 6], 50.0%; OP + EBRT [n = 28), 89.3%; OP + RAI [n = 12], 91.7%) but without statistical significance (p = 0.771; Fig. 2D, Table 4, and Supplementary Table S2). In univariate analysis, the significant factors of prognosis were age (OR = 1.12 [CI 1.01–1.24]), sex (OR = 6.63 [CI 1.28–34.41]), and tracheal invasion (OR = 12.04 [CI 1.25–115.85], p = 0.029, 0.024, and 0.031, respectively; Supplementary Table S4).
Discussion
This study demonstrates that the incidence of DTC with anaplastic foci has increased, while the relative incidence of ATC has gradually decreased over time. The relative incidence of PDTC has remained about the same over the study period. Although ATC and PDTC are known to be different disease entities, both have shown locoregional aggressiveness and have resulted in poorer survival outcomes. In ATC, resectability of the cancer, including those tumors with tracheal invasion, showed the best predictability for survival at pre- and intraoperative evaluation; and lymphatic invasion was the best predictive factor after surgery. Interestingly, EBRT showed some beneficial effects on survival of ATC in both resectable and unresectable tumors, suggesting the possibility of an important role of EBRT in treating ATC.
The incidence of thyroid cancer has been increasing, partly due to improved diagnostic techniques such as ultrasonography. In particular, in 2005, the incidence of papillary thyroid cancer abruptly rose, mainly due to the increasing detection of cases in Korea by health checkup examination (12 –14). When comparing the clinical characteristics of ATC or PDTC in the present study with those of the previous report on DTC (15), age at diagnosis and the proportion of male patients were found to be higher in tumors with aggressive pathology in the present study. Time trends showed that the number of cases in all three diagnostic groups, as well as the number of surgical cases with resectable tumors, have increased, while cases with a previous history of goiter and stage T4b tumors have decreased. Among the three groups, the increment was obvious in DTC with anaplastic foci, in accordance with increasing cases of DTC. Overall, these data regarding trends over time may result partially from the earlier detection of thyroid cancer, thus showing increasing detection of tumors at an early stage of anaplastic transformation in DTC (i.e., small and resectable tumors). Moreover, the increment in absolute numbers in all groups may be a true increment, although this could not be determined based just on data from a single institute.
However, the definition of the categories of DTC with anaplastic foci is still unclear. Treatment of those cases of DTC with a small focus of an anaplastic component has been reported to influence the prognosis of DTC negatively (16). Nevertheless, such cancers showed a better long-term survival rate than ATC (7). However, the criteria for the definition of anaplastic foci have not been clearly established, and a previous report of DTC with anaplastic foci did not show the percentage of anaplastic foci used in their criteria (7,16). In the present study, we defined the cutoff point of contained anaplastic component to distinguish DTC with anaplastic foci from ATC arising from DTC as 10%. However, all cases of ATC arising from DTC were composed of >50% of anaplastic component in this study. Therefore, further research is needed to define the criteria by elucidating the relation between the proportion of anaplastic component of tumors and their prognosis.
ATC arising from DTC was defined as a tumor in which >10% of its volume was occupied by undifferentiated cells, while DTC with anaplastic foci was defined as a tumor in which <10% of the tumor volume was occupied by undifferentiated cells in the background of differentiated cancer. Interestingly, in PDTC, a slightly poorer survival was evident in the five-year survival rates, and it continuously decreased faster than that of DTC with anaplastic foci (Fig. 1). A few previous studies have also reported similar five-year survival rates of approximately 50–60% in PDTC (17,18). Therefore, it should be kept in mind that PDTC might progress after long-term follow-up, while the prognosis of DTC with anaplastic foci in complete remission status could remain excellent.
Orita et al. reported that survival of ATC was higher in patients who were diagnosed between 1999 and 2009 compared with those diagnosed between 1976 and 1999 (19). Han et al. also reported on the time trend of ATC, noting an increased number of small tumors and improved survival outcomes (7). In this study, although a previous history of goiter in ATC patients was less prevalent, there were still a significant number of cases of unresectable tumors with cervical lymph node or distant metastases. Thus, this trend may indicate that the early detection of thyroid cancer might only benefit patients with PDTC and DTC with anaplastic foci.
In both PDTC and DTC with anaplastic foci, resectibility was also the most significant prognosticator, and most resectable tumors could be treated with curative-intended surgery as a first-line treatment. Most cases of DTC with anaplastic foci have been found incidentally after surgical resection of a predominantly non-anaplastic tumor (20 –22). In this study, most (i.e., 72.9%) cases of DTC with anaplastic foci were also detected during a routine thyroid health checkup, so most (95.8%) of the tumors were resectable, and patients thereby underwent surgery as a first-line treatment. Therefore, knowing the efficacy of adjuvant EBRT after surgery could be very important. Whether these tumors necessitate adjuvant EBRT or whether they could be treated similarly to DTC remains controversial, and there is unfortunately no meaningful data to define the best approach. The data presented here suggest that adjuvant EBRT as well as RAI might improve survival rates in PDTC and DTC with anaplastic foci, although there was no statistical significance. Considering the small number of patients in this study, the results, however, remain inconclusive.
In ATC, resectability is a well-known prognosticator of the decision to perform surgery (1,3,20,23 –27). Currently, radical surgery and additional multimodality therapy is deemed to be the best treatment protocol for resectable tumors (28 –33). In addition, an R0/R1 resection is reported to correlate with better survival outcomes (34,35). In the present study, patients with fatal outcomes due to ATC and PDTC showed a higher prevalence of unresectable tumors, carotid incasement, prevertebral space invasion, tracheal invasion, and esophageal invasion, although statistical significance was attained mainly for resectability and tracheal invasion. Therefore, surgeons should be aware of their own surgical expertise and thoroughly evaluate the possibility of resectability with preoperative imaging studies. An improvement in the quality of images over the study period partly affected decision making in regard to resectability. However, a positive resection margin in resectable tumors was found to be stable with 14.2%, 8.3%, and 19.7% of cases during the study period (Table 1). Therefore, the interpretation of past and current imaging studies regarding resectability did not differ substantially over time.
This study demonstrated that EBRT on unresectable tumors was beneficial in terms of disease-specific survival rate and median survival duration. However, its efficacy could not be determined because of limited number of subjects in this study. Others reported that higher doses of EBRT do not always improve response rate or survival (36). Nevertheless, EBRT sometimes renders an unresectable tumor potentially resectable, potentially resulting in an increase in survival (9,21,37). Therefore, primary EBRT on unresectable tumors might improve survival in ATC, but this aspect requires further investigation.
Several studies have suggested that the prognostic factors for ATC include age, acute symptoms, leukocytosis, size, T category, and M category (7,38 –40). The novel finding presented here is that lymphatic invasion is the most significant factor affecting long-term survival of ATC. Although postoperative treatment is not expected to be modified on the basis of lymphatic invasion, it could be used as a basis for stratification. Moreover, a more thorough examination of locoregional and distant recurrence of the patients with lymphatic invasion may be needed during follow-up.
In this study, survival duration appeared to be longer than in previous studies. However, one recent study of ATC patients (25) showed survival data comparable with this study, suggesting improvement of survival in the last two decades. Moreover, in cases that were lost to follow-up without knowing the survival status, data regarding the date and cause of death in the present study were obtained from the National Statistical Office. Thus, the survival data are relatively accurate. There could have been some cases that were not diagnosed as ATC because of undifferentiated histology and advanced extent. Thus, very aggressive tumors could have been excluded from the present study. Moreover, mean tumor size in this study seemed smaller than in other studies, which might have resulted from earlier detection and resulted in better survival outcomes.
This study has some limitations. For example, this is a retrospective analysis in which an inappropriate diagnosis and categorization of patients diagnosed by fine-needle aspiration (FNA) or incisional biopsy may have occurred. Indeed, among PDTC cases, the pathology review revealed that the diagnosis for 22.7% (5/22) of cases had been changed. A lack of accuracy of results using FNA or incisional biopsy in early cohorts may have biased the result. In addition, a possible limitation could consist in discrepancies concerning what constitutes a resectable tumor among physicians who retrospectively performed analyses and who actually decided treatment plans and performed the surgery. Moreover, diagnostic categorization was arbitrary, especially in regards to the use of 10% of undifferentiated cells to separate DTC from ATC. In addition, the lack of a standard treatment protocol could bias the findings. However, this study is one of the largest cohorts by far from a single institution, thereby minimizing other confounding factors. To the best of the authors' knowledge, this study is the first to compare the clinicopathological characteristics and survival outcomes of various aggressive pathologic entities of thyroid cancer and their temporal trends. By inspecting the time trends and comparing the treatment outcomes according to the histopathologic categorization, this study is potentially valuable.
In conclusion, the incidence of DTC with anaplastic foci has increased and the incidence of ATA has decreased over time. DTC with anaplastic foci and PDTC show a better survival than ATC. Resectability is the most significant prognostic factor in preoperative findings, while lymphatic invasion is the most significant postoperative prognosticator in ATC. In ATC, because surgery with additional EBRT showed longer survival than surgery alone in resectable tumors, adjuvant EBRT should be applied. In contrast, EBRT-based therapy may be of benefit for unresectable tumors and applied without surgical treatment. In PDTC and DTC with anaplastic foci, adjuvant EBRT or RAI seems to confer survival gain. Although further research is needed to elucidate the role of adjuvant therapy, the choice of treatment of ATC and PDTC could be modified according to the stratification by perioperative parameters including resectability and lymphatic invasion of the cancer.
Footnotes
Acknowledgments
This study was supported by the Research Grant Number CB-2011-03-01 of the Korean Foundation for Cancer Research. This article was presented in 84th annual meeting of American Thyroid Association, Coronado, CA.
Author Disclosure Statement
The authors have nothing to disclose.