
Abstract
Background:
Although radioactive iodine (RAI) imaging/therapy is one of the earliest applications of theranostics, there remain a number of unresolved clinical questions as to the optimization of diagnostic techniques/protocols and improvements in patient-specific treatment planning strategies. The objectives of this study were to determine the imaging characteristics and clinical feasibility of 124I positron emission tomography/computed tomography (PET/CT) for the determination of extent of disease and evaluation of RAI kinetics in its physiologic and neoplastic distribution in patients with differentiated thyroid cancer (DTC).
Methods:
The study was designed as a prospective phase II diagnostic trial of patients with confirmed DTC. Following adequate preparation, patients received 2 mCi 124I in liquid form and sequential whole-body PET/CT imaging was performed at five time points (2–4 h, 24 ± 6 h, 48 ± 6 h, 72 ± 6 h, and 96 ± 6 h post-administration). All patients who had 124I imaging subsequently underwent RAI treatment with 131I, with administered activities ranging from 100 to 300 mCi. Post-treatment scans were obtained 5–7 days after RAI treatment. A by-patient and by-lesion analysis of the 124I images was performed and compared with the post-treatment 131I scans as well as F-18 FDG PET/CT images. Quantitative image analysis was also performed to determine the total functional volume (mL), activity per functional volume (μCi/mL), and cumulated activity (μCi/h) for remnants, salivary glands, and nodal metastases.
Results:
Fifteen patients (6 women; M age = 57 years; range 29–91 years) were enrolled into the study. Forty-six distinct lesions were identified in these 15 patients on 124I PET/CT images, with a sensitivity of 92.5%. In addition, 124I identified 22.5% more foci of RAI-avid lesions compared with the planar 131I post-treatment scans. This study demonstrates different kinetic profiles for normal thyroid remnants (peaked at 24 h with mono-exponential clearance), salivary glands (peaked at 4 h with bi-exponential clearance), and metastatic lesions (protracted retention), as well as individual variations in functional volumes and thus cumulated activities.
Conclusions:
124I PET/CT is a valuable clinical imaging tool/agent, both in determining the extent of disease in the setting of metastatic DTC and in the functional volumetric and kinetic evaluation of target lesions.
Introduction
A
Study Design
The study was designed as a prospective phase II diagnostic trial with the objectives to determine the imaging characteristics and clinical feasibility of 124I PET/computed tomography (CT) imaging for determination of extent of disease and evaluation of RAI kinetics in its physiologic and neoplastic distribution in patients with DTC. Patients with confirmed differentiated (both well-differentiated and poorly differentiated) thyroid cancers were studied. Patients who were newly diagnosed, as well as those who had known or suspected recurrent/metastatic disease, were eligible for the trial. The inclusion criteria for the study included a histological confirmation of DTC and a clinical indication for RAI imaging (detection of known or suspected postoperative residual thyroid bed or nodal disease, extent-of-disease evaluation in known recurrent/metastatic disease, suspicious nodule/mass detected by physical exam, imaging study or fine-needle aspiration, recurrent/metastatic disease suspected by elevated thyroglobulin), age ≥18 years, ability and willingness to give written consent, life expectancy >3 months, and Karnofsky performance status ≥70. Pregnant and nursing women and individuals allergic to iodine were excluded from the study. The study was approved by the Institutional Review Board, and was conducted in accordance with institutional investigational new drug (IND)/research guidelines.
Material and Methods
124I sodium iodide
The 124I sodium iodide utilized for this study was obtained from IBA Molecular N.A., Inc. It was provided in a 0.02 N aqueous NaOH solution with a radiochemical purity (RCP) >95% iodide, radiochemical impurity <5% (iodate and diiodate), and a radionuclide purity (RNP) >99.9% at calibration. The chemical purity was determined with Tellurium (Te) <1 μg/mL. The RCP and RNP stabilities were verified for 10 days.
124I imaging protocol
The administered activity for 124I was 2 mCi by oral administration in liquid form. The basic imaging protocol involved a five time-point (2–4 h, 24 ± 6 h, 48 ± 6 h, 72 ± 6 h, and 96 ± 6 h post-administration) whole-body PET/CT imaging schedule. The patients were prepared for RAI imaging/dosimetry either by withholding suppressive thyroxine for an adequate length of time (to achieve a thyrotropin [TSH] level of >50 at the time of imaging) or by administering recombinant human TSH (rhTSH; two consecutive daily doses of 0.9 mg intramuscularly, in the days preceding RAI administration). Two patients in the study cohort were prepared using the rhTSH protocol. These patients underwent 124I imaging after receiving the standard two-day rhTSH injections. They received a second set of rhTSH injections for the 131I treatment. The remaining patients were prepared using the withdrawal protocol. PET/CT scans were performed on a Siemens Biograph Truepoint™ scanner and combined with low-dose CT for attenuation correction and anatomic localization. Scans were obtained from the top of the head to the feet. An acquisition time of 5 min per bed position was used, with iterative 3D reconstruction by four iterations with eight subsets and a Gaussian filter.
131I imaging protocol
All patients who had 124I imaging subsequently underwent RAI treatment with 131I sodium iodide, with administered activities in the range 100–300 mCi. Post-treatment scans were obtained 5–7 days after RAI treatment. Anterior and posterior planar whole-body scans, as well as static antero-posterior and oblique neck images, were acquired.
Image analysis
The localization of 124I in known/suspected lesions, including cervical and remote metastatic sites, was documented. 124I images were compared to post-treatment 131I images. Comparisons were performed on a by-patient and by-lesion basis. All images were reviewed and analyzed by two experienced nuclear medicine physicians. Quantitative image analysis was performed using semiautomatic region of interest (ROI) methodology. The total functional volume (mL), activity per functional volume (μCi/mL), and cumulated activity (μCi/h) for remnants, salivary glands, and nodal metastases were calculated. The 124I images were also compared to F-18 FDG PET/CT images that were acquired prior to RAI treatment in all patients. F-18 FDG PET/CT imaging was performed as part of a comprehensive extent of disease evaluation and not for the purpose of this study per se.
Relative sensitivity determination for 124I PET/CT versus post-treatment planar 131I imaging
Comparative image analysis was performed on a by-patient and by-lesion basis. For the purposes of by lesion analysis, any distinct uptake noted on 124I PET/CT or post-treatment 131I planar images was considered “positive reference.” A positive reference implies presence of a tumor/remnant with RAI uptake. The true positive (TP) and false negative (FN) designations, and the sensitivity calculations for 124I and 131I imaging were performed based on the “positive reference.” The sites of physiologic uptake were carefully identified. A physiologic uptake was not considered as false positive (FP). A true negative (TN) designation was used when both 124I and 131I images were negative. The complete chart for TP, TN, FP, and FN designations are explained in Table 1.
TP, true positive; TN, true negative; FP, false positive; FN, false negative; NED, no evidence of disease; RAI, radioactive iodine; Tg, thyroglobulin.
Results
Fifteen patients (6 women; M age = 57 years; range 29–91 years) were enrolled into the study. All patients underwent 2 mCi diagnostic 124I imaging. All but one patient completed all 5 days of data collection for dosimetry; one patient only completed 2 days of data collection due to personal reasons. Forty-six distinct lesions were identified in 15 patients (11 remnant tissue, 19 metastatic neck nodes, 3 residual neck tumors, 5 metastatic mediastinal/hilar nodes, 5 metastatic lung disease [diffuse micro- or macronodular uptake], and 3 metastatic abdominal tumors). The 46 distinct lesions are the aggregate sum of all the imaging modalities. This number also includes the lesions identified on FDG PET/CT. By virtue of image detail on 124I images, the thyroid remnant was further divided into ROIs, including the right and left remnant lobes as well as the pyramidal lobe. These were not separately identified on the post-treatment 131I scans. FDG PET/CT was clinically indicated and performed in all 15 patients. Therefore, 124I PET/CT to FDG PET/CT image comparison was possible in all patients. The FDG(+)/RAI(–) lesions were considered to be functionally dedifferentiated, and were thus stratified as a different biological group, and not considered FN. All patients received therapeutic 131I, with administered activities ranging from 100 to 300 mCi, and underwent post-treatment imaging.
Remnant uptake and kinetics
There were eight patients with thyroid remnants, status post recent total thyroidectomy (RAI-naive). By-patient analysis indicated that remnant uptake was demonstrated in all of these patients on both 124I and 131I imaging studies. A total of 11 distinct foci of remnant uptake were identified. 124I distinctly defined remnant uptake in right lobe, left lobe, and isthmus/pyramidal lobe anatomic sites. 124I was positive in 11/11 (100%). 131I revealed 9/11 (82%) distinct remnant foci. The two missed foci of remnant uptake by 131I were in the trajectory of the pyramidal lobe in the midline. FDG was negative in all remnant tissue, and none of the thyroid remnants was visually detected as a soft-tissue abnormality on CT. The sequential 124I images consistently demonstrated the maximum remnant activity to occur at 24 h. After the peak activity was reached, the clearance was mono-exponential, as shown in Figure 1. The maximum remnant activity ranged from 1.2 to 215.9 μCi, with the total functional remnant volume (the total number of voxels within the remnant ROI) ranging from 1 to 60 mL. The activity per volume of remnant tissue ranged from 0.036 to 11.265 μCi/mL. The total cumulated activity within the remnant ranged from 68 to 12757.3 μCi/h.

The uptake and clearance pattern in thyroid remnants. The time–activity curve shows a peak at 24 hours followed by exponential decay.
Salivary gland uptake and kinetics
Physiologic salivary gland activity was demonstrated in all 15 patients, with the activity reaching a peak at 4 h after radioiodine administration. The salivary gland clearance was bi-exponential, with an average of 81% of the activity being cleared from the salivary glands by 24 h.
Nodal disease uptake and kinetics
There were 19 distinct foci of uptake identified as nodal metastasis. 124I was positive in 16/19 (84%). 131I revealed 9/19 (47%) distinct foci of nodal uptake. The three negative nodes by 124I were also negative by 131I but positive on FDG (iodine-refractory nodal disease). Nodal metastatic disease demonstrated a pattern of uptake that was significantly different from the thyroid remnant or physiologic salivary gland activity. A protracted retention was identified as a characteristic pattern for metastatic nodal disease, as shown in Figure 2.
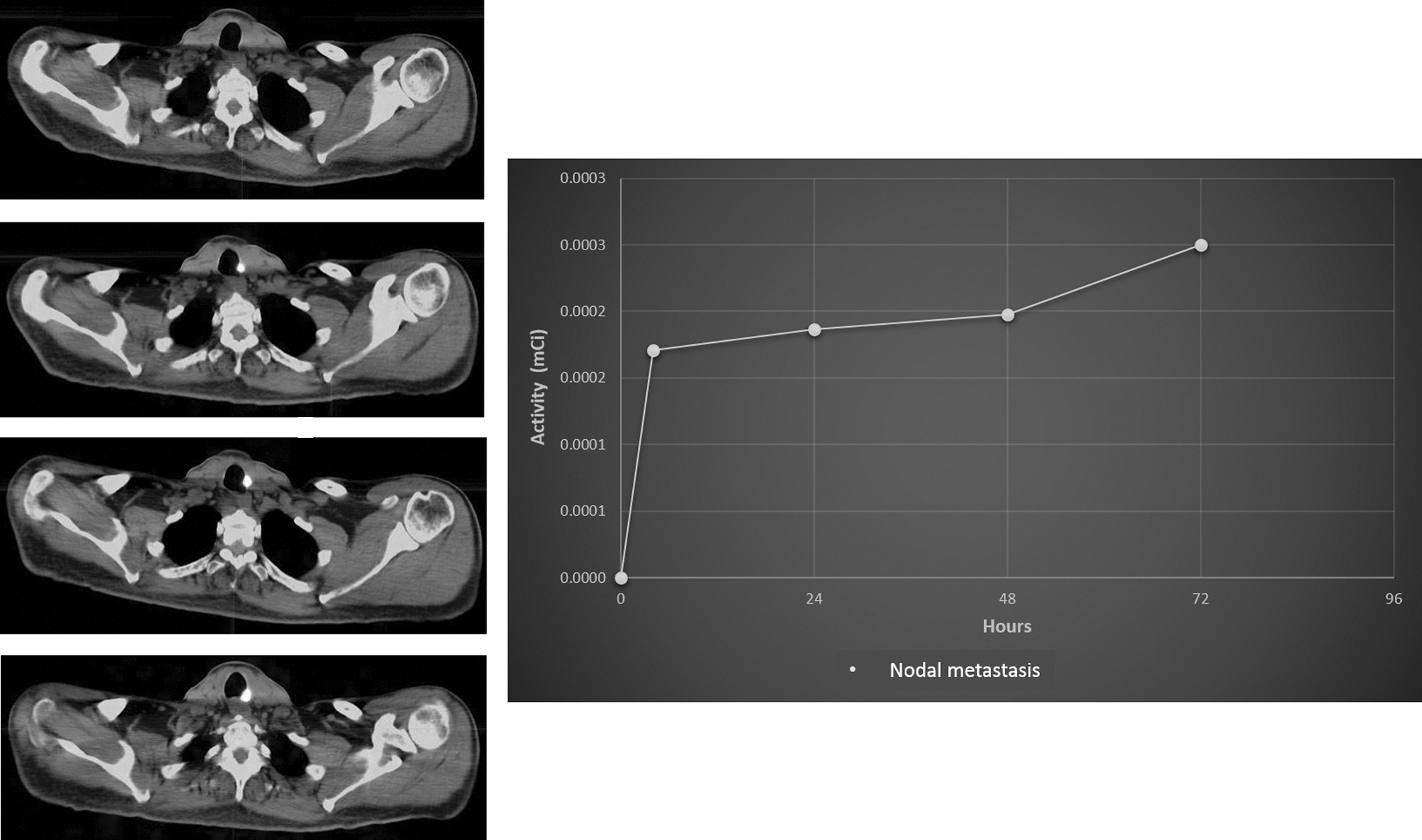
The uptake and clearance pattern in lymph node metastasis. The time–activity curve demonstrates a slow upslope to the peak activity with a protracted retention.
Lung disease
There were five cases of metastatic lung disease (2 micronodular, 3 macronodular). One case was negative on both 124I and 131I, but was positive on FDG (iodine-refractory disease). Of the remaining four cases with metastatic lung disease, 124I was positive in 1/2 cases with macronodular disease, but was negative in 2/2 cases with micronodular metastatic disease. 131I post-treatment scans were positive in 4/4 cases. The case of macronodular disease that was negative on 124I and positive on 131I was also positive on FDG and may be in the process of undergoing dedifferentiation.
Abdominal disease
There was only one patient with abdominal disease. This was a very unusual case that presented with metastatic abdominal disease, and no primary was identified in the total thyroidectomy specimen. The disease was discovered at exploratory laparotomy and confirmed by hematoxylin and eosin and immunohistochemistry (for thyroglobulin and TTF-1 staining). A subsequent FDG study showed hepatic, mesenteric nodal, and peritoneal disease. 124I demonstrated positive uptake in all abdominal lesions. However, 131I was only positive in the hepatic disease.
The comparative uptake patterns of 124I and 131I and the overall sensitivity for respective imaging modalities are presented in Tables 2 and 3.
Discussion
This prospective phase II study demonstrates that 124I PET/CT imaging is clinically feasible, has high lesion detection sensitivity, and offers an additional advantage of quantitation, which can readily be translated into high-quality dosimetric input (activity determination for absorbed dose calculations). This study is unique in that it utilizes post-treatment 131I imaging as the gold standard as opposed to routine diagnostic activities of 131I, which have known limitations in lesion detection.
Van Nostrand et al. compared the ability of diagnostic 124I PET/CT images (1.7 mCi) with 131I planar whole-body imaging (1–2 mCi) in detecting residual thyroid tissue and/or metastatic well-differentiated thyroid cancer. Their data concluded that relative to 131I planar whole-body imaging, 124I PET/CT identified as many as 50% more foci of radioiodine uptake in as many as 32% more patients (23). The present study not only indicates an improved benefit in lesion detectability with 124I PET/CT, but also demonstrates its by lesion detection power (sensitivity) when matched against the gold standard of iodine-avid disease, which is a post-treatment 131I scan after therapeutic doses ranging from 100 to 300 mCi. When using 131I post-treatment scans as the gold standard, 124I PET/CT identified 22.5% more foci of RAI-avid lesions.
The kinetic data derived from the current study demonstrate that normal thyroid remnants, salivary glands, and tumoral lesions (residual cancer tissue and metastatic foci) have different kinetic profiles. Sequential 124I images consistently demonstrated that the maximum activity within the thyroid remnant occurs at 24 hours and, after the peak activity is reached, the clearance is mono-exponential. Physiologic salivary gland activity also demonstrated a dependable kinetic pattern reaching a peak at four hours after radioiodine administration and the clearance is bi-exponential. Nodal metastatic disease demonstrated a pattern of uptake that was significantly different from the thyroid remnant or physiologic salivary gland activity. A protracted retention was identified as a characteristic pattern for metastatic nodal disease.
The notable variation in individual kinetic parameters suggests that dosimetry with 124I PET/CT could enhance the theranostic value that is always emphasized more than the traditional 131I methodology. The decision making and selection of appropriate therapeutic activities of 131I could be more reproducible and accurately determined with 124I. It is well known that 131I has many drawbacks as an imaging agent emitting high-energy 364 keV photons, which are too high for standard nuclear medicine gamma cameras. The low count detection sensitivity resulting from penetration of the crystal and collimator septa by the high-energy photons causes image degradation. These shortcomings of 131I conventional gamma camera imaging are overcome by the improved spatial resolution of coincidence detection in 124I PET/CT. The higher spatial resolution of 124I PET/CT is the basis for improved quantitation. Furthermore, the four-day half-life of 124I allows for time sequence imaging, which is essential for dosimetry applications. The visual image analysis in this study demonstrated that clinically relevant information as to the extent of disease can be obtained within a 72-hour time period. A future detailed dosimetric analysis will finalize a clinically applicable and logistically feasible protocol (not demanding on patient and physician time and resources).
The present data reveal that on a by-patient basis, the mere presence of remnant tissue can be demonstrated on 124I pre-ablation imaging comparable to post-ablation 131I imaging. However, 124I imaging was clearly superior, providing exquisite details in terms of location and laterality of the remnant tissue. High pyramidal lobe remnants were identifiable by 124I, but not by 131I. 124I was also superior in the distinction between nodal versus remnant tissue. Perhaps one of the most important findings obtained was the identification of functional thyroid tissue without an anatomic depiction/appreciation of remnant tissue. In all eight patients who had 124I imaging performed postoperatively, functional thyroid tissue (remnant) was demonstrated with a measurable functional volume. None of these patients had an anatomically definable volume of tissue by CT imaging in the thyroid bed. The functional remnant volume was different for each lobe (side), in addition to the absolute uptake value at 24 hours, as well as the clearance, and thus the cumulated activity. This finding could challenge the recent trend to utilize fixed and low(er) administered activities to ablate the thyroid remnants (24 –26). Obviously, a larger-scale remnant dosimetry study is required to address this concern.
Diagnostic 124I PET/CT imaging failed to demonstrate lung metastases clearly in three patients, two with micronodular disease and one with macronodular disease. All of these cases of lung metastases were detected on the post-treatment 131I scans. The discrepancy in regards to detection of micronodular lung disease may at least in part be explainable by the fractional uptake that could be under the threshold of detectability/visibility, in the individual nodules from an administered activity of 2 mCi 124I. Visibility threshold is defined as adequate activity concentration within a given target volume high enough to be discernable from the background activity. Obviously, the fractional uptake of RAI within a lesion is a function of the NaI symporter (NIS), its expression, and its temporal and spatial functional activity. Taking into consideration the observation of a protracted retention of radioiodine in metastatic lesions and given the process of physical decay, it is possible that these two dynamic processes (in opposing directions) reach the detectability/visibility threshold at different time points. Not only is the administered activity higher for the post-treatment 131I versus diagnostic 124I scans, there is also a 50% difference in physical half-life between the two radiotracers. Therefore, at any reference time point, the relative cumulated activity will be higher with 131I. In addition, it was observed that there is a progressive increase in activity in metastatic lesions over time. It is postulated that the visibility threshold may not be reached with a 2 mCi administered activity of 124I because the point of intersection of the time activity curve for the tumor and the effective half-life curve for 124I might remain under the detection threshold.
In one patient, who was proven to have multiple mesenteric/peritoneal nodules by surgical exploration, the pre-treatment 124I imaging demonstrated intense uptake in all metastatic lesions. These lesions were not seen on post-treatment 131I images (which also included SPECT). In this particular patient, a metastatic liver lesion was seen in both imaging modalities (124I and 131I). This perhaps could also be explained by the temporal and spatial functional activity of NIS, which may vary at different metastatic sites or lesions.
The issue of NIS activity has a pivotal importance in the design of the study as well as the data analysis. The functional dedifferentiation process (in thyroid cancers of follicular cell origin) involves downregulation of NIS, and therefore not all thyroid cancer lesions show similar avidity for RAI (27 –29). For this reason, in a strict sense, a FN designation in a given lesion may not (does not) apply. Similarly, other tissues expressing NIS will be positive on RAI imaging, and a FP designation for those does not apply. The sensitivity of 124I, as a function of lesion size, is best evaluated by comparison to the post-treatment 131I scan, which typically is performed with administered activities >100 mCi. A discordance between the two RAI images (124I and 131I) will indicate a different technical performance of the respective radiopharmaceutical/imaging technology. A discordance between RAI images (124I or 131I) and F-18 FDG, on the other hand, will indicate a different functional profile.
124I imaging is not without potential technical challenges. The physical characteristics of 124I compared with 131I are summarized in Table 4. One important technical consideration as it directly applies to clinical imaging performance is that 124I has a complicated decay schema. First and foremost, 124I is not a pure positron emitter. Thus, a potential factor that may degrade image quality is an aberrant source of “true coincidences.” In addition to positron emission, 124I has prompt gamma-ray emission that can directly fall within the 511-keV energy window, or down-scatter and result in signal detection within this window. The consequence of prompt gamma-ray emission is that they provide an aberrant source of “true coincidences” when one of the two co-linear 511-keV photons is absorbed or otherwise not detected. However, these coincidences contain no information about the origin of the source decay (30,31). The contribution of this aberrant coincidence detection and its relevance to clinical imaging/dosimetry is yet to be determined.
Another potentially important technical consideration is the “spillover effect.” The spillover effect can be defined as an apparent gain in activity for small objects or regions. Although partial volume effect and spillover essentially refer to the same physical phenomenon, it is important to distinguish the outcome of these two different effects. For partial volume effect, the apparent loss of activity in the object is distributed across adjacent voxels, which are considered outside the object, resulting in increased activity in these voxels. This increase in activity is referred to as spillover, whereas loss in activity is referred to as partial volume loss (32). In 124I PET/CT imaging of thyroid remnants and cancers, this effect could be very important. Remnant tissue, having normal thyroid function, has a preserved capacity of RAI uptake. A very small volume, undiscernible by CT, may have significant uptake of RAI. By virtue of the “spillover” effect, the visible PET activity might be overly exaggerated. In contrast to the remnant tissue, a small metastatic deposit with suppressed uptake function may not be appreciated due to partial volume effect.
Conclusion
In conclusion, 124I PET/CT is a valuable clinical imaging tool/agent, in both extent of disease evaluation in the setting of metastatic DTC and in the functional volumetric and kinetic evaluation of target lesions. On a by-lesion and by-patient analysis, 124I clearly demonstrated superior clinical characteristics by identifying 22.5% more foci of RAI-avid lesions with a sensitivity of 92.5% (compared with the gold standard 131I post-treatment scan) and by providing exquisite detail in terms of location and laterality of the remnant thyroid tissue (even when no remnant tissue was appreciated on anatomical imaging). 124I, by virtue of being a PET agent, provides discriminating visual image details, which not only facilitate detection and visualization of disease, but also potentially affords quantitative input for accurate dosimetry. The present study demonstrates different kinetic profiles for normal thyroid remnants, salivary glands, and metastatic lesions, as well as individual variations in functional volumes, and thus cumulated activities, which may have implications for treatment planning. The quantitative power of 124I PET/CT can be optimized by modifying image acquisition settings and creating indication-specific (remnant vs. disease imaging) protocols.
Footnotes
Acknowledgments
This study was supported by the Simpkins Foundation Grant for thyroid cancer research.
Author Disclosure Statement
None of the study authors has competing financial interests in connection with the submitted manuscript.