
Abstract
Purpose:
The aim of this study was to evaluate the relationship between lymph node yield (LNY) from central (CND) and lateral (LND) neck dissections and risk of recurrence in patients undergoing primary surgery for well-differentiated papillary thyroid carcinoma (WDPTC).
Methods:
Clinical data were reviewed from all patients with biopsy-proven WDPTC who underwent primary total thyroidectomy with CND or LND at the authors' institution from 2005 to 2009. Patient demographics and tumor characteristics were obtained, and clinical data with at least five-year follow-up were used. Within the CNDs and LNDs, total number of nodes removed (LNY), total positive nodes removed, and the ratio of positive lymph nodes to LNY were determined.
Results:
One hundred fifty-two patients were included in the study, with average follow-up of 69 months. Of 125 patients who underwent CND, 20 had central neck disease recurrence. The LNY of patients with central neck recurrence was significantly less than those who had no recurrence (2.5 vs. 10.3; p < 0.0001). Of 71 patients who underwent LND, 23 had ipsilateral lateral neck disease recurrence. The LNY of patients with lateral neck recurrence was significantly less than those who did not recur (10.5 vs. 24.6; p < 0.0001). Higher rates of recurrence were associated with smaller LNY in both groups. For both groups, lower LNY remains predictive of recurrence on multivariate analysis controlling for pT stage, pN stage, American Joint Committee on Cancer stage, and radioactive iodine treatment.
Conclusions:
Higher LNY in CNDs and LNDs is associated with lower rates of papillary thyroid carcinoma recurrence in the central and lateral neck. To minimize the risk of recurrence and the need for secondary therapy with revision surgery and/or radiation, surgeons should perform thorough, compartment-oriented CNDs and LNDs when nodal surgery is undertaken.
Introduction
W
Methods
Approval for this study was obtained from the University of California–San Francisco Institutional Review Board. Study subjects were identified from a cancer registry database. Patient data were extracted from clinic visit notes, radiology reports, pathology reports, and operative reports in the electronic medical record system.
All patients with a diagnosis of WDPTC who underwent primary therapeutic CND or LND with follow-up data at least 60 months after surgery from January 2005 to December 2009 were included. Neck dissection was performed for suspicious lymph nodes on preoperative ultrasound imaging, pathologically positive nodes on fine-needle aspiration (FNA) biopsy, or clinically positive nodes on intraoperative exam at the time of total thyroidectomy. Suspicious lymph nodes on preoperative ultrasound imaging were defined by: (i) lymph node growth on serial imaging, (ii) size >1 cm, (iii) rounded shape, (iv) hypoechoic and/or cystic echotexture with loss of a fatty hilum, or (v) presence of microcalcifications.
Conventional CND includes removal of unilateral or, when specified, bilateral, paratracheal, pretracheal, and prelaryngeal lymph nodes, anatomically defined as the level VI lymph node basin. Complete or modified radical LND includes removal of nodes deep to the sternocleidomastoid muscle superiorly from the skull base down to the clavicle, anatomically defined as level II, III, IV, and V lymph node basins (with sub-compartments IIA and VB of significant consideration in thyroid cancer). Surgeries were performed by surgeons from both the Department of Otolaryngology—Head and Neck Surgery and the Department of Surgery, and data were pooled. Patients were classified based upon the operative report notes written by the individual surgeon as “central neck dissection” and/or “lateral neck dissection.” The LNY for the central neck was analyzed in terms of the entire central compartment (right, left, or both), as the pretracheal and prelaryngeal components of the central neck are overlapping parts of unilateral CNDs. The precise levels included in the surgeries were not always described.
Patient demographics and tumor characteristics were recorded. Pathology reports were reviewed for number of lymph nodes removed (i.e., LNY) in the CND and LND specimens. The number of positive lymph nodes was also recorded, and a ratio of positive lymph nodes to LNY was calculated (lymph node ratio [LNR]).
Recurrent disease was defined after pathologic confirmation of disease within lymph nodes on FNA biopsy or after secondary lymphadenectomy. Patients without cytologic or histologically proven thyroid cancer recurrence but with abnormalities on surveillance ultrasound or elevated serum thyroglobulin levels were not categorized to have recurrent disease.
Groups with and without recurrent PTC were compared using the Mann–Whitney test and Pearson correlation tests. Pearson partial correlation testing controlled for patient variables and tumor characteristics between the two groups, and analysis of covariance was used to obtain means. Kaplan–Meier curves were created for time to recurrence. Logistic regression models for recurrence were performed to assess the relationship of LNY with recurrence, controlling for differences in patient and tumor characteristics. Data analysis was performed using SAS (SAS Institute, Cary, NC).
Results
One hundred fifty-two patients met inclusion criteria, including 105 women, with an age range of 17–83 years (M = 44.2, standard deviation [SD] = 15.7; median = 41). Average follow-up was 69 months (SD = 19; median = 68). A total of 125 CNDs and 71 LNDs were performed. Forty-three patients were diagnosed with PTC recurrence. At the time of last follow-up, treatment for recurrence in 16 patients was still pending. One hundred forty-five patients were alive at last follow-up, and thyroid cancer was not the cause of death in any patient during this study period. Advanced T-stage was associated with both central (p < 0.05) and lateral neck recurrence (p < 0.005). Sex and age at diagnosis were not associated with elevated central and lateral neck recurrence rates (Table 1).
Statistical significance.
AJCC, American Joint Committee on Cancer; EBT, external beam therapy; RAI, radioactive iodine.
CND LNY is associated with disease recurrence
CND was performed in 125 patients, with LNY ranging from 1 to 27 nodes. Average LNY in patients without central neck recurrence (n = 105) was 10.3 compared with an average LNY of 2.5 in the patients with central neck recurrence (n = 20).
Eighty-six (68.8%) patients had at least one positive lymph node on surgical pathology, 55 (63.9%) of whom received postoperative radiation (131I), and 13 (15.1%) developed a central neck recurrence. Thirty-nine (31.2%) patients had no evidence of metastatic thyroid carcinoma in the neck dissection specimen, although clinical decision for performing neck dissection was based on suspicious findings on imaging or cytology, or intraoperative assessment of enlarged lymph nodes. Fifteen (38.4%) patients without nodal metastasis received postoperative 131I based on characteristics of the primary tumor. Despite the lack of metastatic disease on pathologic analysis, seven (17.9%) patients were diagnosed with central neck recurrence.
Central neck LNY was significantly lower in the recurrence group compared with the no-recurrence group (p < 0.001; Fig. 1). The difference between cohorts with and without recurrence remained significant, even after excluding patients with pN0 disease found on final pathology from the analysis (p < 0.0001), and when controlling for pT stage and TNM stage (p < 0.0001, Table 2). Multivariate analysis confirms that higher central neck LNY is associated with lower recurrence rates when controlling for pT stage, pN stage, American Joint Committee on Cancer (AJCC) staging, and 131I treatment (p < 0.001; odds ratio [OR] = 0.47).
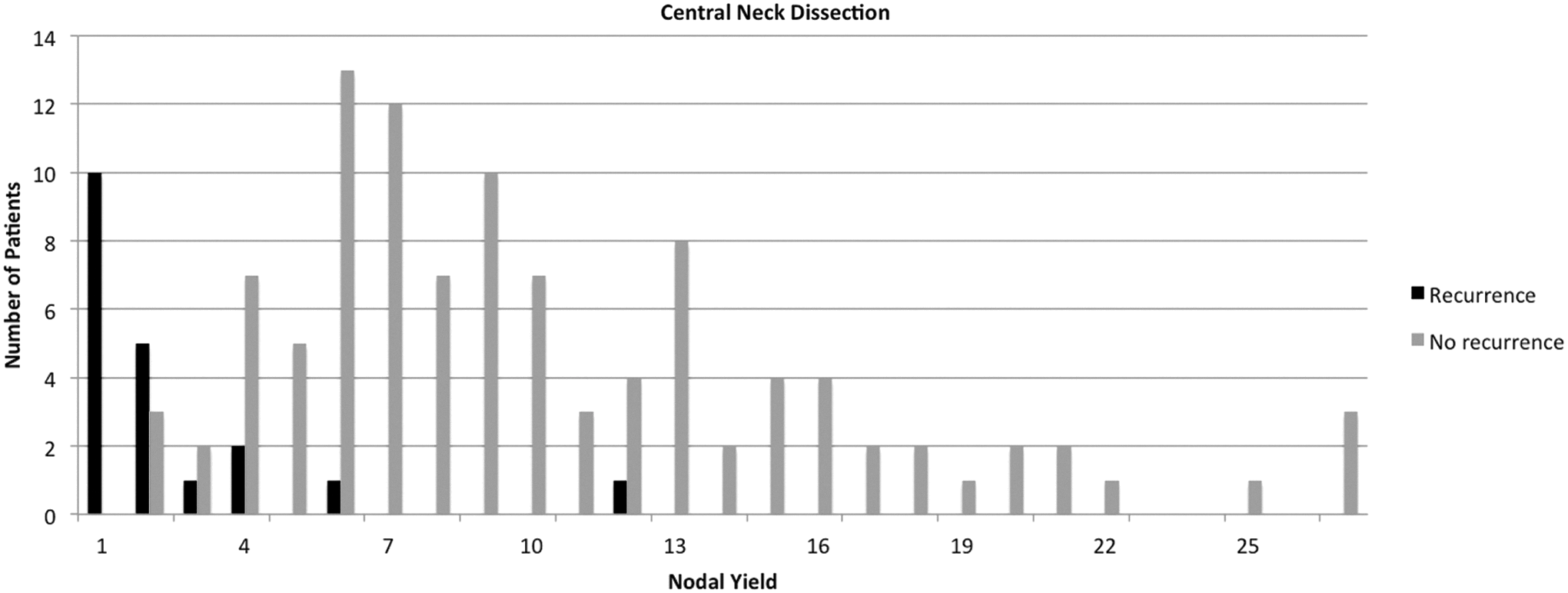
Central neck dissection (CND) low lymph node yield (LNY) is associated with disease recurrence.
CND, central neck dissection; LND, lateral neck dissection; LNR, lymph node ratio; LNY, lymph node yield.
Twenty patients were diagnosed with ipsilateral central neck recurrence on biopsy or imaging, and underwent additional surgery. The mean time to diagnosis of central neck recurrence was 23 months. Sixteen (80%) patients with recurrence had undergone radioactive iodine ablation with 131I after their initial surgery. After secondary surgery, 15 (75%) patients underwent 131I therapy, 12 of whom received a second course of 131I and three received their first dose of 131I.
The difference between the number of positive nodes in the pathology specimen from the original surgery in the two groups was not significant (3.6 for no-recurrence group and 1.5 for recurrence group; p > 0.05). However, the LNR (defined as pathologically positive nodes divided by LNY) was significantly different between the two groups (0.35 for non-recurrence group and 0.58 for recurrence group; p < 0.05; Table 2).
Central neck LNY was separated into three groups (group 1: 1–4 nodes; group 2: 5–8 nodes; group 3: 9+ nodes). Kaplan–Meier curves for recurrence by number of central nodes dissected shows that the rate of recurrence is associated with lower LNY (p < 0.001; Fig. 2). There was no difference in time to recurrence between the three groups (1–4 nodes: M = 21.3 months; 5–8 nodes: M = 47 months; 9+ nodes: M = 29 months; p > 0.05).
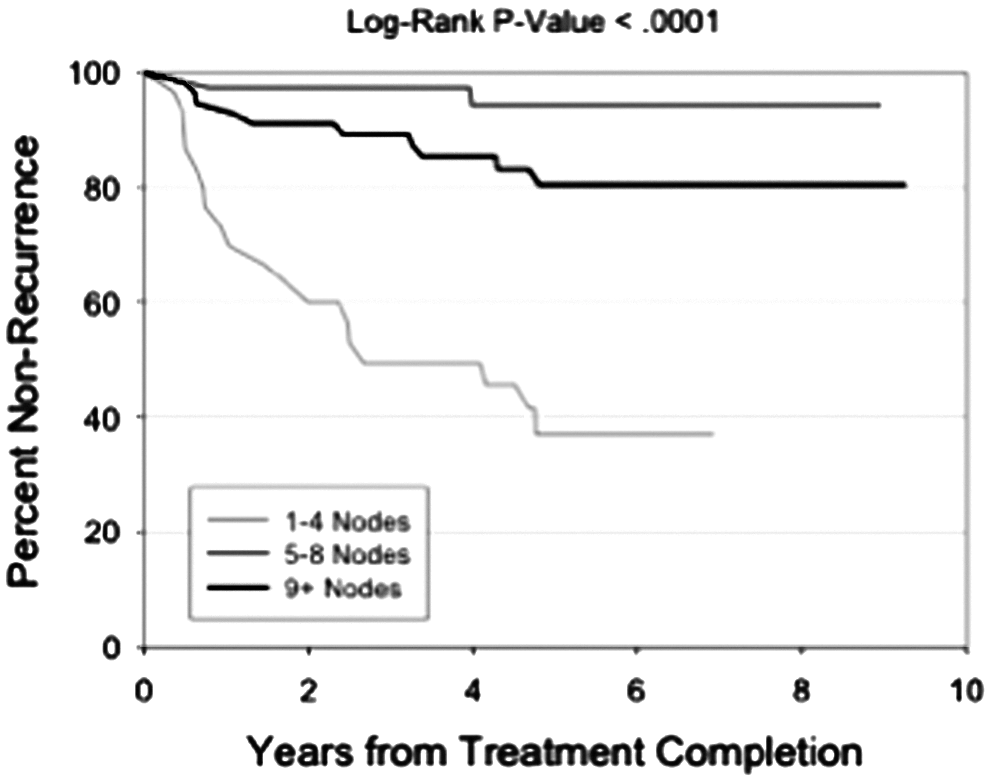
Rate of recurrence is associated with CND LNY.
The LNY for the central neck was analyzed in terms of the overall central compartment because the pretracheal and prelaryngeal components of the central neck are overlapping parts of both right and left unilateral CNDs. It would not be expected that a bilateral CND would yield twice as many nodes as a unilateral CND, since the pretracheal and prelaryngeal nodes are included in either right or left unilateral CND alone. The entire central neck compartment was analyzed, understanding that many patients would have undergone only a unilateral CND, and their node counts would influence the overall results.
LND LNY is associated with disease recurrence
Unilateral LND surgery was performed in 71 patients. LNY ranged from 2 to 46 nodes. Forty-eight patients without lateral neck disease recurrence had an average LNY of 24.6 compared with 23 patients with lateral neck disease recurrence with an average LNY of 10.5.
Sixty-three (88.7%) patients had at least one positive lymph node on surgical pathology of whom 36 (57.1%) received postoperative 131I treatment, and 23 (36.5%) developed a lateral neck recurrence. Eight (11.3%) patients had no evidence of metastatic disease in the LND specimen, in spite of the fact that four of these patients had preoperative FNA biopsy showing PTC, and four had ultrasound findings suggestive of lateral neck disease. Of these eight patients, three (37.5%) received postoperative 131I therapy. None of the patients with negative pathology developed a lateral neck recurrence, suggesting that either preoperative FNA or ultrasound was misinterpreted, surgical pathology missed the presence of metastatic disease, or postoperative 131I therapy successfully ablated disease.
Lateral neck LNY was significantly lower in the recurrence group compared with the no-recurrence group (p < 0.001; Fig. 3). The difference between groups remained significant even after patients with pN0 disease based on final pathology were excluded from the analysis (p < 0.0001), and after controlling for pT stage and TNM stage (p < 0.0001). Multivariate analysis confirms that higher lateral neck LNY is associated with lower recurrence rates when controlling for pT stage, pN stage, AJCC staging, and 131I treatment (p = 0.0004; OR = 0.72).
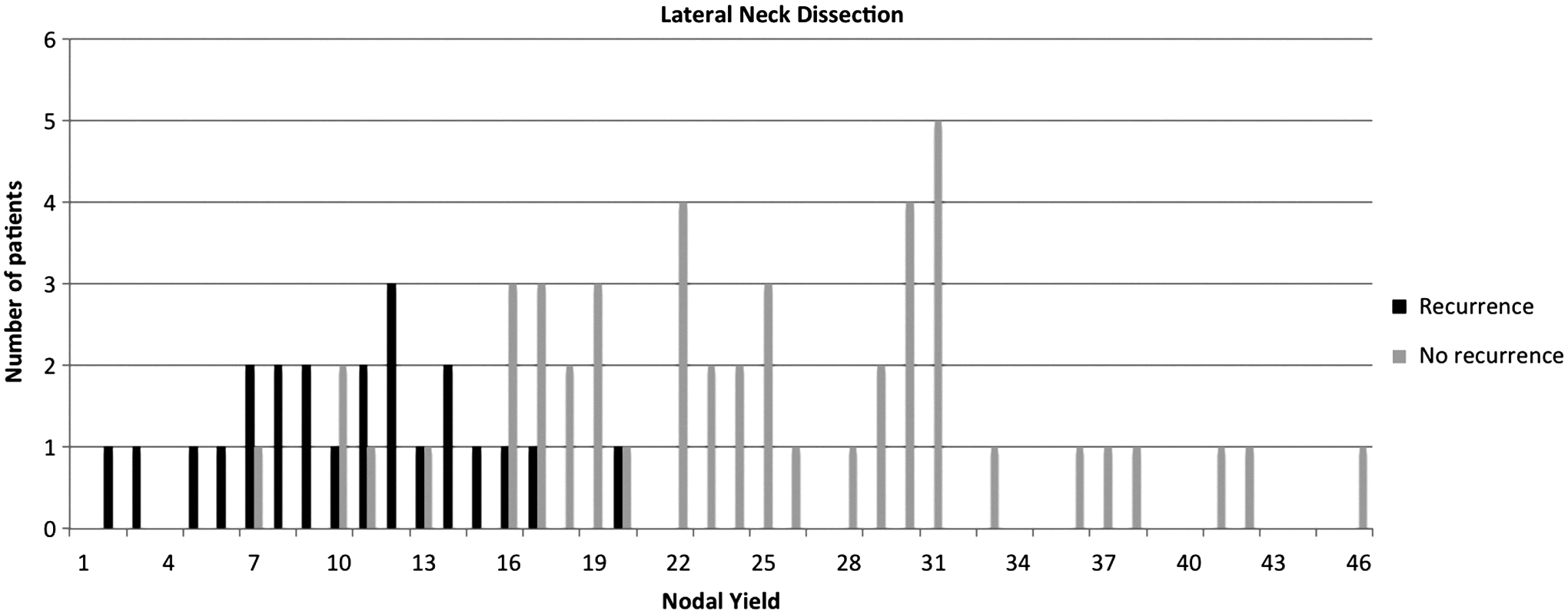
Lateral neck dissection (LND) low LNY is associated with disease recurrence.
Twenty-three patients were diagnosed with ipsilateral lateral neck PTC recurrence on biopsy or imaging, and underwent additional surgery. The mean time to diagnosis of lateral neck recurrence was 22.7 months (median = 13 months). All patients with recurrence underwent additional surgery. Seventeen (73.9%) patients with recurrence had undergone 131I therapy after their initial surgery. Nineteen (82.6%) patients were treated with 131I after secondary revision surgery (15 patients received a second course of 131I, and four their first). There was no significant difference in the number of positive nodes found at the original surgery between the two groups (4.5 for no-recurrence group and 4.7 for recurrence group; p > 0.05). However, the LNR was significantly different between the two groups (0.19 for the non-recurrence group and 0.49 for the recurrence group; p < 0.0001).
Lateral neck LNY was divided into three groups (group 1: 1–9 nodes; group 2: 10–19 nodes; group 3: 20+ nodes). Kaplan–Meier curves for recurrence by number of lateral nodes removed demonstrates that the rate of disease recurrence is associated with lower LNY (p < 0.0001; Fig. 4). There was no difference in time to recurrence between the three groups (1–9 nodes: M = 19.8 months; 10–19 nodes: M = 26.6 months; 20+ nodes: M = 5 months; p > 0.05).
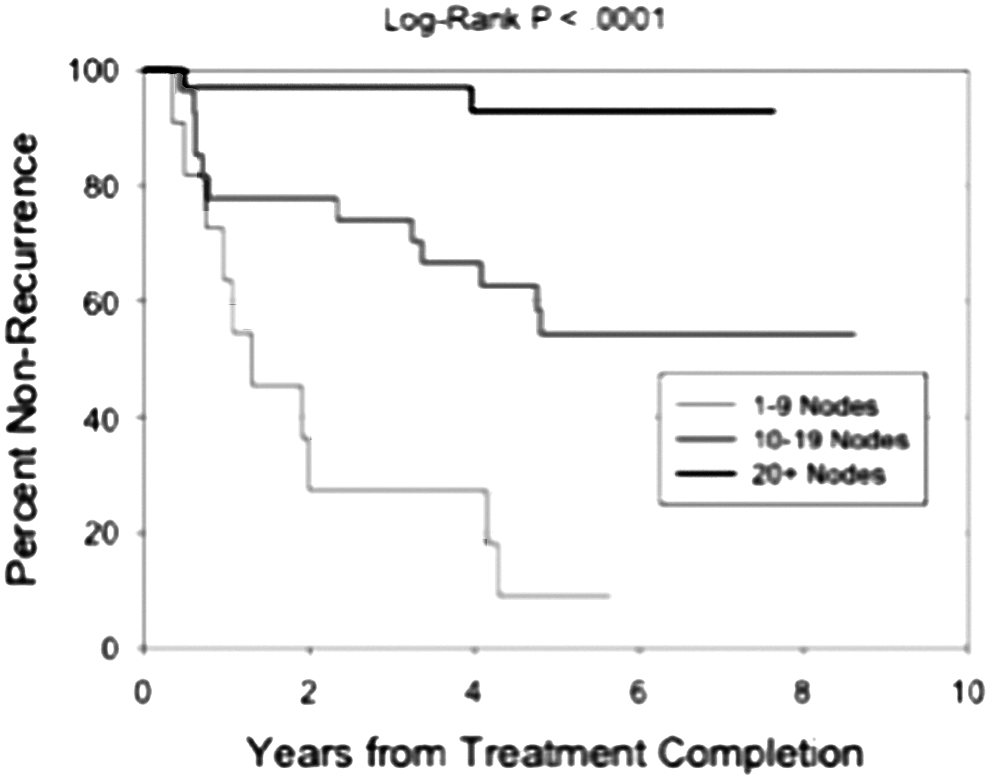
Rate of recurrence is associated with LND LNY.
Potential LNY goal in CNDs and LNDs
Examination of the probability of recurrence versus LNY reveals that an odds ratio of zero is associated with removal of at least 12 nodes in a CND and 22 nodes in a LND (Fig. 5). LNY of a minimum of six in a CND and a minimum of 16 in a LND were both associated with very low recurrence rates.
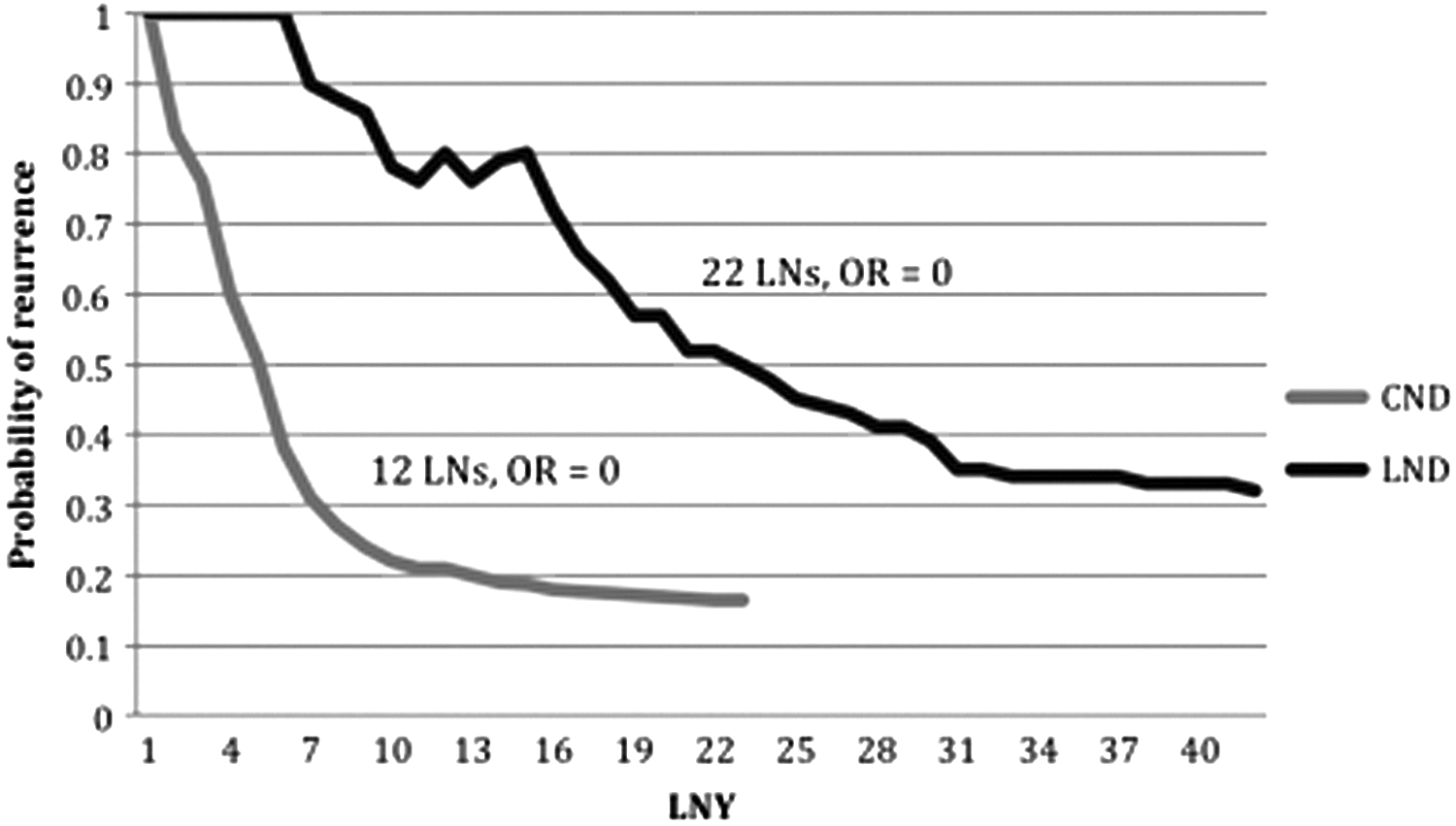
Probability of recurrence based on LNY; the number of lymph nodes dissected corresponding to an odds ratio of zero is depicted.
Discussion
WDPTC can metastasize to lymph nodes in the central and lateral neck. While there is no strong evidence that regional metastases have a substantial effect on overall survival, lymph node metastases are associated with an increased risk of locoregional recurrence (6,7). Management of recurrence often requires additional surgery, radioiodine therapy, or radiation, which incurs additional risks to patients. With revision central and lateral neck surgery, scarring from prior surgical dissection makes visualization and identification of parathyroid glands, the recurrent laryngeal nerves, and other cranial nerves more difficult, placing patients at higher risk for injury. Repeat 131I radioiodine therapy used in cases of advanced disease is associated with increased severity of radiation-induced sequelae, including xerostomia, sialadenitis, dacryocystitis, and increased risk of secondary malignancies. Disease recurrence is also associated with significant psychological burden. Therefore, this study aimed to determine if more complete lymph node removal at primary surgery decreases the need for revision surgery.
Analysis of patients who underwent primary CND or LND for WDPTC demonstrates that LNYs from neck dissection specimens are significantly lower in the group with recurrence compared with the group without recurrent disease. The association between LNY and recurrence remains statistically significant when controlling for both patient and tumor characteristics. Lower LNY also correlated with treatment with additional radioiodine therapy.
The importance of lymph node metastases and LNY in regional dissections for non-head and neck cancers has been studied. The number of lymph nodes removed has been shown to be an independent predictor of overall survival and cancer-specific survival in some colorectal and thoracic malignancies (8,9). Within the head and neck, in the context of elective neck dissection for oral-cavity squamous-cell carcinoma, nodal yield is an independent prognostic factor affecting disease-free survival, disease-specific survival, and overall survival (10). In thyroid malignancies, increasing LNY in patients undergoing nodal dissection for medullary thyroid cancer correlated with improved survival (11). The prognostic value of LNY for WDPTC has remained less clear due to high overall survival rates, even with lymph node metastases. For this very reason, the recommended extent of lymphadenectomy for metastatic PTC remains debated. With regards to survival, Beal et al. (12) noted increasing LNY was associated with decreased survival in PTC. This was believed to be due to an increased likelihood of finding metastatic nodes and, in essence, revealing more advanced disease with more thorough lymph node dissection. However, association with recurrence was not evaluated, and the study concluded that nodal understaging is inconsequential to survival in this patient population (12). A study by Pereira et al. showed no central neck recurrence but the highest risk of recurrence in the lateral neck in patients in whom six or more nodes were positive in the CND (13).
Others have examined the prognostic significance of LNR as an adjunct to LNY in WDPTC. With regards to disease-free survival, patients with a higher ratio have been found to recur more often. Vas Nunes et al. noted that a ratio of ≥0.3 was associated with a recurrence rate 3.4 times higher than for those with a smaller ratio (14). Schneider et al. noted a recurrence OR of 19.5 when the LNR was ≥0.7 (15). Ryu et al. showed that recurrence-free survival approaches 99% if the LNR is ≤0.65 with at least three nodes removed (16).
The LNR also has been shown to predict disease-specific mortality. Though the overall mortality rate for PTC remains low, Schneider et al. showed that the mortality of patients with a ratio ≥0.42 was 1.6% compared with 0.65% for those with a lower ratio (17).
This study is the first to examine the roles of LNY and LNR from both CNDs and LNDs. As it is influenced by disease burden and extent of neck dissection, the focus was on LNY as a potentially more sophisticated measurement. Since it is recognized that disease-specific mortality for this population is low, the focus was on determining the implications of LNY in terms of need for revision lymph node dissection and radioiodine therapy. With the cohort of patients in this study, it was found that a thorough, compartment-oriented nodal dissection is associated with a decreased need for revision neck dissection. To achieve an OR of zero for recurrence, the ideal goal nodal yield in the central neck is a minimum of 12 nodes; in the lateral neck, it is 22 nodes. These numbers are ideals and are based on pooled data. Yet, this may not be feasible or realistic in every patient. Still, this ideal nodal yield supports the practice of complete dissection of lymph node basins by anatomically defined compartments. This has implications for surgical technique and patient counseling. Although a difference in overall survival is unlikely, a patient undergoing more complete, compartment-oriented neck dissection can be reassured that the need for revision surgery will be less likely.
This study examined the relationship of LNY to rate of recurrence with follow-up of at least five years. Among patients who had recurrence, a smaller LNY correlated with a higher rate of recurrence. This may represent persistent macroscopic or microscopic disease that was present at the initial operation but not removed due to a less thorough dissection. While this finding may not affect overall survival, it does result in revision surgery and incurs the risks associated with reoperation.
As seen in other studies, the LNR also correlated with recurrence rates. In the current patient population, higher LNRs were more the result of a small LNY with a few positive metastatic nodes, rather than significant disease burden. It is presumed that if these patients had undergone more thorough neck dissections with a higher LNY, their LNRs would have been lower and their chance of recurrence decreased. Finally, this study also examined the association between LNY and LNR and the decision for further radioiodine therapy. As they do for revision surgery, the results show a significant correlation between low LNY and high LNR and perceived need for further radiation therapy with 131I.
This study is limited by clinical and pathologic confounders. Patients with fewer than five years of clinical follow-up were excluded, so the outcomes for neck dissection at the authors' institution are not known for every patient. It is acknowledged that as a regional academic tertiary care medical center, some patients come for surgery but receive their follow-up care and surveillance in the community, sometimes at great distance from the center. Still, the nature of the referral network suggests that patients who have been treated at the center return to the center for further treatment if they are diagnosed with recurrence and they still live in the region. Potential pathologic confounders include the association of extracapsular extension, size of metastatic deposit, and metastatic lymph node size with disease recurrence. Unfortunately, given the retrospective nature of this study, these histologic details were not reported in every case. Investigation of histologic features would be an important component of a prospective study on this topic. Additionally, it should be noted that it was not always possible to determine whether recurrence was within lymph nodes or within soft tissue, and possibly associated with residual thyroid tissue following incomplete thyroidectomy. Due to inconsistencies in surgeon labeling of surgical specimens, it cannot be confirmed whether all of the intended lymph nodes were actually the lymph nodes retrieved in these neck dissections. Multiple pathologists interpreted surgical specimens over the time period of this study, and it is acknowledged that LNY is dependent on the analyses of the reading pathologist. Clinically, there was a lack of standardization of radioactive iodine administration in the cohort. However, the majority of patients with documented N1a and/or N1b disease received postoperative 131I therapy per practice guidelines for the time period during which the cohort was treated.
Conclusion
This study suggests that LNY is associated with risk of disease recurrence and need for revision surgery in WDPTC. To mitigate the risk of recurrence and the inherent risks of revision surgery when treating lymph node metastases in the central or lateral neck from PTC, thorough, compartment-oriented neck dissections should be performed.
Footnotes
Acknowledgments
The authors would like to acknowledge Alan Bostrom for his assistance with statistical analysis. This article was presented as Late-Breaking Abstract at the Annual Meeting of the American Thyroid Association, San Diego, CA, October 29–November 2, 2014.
Author Disclosure Statement
The authors have no disclosures.