
Abstract
Background:
MicroSPECT/CT imaging was used to quantitatively evaluate how iodide uptake in the mouse thyroid is influenced by (i) route of iodine administration; (ii) injection of recombinant human thyrotropin (rhTSH); and (iii) low iodide diet (LID) in euthyroid and triiodothyronine (T3)-treated mice.
Methods:
Pertechnetate (99mTcO4 −) and 123I thyroid uptake in euthyroid and T3-treated animals fed either a normal-iodine diet (NID) or an LID, treated or not with rhTSH, and radiotracer administered intravenously, subcutaneously, intraperitoneally or by gavage, were assessed using microSPECT/CT imaging. Western blotting was performed to measure sodium/iodide symporter expression levels in the thyroid.
Results:
Systemic administration of radioiodide resulted in a higher (2.35-fold in NID mice) accumulation of iodide in the thyroid than oral administration. Mice fed LID with systemic radioiodide administration showed a further two-fold increase in thyroid iodide uptake to yield a ∼5-fold increase in uptake compared to the standard NID/oral route. Although rhTSH injections stimulated thyroid activity in both euthyroid and T3-treated mice fed the NID, uptake levels for T3-treated mice remained low compared with those for the euthyroid mice. Combining LID and rhTSH in T3-treated mice resulted in a 2.8-fold higher uptake compared with NID/T3/rhTSH mice and helped restore thyroid activity to levels equivalent to those of euthyroid animals.
Conclusions:
Systemic radioiodide administration results in higher thyroidal iodide levels than oral administration, particularly in LID-fed mice. These data highlight the importance of LID, both in euthyroid and T3-treated, rhTSH-injected mice. Extrapolated to human patients, and in the context of clinical guidelines for the preparation of differentiated thyroid cancer patients, our data indicate that LID can potentiate the efficacy of rhTSH treatment in T3-treated patients.
Introduction
T
Additional factors may affect RAIT efficacy. Dietary iodine restriction can be used to increase radioiodine uptake and possibly improve the efficiency of 131I therapy, especially in the context of hormone withdrawal (5). The route of iodine administration (oral or intravenous) might also influence bioavailability and therefore uptake by target organs (6,7).
According to American Thyroid Association recommendations, dietary iodine restriction for patients receiving hormone replacement therapy is considered to be a weak recommendation with “low-quality evidence” (4) due to insufficient preclinical and clinical evidence on the impact of dietary iodine before RAIT treatment. To our knowledge, only one clinical study has explored RAIT and iodine restriction together (8), but only the urinary iodine-to-creatinine ratio was examined and no quantitative analysis of thyroid iodine uptake was performed. Data concerning the route of iodine administration are also limited and the results are controversial. A recent study performed in rats suggested that oral administration favors radioactive iodine uptake by the thyroid over the intravenous route (6), whereas some clinical data suggest that both routes have equal treatment efficacy (7).
In a clinical setting, assessing the impact of various combinations of preparative measures to treat differentiated thyroid cancer (DTC), including dietary iodine, hormone replacement therapy, rhTSH treatment, and intravenous iodine administration, is complex. With the development of dedicated high-resolution small-animal scanners, functional thyroid imaging can now be performed in rodents and these images can provide quantitative information on thyroid uptake under different experimental conditions. For instance, micro single-photon emission computed tomography (microSPECT/CT) imaging of mice was used to define the radiation dose required to induce thyroid stunning (9). Moreover, radiotracers such as 99mTc pertechnetate (99mTcO4 −) or 123I can be useful to refine imaging analyses. Both radiotracers are detectable using SPECT and are taken up by the thyroid and other organs that express the sodium iodide symporter (NIS) (10). However, unlike 123I, 99mTcO4 − is not covalently bound to thyroglobulin and therefore can be used as an iodide uptake marker (11).
The aim of this preclinical study was to use microSPECT/CT imaging to determine the influence of the administration route of either 99mTcO4 − or 123I on biodistribution, and to measure how different dietary iodide intake and recombinant human TSH (rhTSH) affects euthyroid and triiodothyronine (T3)-treated mice. Considering the lack of clinically relevant DTC animal models, we performed these experiments with mice, which are reported to have a similar NIS expression pattern to that of humans (12 –14).
Materials and Methods
Animals
Female, eight-week-old C57B/6J mice were obtained from Janvier. Animal housing and procedures were conducted according to French Agriculture Ministry guidelines and were approved by the local ethics committee (Ciepal NCE/2014-211).
Animal study protocols
To determine the influence of dietary iodide intake and the route of radiotracer administration, animals were fed either a normal-iodide diet (NID, around 1 μg iodide per day) or a low-iodide diet (LID <0.01 μg iodide per day) for 11 days. For T3 treatment, T3 at a final concentration of 3 μg/mL was added to the drinking water, which was available to animals ad libitum. The various experimental protocols used in this study are summarized in Figure 1.
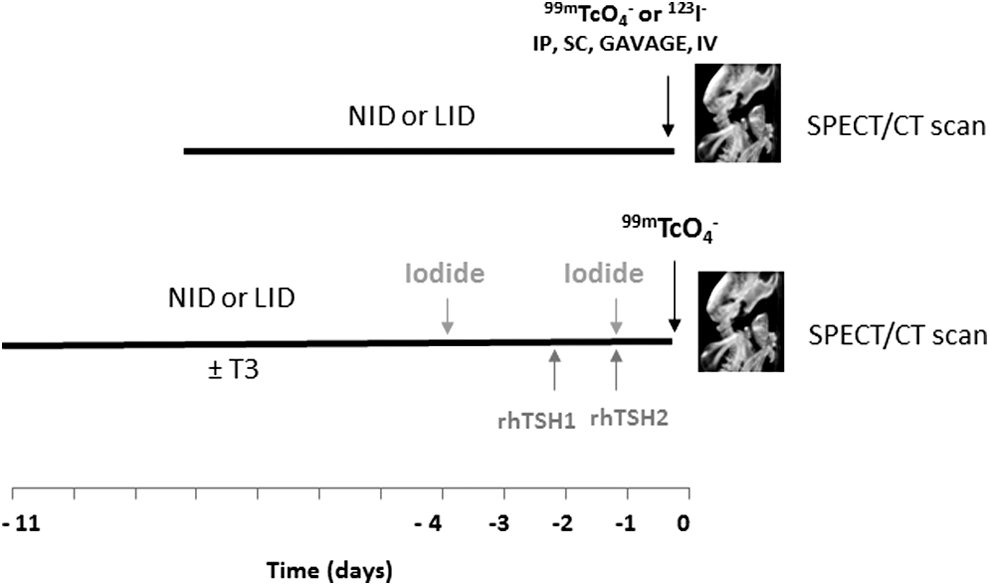
Study protocols. (
In vivo microSPECT/CT studies
99mTcO4 − was obtained from a freshly eluted 99Mo/99mTc generator, and 123I− sodium iodide was purchased from IBA Molecular. Animals were administered activities of 20 MBq 99mTcO4 − or 10 MBq 123I− intravenously, subcutaneously, intraperitoneally, or by gavage. Thyroid, salivary gland, and stomach tracer uptake was measured at different times using a dedicated microSPECT/CT scanner (eXplore speCZT CT120, GE) under gas anesthesia (air and 1–2% isoflurane) in an air-warmed imaging chamber (Minerve) to maintain body temperature at 37°C. The SPECT scanner uses a stationary full ring of cadmium zinc telluride (CZT) detectors and a rotating seven-pinhole (1 mm opening) collimator. A total of 350 projections were acquired over 360°C in 8 minutes.
Image analysis
Images were reconstructed using the manufacturer's 3D-ordered subset expectation maximization algorithm (5 subsets and 11 iterations), which incorporates the system's collimator–detector response function and scatter correction. Reconstructed images were analyzed and quantified using AMIDE software (15). Tracer activity in the various relevant organs was calculated as previously described (16). Three-dimensional regions of interest were drawn manually around the thyroid, salivary glands, and stomach. Pertechnetate uptake values were expressed as a percentage of the injected dose after decay corrections. Iodide-123 activity values were not corrected for nuclear decay. The results are expressed as the mean ± standard error of the mean.
TSH analysis
The quantitative determination of mouse TSH serum levels was performed by enzyme-linked immunosorbent assay (kit CEA463Mu, Euromedex) according to the manufacturer's instructions.
Membrane vesicle preparation, SDS-PAGE, and Western blot analyses
Thyroid membrane proteins were obtained as previously described (9,17) and subjected to SDS-PAGE electrophoresis. Western blotting was performed with an anti-mouse NIS antibody using an affinity-purified rabbit immunoreactive serum fraction, as previously described (18), or with an anti-β-actin antibody (Sigma).
Statistical analysis
Statistical analysis and determination of the areas under the curves (AUC) were performed using Prism (GraphPad software). Dual comparisons were made using Student's t-test and comparisons between multiple conditions were analyzed using ANOVA. Statistical significance was set at p < 0.05.
Results
MicroSPECT/CT images
Typical SPECT/CT images of a naïve mouse showing 99mTcO4 − uptake in the thyroid, salivary glands, and stomach regions were acquired (Fig. 2). Similar images were obtained when 123I− was used as the radiotracer (not shown).
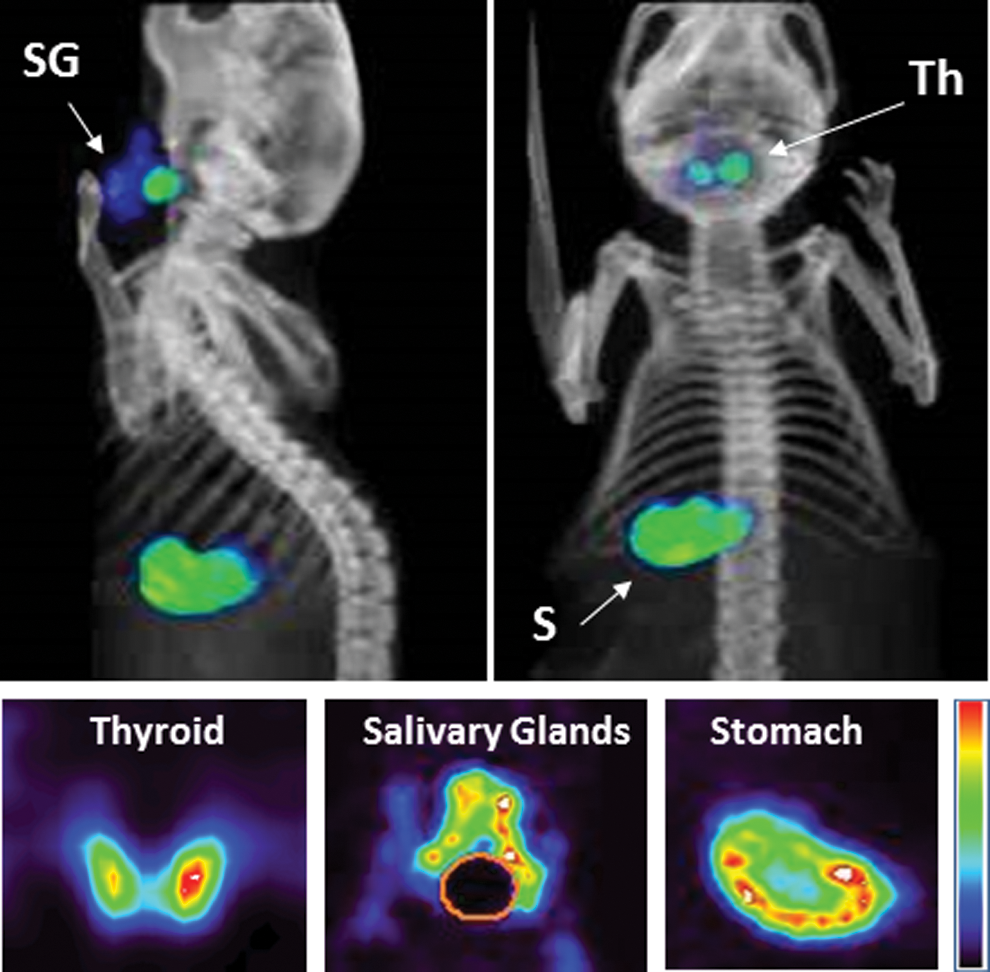
Representative microSPECT/CT images. Upper panels: Fused SPECT/CT, whole body images of control mice: anterior and lateral views show 99mTcO4 − uptake in the thyroid lobes (Th), salivary glands (SG), and stomach (S). Lower panels: Coronal slices of the thyroid, salivary glands, and stomach from a control mouse 60 minutes after 99mTc pertechnetate injection.
Influence of radiotracer administration route
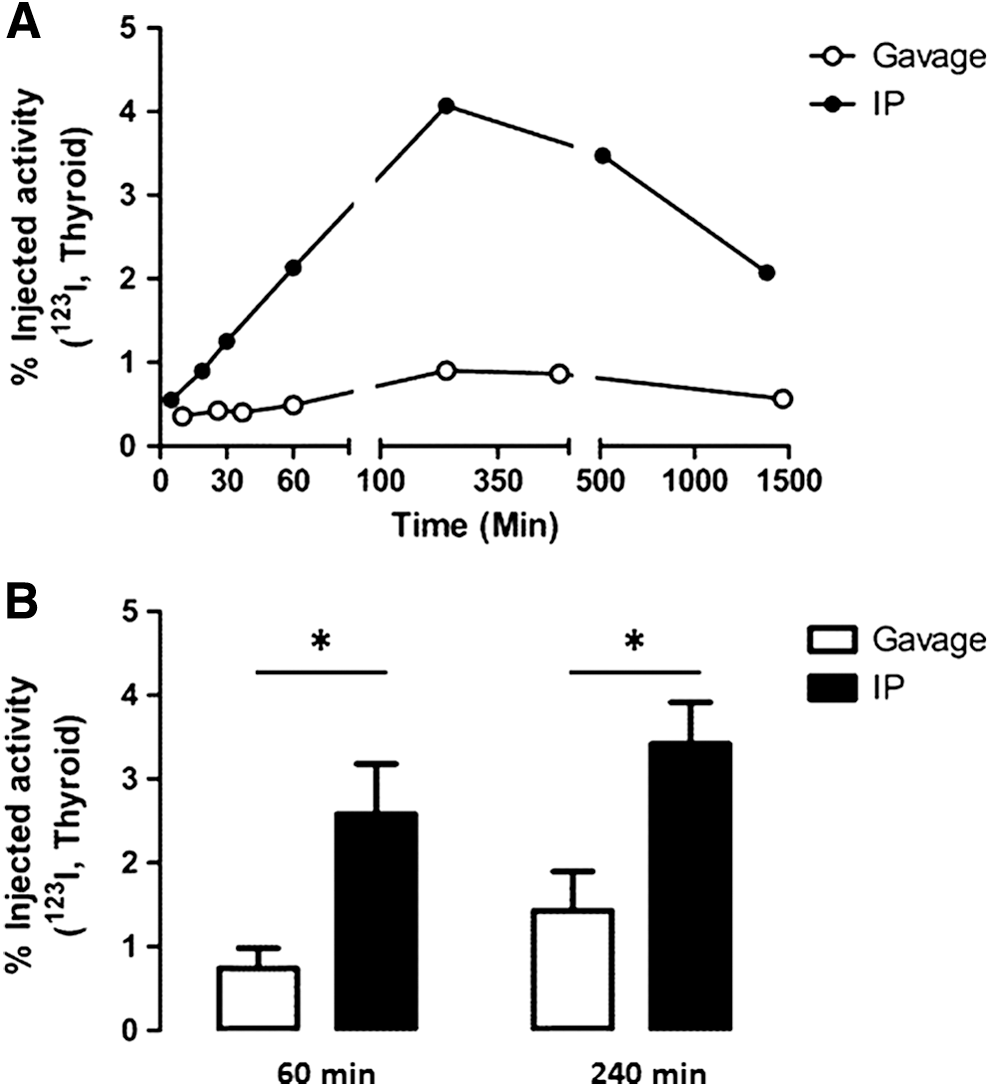
To determine the influence of administration route on radiotracer uptake by different organs expressing NIS, mice were fed an NID for 8 days and were scanned at different time points after radiotracer administration (99mTcO4 − or 123I−). At early time points (≤80 min), 99mTcO4 − accumulation in the thyroid was higher when the radiotracer was administered intraperitoneally or subcutaneously relative to gavage administration (Fig. 3A), which tended to result in accumulation of the radiotracer in the stomach (Fig. 3B). For both the thyroid and stomach, intraperitoneal and subcutaneous (Fig. 3) as well as intravenous (not shown) administration showed similar radiotracer uptake kinetics. These data suggest that gavage administration promotes radiotracer accumulation in the stomach rather than in other NIS-expressing organs. To confirm these outcomes, mice were administered 123I− intraperitoneally or by gavage. Thyroid and salivary gland uptake were monitored over a longer time period—up to 24 hours. The representative kinetics of 123I− accumulation in the thyroid showed that for both modes of administration, the radiotracer levels peaked four hours after administration (Fig. 4A). The AUC of 123I thyroid uptake in the intraperitoneal group was 3.63-fold higher than that of the gavage group (Figs. 4A, 5). Statistical analysis of thyroid uptake 1 and 4 hours after administration confirmed these results (Fig. 4B), which were consistent with those for NIS-expressing salivary glands (Fig. 4B).
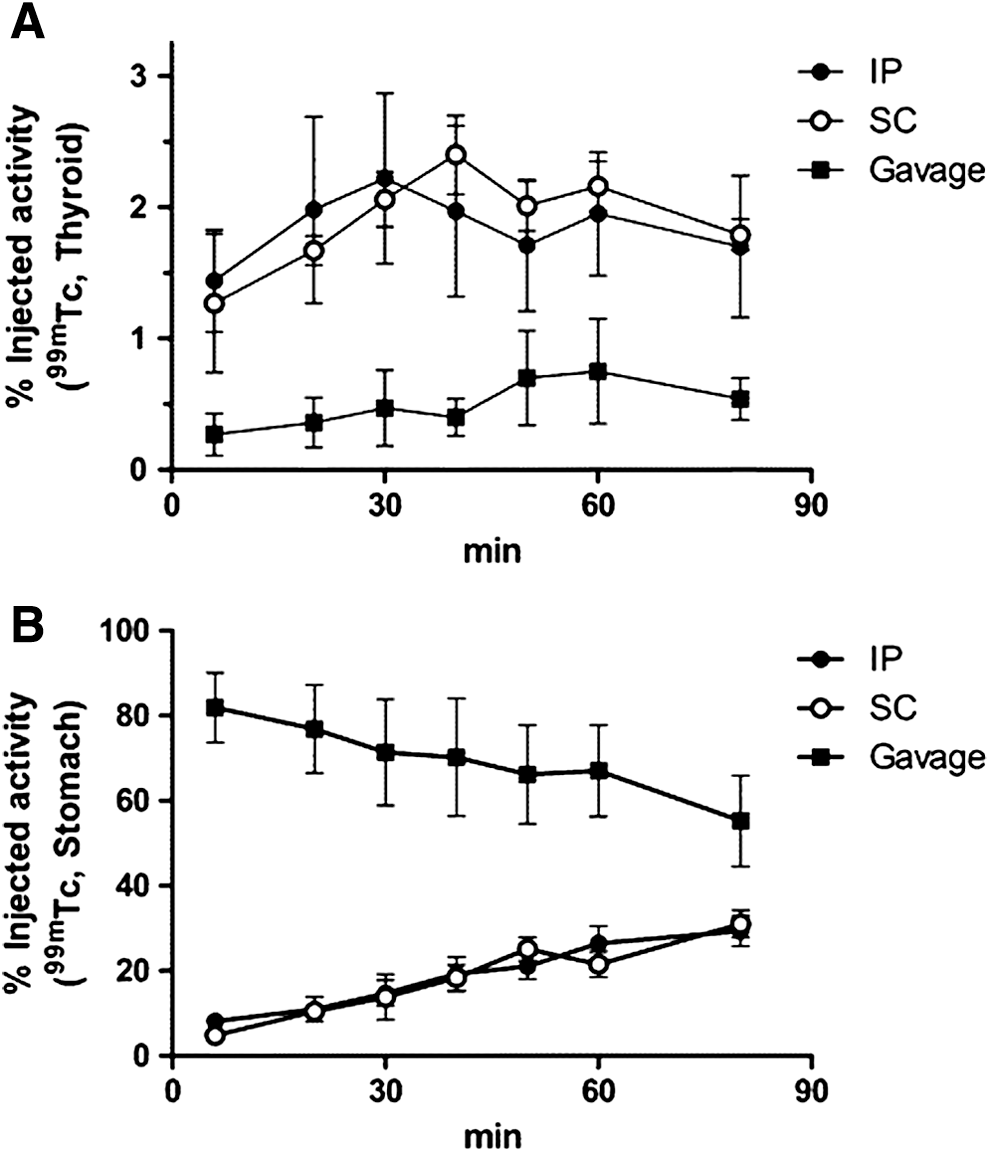
Effect of radiotracer administration route on short-term 99mTcO4
− uptake in the thyroid and stomach. A schematic representation of the general protocol is shown in Fig. 1A. Mice were fed only the NID and 99mTcO4
− was administered IP, SC, or by gavage. (

Effect of the radiotracer administration route on the kinetics of 123I− accumulation in thyroids and salivary glands of NID mice. A schematic representation of the general protocol is shown in Fig. 1A. The mice were fed only the NID and 123I− was administered either IP (black bars or signs) or by gavage (white bars or signs). (
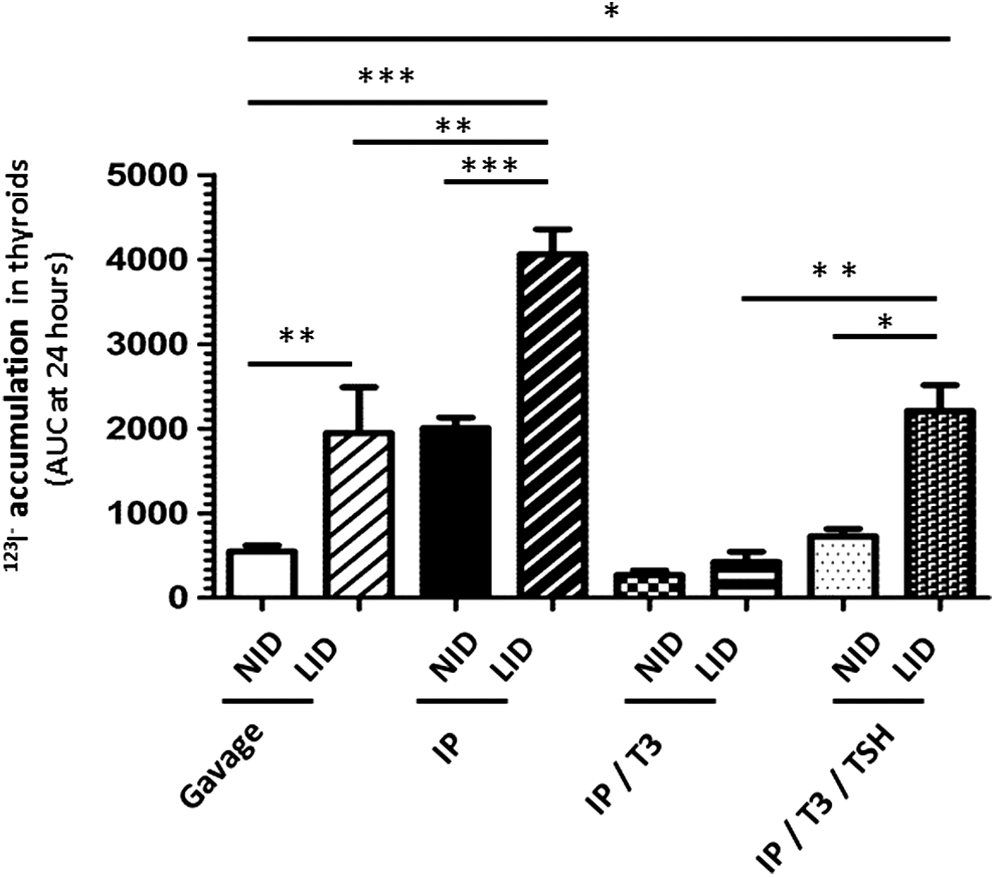
Comparative analysis of 123I− accumulation in the thyroids of mice prepared with different protocols. Iodine 123 thyroid uptake was measured by microSPECT/CT over time and expressed as the AUC (area under the curve) at 24 hours. The data represent averages (n = 2–6) of radiotracer accumulation in the thyroids of the mice. The results are expressed as the mean ± standard error of the mean (SEM). *p < 0.05, **p < 0.01, ***p < 0.001.
Effect of dietary iodide intake on radiotracer uptake by the thyroid
For mice fed a low-iodide diet (LID) for 10 days before the SPECT/CT scans, the kinetics of iodide accumulation in the thyroid were similar to those obtained for mice fed the NID, with peak radiotracer uptake 4 hours after administration (Fig. 6A). The AUC of 123I thyroid uptake following intraperitoneal tracer administration was two-fold higher than the AUC for the gavage group, thus confirming that intraperitoneal radiotracer administration results in a higher accumulation in the thyroid relative to gavage administration. In addition, radiotracer administration to LID mice resulted in a higher uptake in the thyroid than that seen for NID mice (Fig. 4B versus Fig. 6B and Fig. 5). For intraperitoneal administration of 123I−, thyroid activity at peak radiotracer levels was 2.2 ± 0.27% of the injected activity in NID mice, but reached 3.42 ± 0.5% in the LID mice (p < 0.05). Overall, combining the LID and systemic radiotracer administration produced a seven-fold higher accumulation of 123I− compared with NID/gavage.
Effect of the radiotracer administration route on the kinetics of 123I− accumulation in the thyroids of LID mice. A schematic representation of the general protocol is shown in Fig. 1A. Mice were fed only the LID and administered 123I− either IP (black bars or signs) or by gavage (white bars or signs). (
Effect of rhTSH injection on radiotracer uptake by the thyroid
We first compared 99mTcO4 − thyroid uptake in rhTSH-treated and untreated NID mice. As expected, rhTSH injection resulted in increased 99mTcO4 − uptake by the thyroid (1.7-fold increase) (Fig. 7A). We next assessed the effect of rhTSH on mice treated with T3. The T3-treated mice showed a dramatic drop in thyroid uptake that was increased by rhTSH injections, but not to the levels seen for NID-fed mice that did not receive T3 (Fig. 7A). To evaluate the impact of a large, transient increase in dietary iodine, 0.5 mg iodide was injected 4 days before the T3-treated NID animals were scanned. Although the 0.5 mg iodide dose did not affect thyroid uptake 4 days later, a smaller dose of iodide (10 μg) administered just 24 hours prior to the scan reduced thyroid uptake by 50%, suggesting that excess iodide can have a short-term effect on radiotracer uptake (Fig. 7B). We next evaluated the effect of a low-iodide diet using the same experimental protocol. In LID mice, T3 treatment mimicked that seen for T3-treated NID animals in that there was a significant decrease in the TSH levels as measured by enzyme-linked immunosorbent assay (301 ± 26 pg/mL mTSH in LID/T3 mice versus 691 ± 44 pg/mL mTSH in the LID mice). Meanwhile, rhTSH treatment of T3-treated LID mice resulted in a significantly higher increase in thyroid 99mTcO4 − uptake than that produced by rhTSH injection in T3-treated NID animals (Fig. 7C). These results mirror those for western blot measurement of NIS expression (Fig. 7D), which showed that NIS expression was higher in T3-treated LID animals than in T3-treated NID mice. Moreover, rhTSH injections resulted in higher NIS expression levels in T3-treated LID animals relative to T3-treated NID mice.

Effect of rhTSH injection on radiotracer uptake by the thyroids of NID and LID mice. (
These data were further confirmed in a kinetic evaluation spanning 48 hours using 123I− as the radiotracer (Figs. 5, 8). The AUC of 123I− thyroid uptake in the LID/T3 group was 1.6-fold higher than that for the NID/T3 group. For both groups, rhTSH treatment produced an increase in the AUC (2.9-fold and 5-fold for NID/T3 and LID/T3 mice, respectively). Finally, the AUC for the LID/T3/rhTSH group was 2.8-fold higher than that of the NID/T3/rhTSH group, and contributed to a restoration of thyroid activity to levels that were equivalent to that of euthyroid animals (AUC = 2111 in the LID/T3/TSH animals versus AUC = 2082 in the NID mice, Fig. 5).
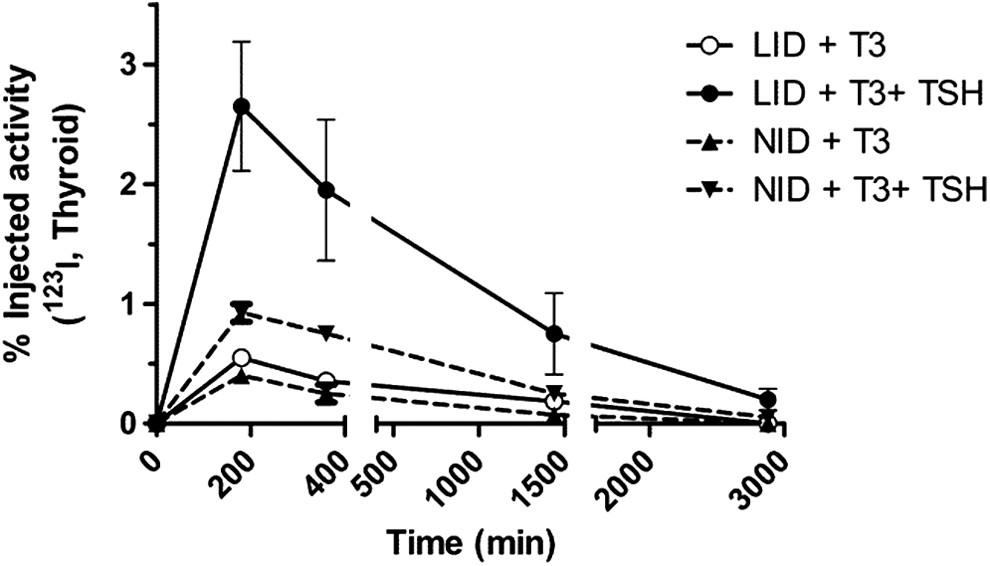
Long-term kinetics of 123I− accumulation in the thyroids of NID and LID mice, stimulated or not with rhTSH. The general protocol is shown schematically in Fig. 1B, in which 123I− was administered by IP. The data represent averages (n = 2) of radiotracer accumulation in the thyroids of NID mice and LID mice. Thyroid activities were not corrected for nuclear decay. The results are expressed as the mean ± SEM.
Discussion
Radioiodide is commonly used as an adjuvant treatment for DTC. Treatment effectiveness is dependent on the amount of radioiodide that accumulates in the thyroid, but there is little information about the impact of both dietary iodine and the route of 131I administration on RAIT efficacy. Thus, this study examined different preparative measures and how they affected the level of uptake by the thyroid. Here we show that systemic or subcutaneous administration of the radiotracer favors thyroid (and salivary gland) uptake of the radiotracer, while oral administration produces a significantly higher accumulation of the radiotracer in the stomach. In patients with Graves' disease, the route of administration (oral versus intravenous) of iodide does not affect the dose received by the thyroid or the outcome (7). In hyperthyroid cats, thyroid uptake and outcome were similar in animals administered radioiodide intravenously or subcutaneously (19). A recent study in rats suggested that the oral route of administration favors radioiodide accumulation in the thyroid compared with the intravenous route (6). This result is in contrast to our finding that oral administration produces lower levels of radioiodide uptake by the thyroid compared with systemic or subcutaneous administration. Notably, unlike human salivary glands, rat salivary glands are known to lack NIS expression (14), which suggests that radiotracer biodistribution in rats and humans may differ qualitatively. Considering the close proximity of the salivary gland to the thyroid, the lack of iodide retention in rat salivary glands may have important repercussions for biodistribution kinetics, and thus the quantitative data obtained using a rat model may not be relevant to humans. Meanwhile, mice and humans have similar NIS expression patterns (12,13), and this similarity together with our results obtained with mice suggests that systemic administration in humans may be better able to increase radioactive iodide uptake by extragastric tissues.
In standard practice, logistic considerations and ease of implementation of a clinical protocol are the main reasons to choose an enteral route for radioiodide administration. In this context, clinicians should consider whether the gain in radioactive accessibility for thyroid remnants and metastases outweighs the logistical advantages provided by the oral route of administration. In DTC patients, capsules containing 1–3.7 GBq are routinely given orally. When necessary, the treatment can be repeated, leading to a cumulative administered activity as high as 11.1 GBq (20). A recent retrospective study involving 2468 DTC patients concluded that a cumulative 131I dose <37 GBq did not increase the risk of a second primary malignancy (21). As such, in standard, routine situations the gains yielded by systemic administration would likely not outweigh the logistic advantages of oral delivery. However, the situation may be different for other therapeutic approaches. For example, a new therapeutic strategy based on the use of gene therapy to induce ectopic NIS expression in nonthyroid cancers is emerging (22,23). Moreover, replication-deficient viruses (24,25) and oncolytic viruses (26,27) have been used to deliver the NIS cDNA to several different types of cancer, and preclinical studies in rodent models were used to validate this approach as a proof of principle. However, when ectopic NIS expression was evaluated using SPECT/CT imaging and dosimetric calculations in a phase 1 clinical trial involving prostate cancer patients, men who were administered a 131I dose of 7.4 GBq had a mean absorbed dose in the prostate that was well below the dose required to eliminate cancerous lesions (28). Therefore, in this experimental situation, improvements related to a parenteral administration route of radioiodide would significantly increase the radiation dose received by the target tissue and should be considered.
We also found that mice fed an LID showed increased thyroid uptake of radioactive iodide. Considering that similar effects were observed when 99mTcO4 − and 123I− uptake were measured, the trapping function is likely to be more affected by dietary changes than is organification. It is well established that NIS protein expression is upregulated under conditions of an LID. The LID-induced increase in iodide uptake was present in both euthyroid and T3-treated mice; the T3 administration was designed to mimic the clinical preparation of patients receiving rhTSH while on substitution therapy with levothyroxine. This model system was initially developed by Colzani et al., who observed that the effect of rhTSH on thyroid uptake was higher in T3-treated mice compared with euthyroid animals (29). Alternatively, a mouse model that spontaneously develops metastatic follicular thyroid cancer exists. ThrbPV/PV mice harbor a knockin dominant negative mutation, known as PV, in the Thrb gene, and thus could be used to validate our conclusions in the context of experimental metastatic disease (30,31). In our model system, the data show that LID-fed animals had increased iodide uptake ranging between 55% and 128% over that seen for NID-fed animals. This result is in agreement with a recent systematic review of dietary iodine restriction in preparation for radioactive treatment or scanning in DTC patients, which concluded that LID increases radioactive iodide uptake and could improve 131I treatment outcomes (5). However, the majority of the studies reviewed included patients under thyroid hormone withdrawal; the only clinical study performed on patients with rhTSH preparation also concluded that a two-week LID optimizes radioiodine uptake (8). This conclusion was based on the urinary iodine-to-creatinine ratio and no quantitative analysis of thyroid iodine uptake was performed. Therefore, our data provide preclinical information to confirm and better understand the relevance of dietary iodine when patients are given rhTSH. Mechanistically, the Western blot experiments demonstrated that part, if not all, of this iodide-dependent effect is due to an elevation in NIS protein levels in the thyrocyte plasma membrane. The relevance of the results we obtained for euthyroid and T3-treated mice to human patients will probably depend on whether the thyroid cancer tissue retains the regulatory mechanisms of normal thyroid tissue. While this may vary among tumors, in general LID has been shown to increase radioiodine uptake by remnant tissue or tumors (32,33). Given the conflicting evidence on how an LID affects remnant ablation outcomes (5), additional studies will be needed for a complete demonstration of the effect of LID on iodide uptake.
Finally, the effect of rhTSH injections on thyroid radioiodide uptake was determined under different conditions. An increase in radiotracer uptake by the thyroid was observed in both euthyroid and T3-treated mice fed an NID. These data are in complete agreement with those of Colzani et al. (29), who studied the effect of rhTSH on NID-fed rats and mice. In this context, a large excess of iodide intake given four days before the scan failed to significantly affect radiotracer uptake. In contrast, iodide intake 24 hours before the scan reduced radiotracer uptake by 50%, probably through the Wolff-Chaikoff effect, which occurs in response to an acute iodide excess (34). These data also highlight the short duration of the effect of excess iodide intake on rhTSH-induced iodide uptake by the thyroid. In addition, our data extend the observations of Colzani et al. (29) to the LID condition. Evaluation of 123I− accumulation kinetics in the thyroid showed that administration of rhTSH to LID/T3 mice resulted in a 2.8-fold increase in the AUC compared with NID/T3 mice. In this model system, LID clearly increased the effect of rhTSH and helped to restore a thyroid activity that was equivalent to that of the euthyroid animals. These data suggest that a combination of LID and rhTSH for patients receiving thyroid hormone replacement therapy may be useful.
In conclusion, our data show that a series of preparative measures can increase thyroid radioiodine uptake and possibly improve 131I treatment outcomes, especially in the context of hormone replacement therapy. First, the systemic administration of radioiodide favors its accumulation in the thyroid compared to the oral route. While this approach is probably not needed for routine DTC cases, it may be relevant to improve the treatment of NIS-expressing tumors through gene therapy. Furthermore, our data highlight the importance of LID in both euthyroid or in T3-treated, rhTSH-injected mice. Extrapolated to the human situation, and in the context of clinical guidelines for preparation of DTC patients, our data indicate that LID may potentiate the efficacy of rhTSH treatment in T3-treated patients.
Footnotes
Acknowledgments
This work was supported by a grant from the Recherche en matières de Sûreté Nucléaire et Radioprotection program from the French National Research Agency and by a grant from Plan Cancer 2014–2019 (MTS201403). The authors thank Institut National de la Santé et de la Recherche Médicale (INSERM) and the radiopharmaceutical team of the Centre Antoine Lacassagne (Nadine Sapin, Guy Martinico, Stéphane Espitallier, and Didier Alberato) for their help with radioisotope production and handling. The authors gratefully acknowledge the Institute for Research on Cancer and Aging, Nice animal core facility. Equipment for this study was purchased through grants from la Région Provence Alpes-Côte d'Azur and INSERM. We thank Colette Ricort for assistance in preparing the manuscript.
All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Author Disclosure Statement
No competing financial interests exist.