
Abstract
Background:
A self-sequential longitudinal reference interval may be expected to minimize the inter-individual variation of thyroid function. Comparison between the self-sequential longitudinal reference interval (SLRI) and cross-sectional reference interval (CSRI) in pregnancy has not been well investigated. The objectives of this study were to establish a stringent SLRI of thyroid function in pregnant women and to compare it with the conventional CSRI.
Methods:
Three cohorts were enrolled: group 1, pregnant women for an SLRI (n = 99); group 2, pregnant women for a CSRI (n = 1318); group 3, non-pregnant control women (NC) as a control group (n = 301) according to the criteria of the National Academy of Clinical Biochemistry. Thyrotropin (TSH), total thyroxine (TT4), free thyroxine (fT4), total triiodothyronine (TT3), free triiodothyronine (fT3), serum ferritin (SF), and urine iodine concentration (UIC) were measured in the three groups.
Results:
Compared with CSRI, the reference interval of the SLRI group had narrower reference intervals of fT4 in the first and second trimesters (p < 0.05). The median of TSH was at a low level during the first trimester, and then gradually elevated in the second and third trimesters. The median of fT4 persistently decreased from 12 weeks, and did not return to the level of the NC group until 12 months postpartum. The TT4 increased to 131.4 nmol/L at gestational week 8, and reached a peak (170.0 nmol/L) at gestational week 12. In the first trimester, the prevalence of hypothyroxinemia was 9.1%, 4.0%, and 2.0% with a fT4 value below the 10th, 5th, and 2.5th percentile, respectively. In contrast, 29.3% of TT4 values were below the lower non-pregnancy reference limit multiplied by 1.5.
Conclusions:
No significant difference was found between a SLRI and a CSRI, even in a stringent self-sequential longitudinal reference interval of thyroid function in pregnant women. In addition, the limit of TT4 below the non-pregnant level multiplied by a factor 1.5 is not appropriate for diagnosing hypothyroxinemia in the first trimester.
Introduction
A
The gestation-specific reference intervals of thyroid function are probably also influenced by factors such as ethnicity, inter- or intra-individual variation, assay methods, iron deficiency, iodine deficiency, and body mass index (BMI) (12 –16). It was recently reported that iron deficiency is an independent risk factor for isolated hypothyroxinemia not only in pregnant women but also in non-pregnant women (16). Approximately 15% of women of reproductive age have iodine deficiency, even in the United States, which is generally an iodine-sufficient region (17). The incidence of isolated hypothyroxinemia in an overweight population was 3.64-fold compared with a normal-weight control population (18). Therefore, in the present study, a SLRI was established from eight weeks of gestation to 12 months postpartum in a pregnant population in whom iodine deficiency, iron deficiency, overweight, and positive thyroid antibodies were excluded compared with the conventional CSRI.
Materials and Methods
Subjects
The Subclinical Hypothyroid in Early Pregnancy (SHEP) study was conducted in Liaoning Province in China. The present study is part of the SHEP study. From August 2011 to June 2014, departments of obstetrics and gynecology and departments of endocrinology of 19 hospitals participated in this study. All participants lived in an iodine-sufficient region (median urine iodine concentration [UIC] = 160.2 μg/L in school-age children). Three cohorts were enrolled: group 1, pregnant women for a SLRI (n = 99); group 2, pregnant women for a CSRI (n = 1318) in whom 975 women were in the first trimester, 252 in the second trimester, and 91 in the third trimester; and group 3, non-pregnant women as a control group (n = 301). Recruitment criteria for pregnant women included: (i) aged 19–40 years; (ii) residing in the city for >10 years; and (iii) a singleton pregnancy at four to eight weeks. Exclusion criteria included: (i) multiple pregnancies; (ii) a personal or family history of thyroid disease; (iii) visible or palpable goiter confirmed by ultrasound; and (iv) patients on any medical regimen that may affect thyroid function, such as glucocorticoids, dopamine, or antiepileptic drugs. In the SLRI group, positive thyroid autoantibodies, overweight (BMI >25 kg/m2), iron deficiency (serum ferritin <12 μg/L), and iodine deficiency (median UIC <150 μg/L) were also exclusion criteria. In contrast to the strictly selected SLRI group, the above factors were not exclusion criteria in the CSRI group in order to reflect the real clinical situation.
Methods
In the SLRI group, samples were collected at nine time points (8, 12, 16, 20, 28, and 36 gestational weeks and 3, 6, and 12 months postpartum). The follow-up rate was 78.8% (78/99). In the CSRI group, samples were collected at different gestational weeks. In the non-pregnant group, only one sample was collected. Spot urine and blood samples were obtained in the morning after an overnight fast. Samples were stored at −20°C until shipped, and assayed in a centralized laboratory within one week. Additionally, 120 samples of school-age children were tested for UIC to assess the iodine status.
Serum TSH, free thyroxine (fT4), thyroperoxidase antibodies (TPOAb), thyroglobulin autoantibodies (TgAb), and serum ferritin (SF) were measured in all participants using electrochemiluminescence immunoassays with Cobas Elecsys 601 (Roche Diagnostics, Switzerland). The functional sensitivity of serum TSH was 0.002 mIU/L. The intra-assay coefficients of variation (CV) of serum TSH, fT4, TPOAb, TgAb, and SF were 1.57–4.12%, 2.24–6.33%, 2.42–5.63%, 1.3–4.9%, and 1.43–4.52%, respectively. The interassay CV values were 1.26–5.76%, 4.53–8.23%, 5.23–8.16%, 2.1–6.9%, and 3.52–7.91%, respectively. The laboratory reference ranges for TSH were 0.27–4.2 mIU/L, fT4 12–22 pmol/L, TPOAb 0–34 IU/mL, TgAb 0–115 IU/mL, and SF 12–150 μg/L. UIC was determined in all participants by the ammonium persulfate method based on the Sandell–Kolthoff reaction. The intra- and inter-assay CV for UIC were 3–4% and 4–6% at 66 μg/L and 2–5% and 3–6% at 230 μg/L, respectively.
Statistical analysis
The data were tested for normality using the Kolmogorov–Smirnov test. Categorical variables are expressed as frequencies and percentages. In the case of a normal distribution, continuous data are presented as mean value ± standard deviation. Otherwise, median and interquartile ranges are reported. The limits of the reference intervals were calculated as median, 2.5th percentile, 97.5th percentile. The Mann–Whitney U-test and Kruskal–Wallis test were performed for comparing continuous data that did not conform to normal distribution. Student's t-test and one-way analysis of variance were conducted to evaluate differences between quantitative variables that were normally distributed. Spearman's correlation test was used to examine the correlation between non-normality variables, and the Pearson's correlation test was used to examine the correlation between normality variables. All statistical analyses were performed using SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered as statistically significant. G*Power was used to perform the power analysis, and most power factors were >80% in order to support the reliability of the results.
Ethics committee approval
All research protocols were approved by the Medical Ethics Committee of China Medical University, and were congruent with the declaration of Helsinki. Informed consent was obtained from every patient.
Results
Iodine status and characteristics of the reference population
The clinical characteristics of the reference population are summarized in Table 1. According to the historical data, the three cohorts lived in an iodine-sufficient region. The median UIC in school-age children was 160.2 μg/L; the median UIC of pregnant women before eight weeks of gestation was 167.78 μg/L; and the median UIC in child-bearing age women was 177.36 μg/L.
Values shown as median and IQR (25th, 75th).
SLRI, self-sequential longitudinal reference interval; CSRI, cross-sectional reference interval; BMI, body mass index; UIC, urinary iodine concentration; Tg, thyroglobulin; SF, serum ferritin.
Gestation-specific reference intervals of thyroid function in the SLRI group
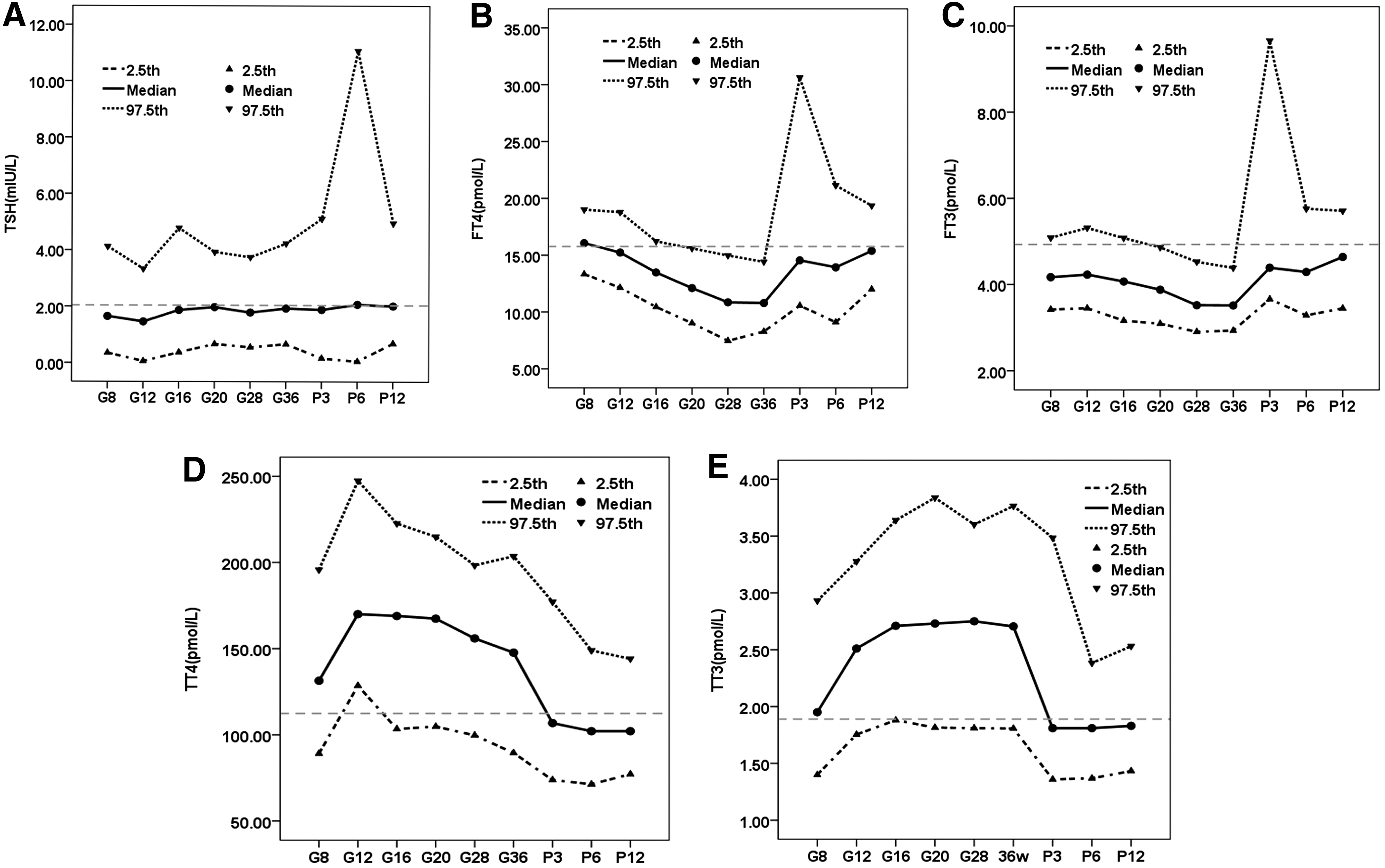
Table 2 shows the trends of the SLRI throughout gestation and postpartum, and compares it with non-pregnant levels. The median concentrations of TSH decreased significantly at eight weeks of gestation, reached a nadir (1.46 mIU/L) and then increased from then on before returning to the level of the non-pregnant state after childbirth (Fig. 1). fT4 levels decreased from 12 weeks of gestation, with a nadir in the third trimester, and did not return to the level of non-pregnancy until 12 months postpartum (Fig. 1B). Median concentrations of free triiodothyronine (fT3) decreased from eight weeks of gestation, and were lower than the non-pregnant levels during pregnancy at 12 months postpartum (p < 0.001; Fig. 1C). The median total thyroxine (TT4) increased slightly to 131.4 nmol/L (117% of the non-pregnant level) at eight weeks of gestation, and reached a level of 170.0 nmol/L (151% of the non-pregnant level) at 12 weeks of gestation. It decreased after delivery, and was lower than the non-pregnant level at 12 months postpartum (p < 0.001; Fig. 1D). The median total triiodothyronine (TT3) concentration rose continuously from eight weeks of gestation and remained stable during gestation. It decreased postpartum, and returned to the non-pregnant level at three months postpartum (Fig. 1E).
Dynamic changes of
Compared with the upper gestation week.
Compared with the nonpregnant group.
TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; TT4, total thyroxine; TT3, total triiodothyronine.
Comparison of SLRI and CSRI
The reference intervals of thyroid function in the SLRI and CSRI groups (median, 2.5th percentile, 97.5th percentile) are listed in Table 3. No significant differences in reference intervals of TSH existed between the SLRI and CSRI groups (first trimester 0.35–4.13 mIU/L vs. 0.35–4.47 mIU/L; second trimester 0.37–4.78 mIU/L vs. 0.07–4.52 mIU/L; third trimester 0.55–3.75 mIU/L vs. 0.75–3.77 mIU/L, respectively; p > 0.05). In the first and second trimesters, the reference intervals of fT4 in the SLRI group were narrower than those in the CSRI group (first trimester 13.35–19.01 pmol/L vs. 13.10–20.31 pmol/L, p < 0.01; second trimester 10.45–16.22 pmol/L vs. 9.17–17.74 pmol/L, p < 0.05). However, in the third trimester, no difference was found in the reference intervals of fT4 between the SLRI and CSRI groups (7.47–14.97 pmol/L vs. 6.94–13.38 pmol/L, p > 0.05).
Compared with the CS group, p < 0.01.
Compared with the CS group, p < 0.05.
T1, first trimester; T2, second trimester; T3, third trimester; M, median; P2.5, 2.5th percentile; P97.5, 97.5th percentile.
Diagnosis of hypothyroxinemia in the first trimester
Hypothyroxinemia in the first trimester was defined as a fT4 value below the 10th, 5th, and 2.5th percentile (fT4 <14.15 pmol/L, <13.67 pmol/L, and <13.33 pmol/L, respectively, in the first trimester in the present study), or a TT4 value below the lower non-pregnant reference limit multiplied by 1.5 (TT4 <1.5 × 81.01 pmol/L in the present study) with a concomitant normal TSH level. In the SLRI group, the prevalence of hypothyroxinemia in the first trimester was 9.1%, 4.0%, and 2.0% based on fT4 criteria, respectively, which was much lower than a finding of 29.3% based on the TT4 criteria (p < 0.000, p = 0.000, and p = 0.000; Table 4).
Discussion
This study demonstrates a stringent SLRI of thyroid function throughout pregnancy (from eight weeks of gestation to 12 months postpartum), and compares it with the conventional CSRI in an iodine-sufficient region in the northeast of China. A SLRI may be expected to minimize the inter-individual variation of thyroid function. However, in this study, there was no significant difference between the SLRI and the CSRI, which is inconsistent with the findings of some other studies. Andersen et al. (19) reported that the intra-individual variation of thyroid function tests in non-pregnant individuals was smaller than the inter-individual variation. Boas et al. (20) drew a similar conclusion. Yu et al. (21) calculated longitudinal reference intervals in the Chinese population, and demonstrated narrower intervals compared with the cross-sectional studies. Wang et al. (3) compared a SLRI with a CSRI and suggested no significant differences in most reference intervals. However, the interquartile range of a SLRI was usually smaller than that of a CSRI, especially in the first trimester. In the present study, the reference intervals of fT4 were narrower in the first and second trimesters in SLRI than those in CSRI were. However, in the third trimester, there was no significant difference in the width of reference intervals between the two groups. Although a SLRI may be expected to minimize the inter-individual variation of thyroid function, the present study suggests that no significant differences exist between SLRI and CSRI, even in a strictly selected pregnant population.
In addition, the CSRI was also influenced by different assay methods (22). The liquid chromatography tandem mass-spectrometry (LC/MS) method improved the accuracy of free measurements during pregnancy due to its higher reliability, reproducibility, and specificity (23). However, fT4 measured by LC/MS is not widely used because of technical difficulties and high costs (24). Compared with LC/MS, immunoassays are easier to implement. The free hormone index (fT4I) method indirectly estimates free hormone concentrations with two separate measurements and corrects the total hormone concentration for the influence of abnormal binding proteins, primarily thyroxine-binding globulin (TBG), based on a simple calculation (25). The fT4I method is less convenient than immunoassays and not widely used in clinical practice. However, some authors question the accuracy of immunoassays (12,22) because immunoassays do not test the serum fT4 directly, and they are influenced by changes in binding proteins such as albumin and free fatty acids during pregnancy (4). fT4 values measured by LC/MS correlate generally to a greater degree with logTSH values compared with values measured by immunoassays (26). Sapin et al. (27) reported that significant inaccuracies were observed in fT4 by immunoassays due to alterations in binding proteins. Kahric-Janicic et al. (23) suggested that fT4 concentrations determined by immunoassays were not in line with those determined by LC/MS. fT4 decreased with each successive trimester when measured by LC/MS, although it increased after the second trimester when measured by immunoassays. However, Anckaert et al. (28) compared fT4 results by three different immunoassays with those obtained by LC/MS assays, and proved that two of the immunoassays gave a consistent pattern with those by LC/MS assays. In the present study, fT4 concentrations measured by immunoassays decreased with progression of trimesters and displayed a consistent tendency with that obtained by LC/MS assays in the study by Kahric et al. (23) (Fig. 2). Moreover, fT4 measured by immunoassays negatively correlated with TSH in the first trimester in the present study (r = −0.201, p < 0.01), which suggests immunoassays could be used for measuring fT4 during pregnancy.

Comparison of fT4 by immunoassay with isotope dilution liquid chromatography tandem mass spectrometry (23). Box plot representation of the descriptive statistics for fT4. The square depicts the mean, the line shows the median, the top and bottom of the box represent the 75% and 25% percentile, respectively, and the whiskers show the 90th and 10th percentile.
Hypothyroxinemia is defined as a normal TSH concentration in conjunction with fT4 concentrations below the 10th, 5th, or 2.5th percentile of the reference range (29). With a fT4 <10th percentile as the diagnostic criterion of hypothyroxinemia, the prevalence of mild hypothyroxinemia was 8.5% (30), which was consistent with 9.1% detected in this study. It has also been suggested to use TT4 to evaluate pregnant hypothyroxinemia, provided that the non-pregnant reference limits are adjusted by a factor of 1.5 (31). However, in the present study, with the lower limit of TT4 below the non-pregnant level multiplied by a factor 1.5 as the diagnostic criterion of hypothyroxinemia in the first trimester, the prevalence of hypothyroxinemia was 29.3%, which is much higher than that found in other reports (30). The explanation for the higher prevalence for hypothyroxinemia is that the median concentrations of TT4 values only increase by about 1.5 times by 12 weeks of gestation. However, in the present study, most pregnant women were screened before eight weeks of gestation, which led to an overdiagnosis for hypothyroxinemia.
In summary, a SLRI from eight weeks of gestation to 12 months postpartum in Chinese pregnant women with sufficient iodine intake, normal iron status, and normal BMI has been established, and a CSRI was collected as a control. Although a SLRI may be expected to minimize the inter-individual variation of thyroid function, there was no significant difference between the SLRI and the CSRI, even in a strictly selected pregnant population. fT4 measurements by immunoassay were consistent with that obtained by LC/MS in the diagnosis of hypothyroxinemia. In addition, the use of a lower TT4 reference limit multiplied by 1.5 is not appropriate for diagnosing hypothyroxinemia in the first trimester.
Footnotes
Acknowledgments
We gratefully acknowledge the residents who participated in this study. This work was supported by National Science and Technology Support Program (2014BAI06B02); Chinese National Natural Science Foundation (81170730); Research Foundation of Key Laboratory of Endocrine Diseases, Department of Science and Technology, Shenyang government, Liaoning province, China (F11-244-1-00); Liaoning science public research funds (2014001001/GY2014-A-001); key platform foundation of science and technology for the universities in Liaoning Province (16010).
Author Disclosure Statement
The authors have no potential conflict of interest to declare.