
Abstract
Background:
Tumor marker doubling time (DT) has been proposed as a prognostic marker for various types of cancer. The present study analyzed the DT of the thyroid-specific tumor marker thyroglobulin (Tg), focusing on patients with progressive differentiated thyroid cancer (DTC).
Methods:
A total of 144 Tg courses of 99 patients with progressive or recurrent DTC were included (median observation period 19 months, 3–11 Tg measurements per course) in this retrospective study. The distribution of Tg-DT was determined for both a highly sensitive assay (functional working range 0.03–3 ng/mL) and a routine assay. Tg-DT and other prognostic markers were used to perform uni- and multivariate statistical analyses for survival predictors.
Results:
The median Tg-DT was 212 days (95% percentile: 49–961 days). No significant differences were observed between DT derived from Tg values in the very low range using a highly sensitive assay and DT calculated from Tg values measured by a conventional Tg assay. Multivariate analysis yielded no simple correlation between Tg-DT and survival rate, but the mortality risk of patients with a Tg-DT <5 months was more than twice as high as compared with a Tg-DT of >14 months. Highly significant differences on survival rates were only observed in patients with a high tumor load (Tg >100 ng/mL).
Conclusions:
Tg-DT alone is not an independent survival predictor in all patients with progressive DTC; however, analyzing only patients with a high tumor load, we found highly significant differences in survival rates.
Introduction
T
After initial surgery, serum Tg considerably decreases according to its half-life of approximately 65 hours (1), but often remains detectable at a low level. Even after successful subsequent radioiodine therapy, Tg levels may show a steady decrease over several months, reflecting protracted radiation effects as well as the long-term effect of levothyroxine suppressive therapy (2). After a median follow-up of five years, Durante et al. observed Tg values below the detection limit (<1 ng/mL) in 95% of patients without radioiodine remnant ablation and in 99% of the patients who did undergo radioiodine remnant ablation (3).
However, the Tg detection limit depends on the type of assay used. Over the last years, assays with improved functional sensitivity became commercially available, allowing the detection of lower Tg levels compared with routinely used assays. Current recommendations concerning the application of highly sensitive assays have been published recently (4).
The level of a single Tg value is not the only clinically relevant marker. In particular, for long-term follow-up, Botsch et al. (5) already postulated in 1983 that the trend observed in serial Tg determinations is more meaningful than a single value to assess treatment success. They stated that regardless of changes in tumor differentiation and consecutively loss of radioiodine uptake in the time course, increasing Tg levels correlate with tumor growth in most cases of tumor progression (5). Similarly, several other authors underline the clinical impact of serial Tg measurements (6 –8). Based on these publications, the revised American Thyroid Association (ATA) guidelines recommend analyzing the Tg trend to identify patients with clinically significant residual disease and noted that Tg-DT may serve as a predictor of recurrence (9). However, none of the above-cited publications includes distinct recommendations regarding quantitative criteria of Tg dynamics.
Tumor marker doubling time (DT) has been a predictive marker for outcomes in patients with various types of cancer, for example the DT of prostate-specific antigen (PSA) in prostate cancer (10 –13) or the DT of calcitonin and carcinoembryonic antigen (CEA) in medullary thyroid cancer (14,15). The first analysis dealing with calcitonin-DT was published in 1983 (16). The authors showed that calcitonin-DT highly correlated with life expectancy and tumor recurrence. Later, Barbet et al. (17) reported the prognostic importance of calcitonin-DT, whereas CEA-DT was a less valuable predictor of survival. In contrast, regarding DTC, there is only one study that systematically investigated Tg-DT and its prognostic impact (18). More precisely, Miyauchi et al. (18) demonstrated that Tg-DT is a prognostic marker in DTC patients. Basically, in patients with a Tg-DT of <12 months, the 10-year survival rate was 50%, and it was considerably lower than for patients with a Tg-DT of 12–36 months. Of paramount importance, Miyauchi et al. (18) included not only patients with progressive disease, but also patients with stable and even declining Tg values, and excluded thyroid carcinoma with other histology than papillary thyroid carcinoma (PTC).
The present study focused on the analysis of Tg-DT in DTC patients with progressive disease. In addition to “conventional” Tg measurements, a highly sensitive Tg assay was included in this study. The observed Tg-DT and other potentially prognostic markers were used to perform uni- and multivariate statistical testing for survival rate analyses.
Materials and Methods
Patients and follow-up
Tg courses of routine follow-up of outpatients with progressive or recurrent DTC followed in the authors' thyroid cancer center between 1994 and 2008 were included in this retrospective study.
Inclusion criteria were: (i) patients with histologically proven DTC, who had undergone thyroidectomy and radioiodine therapy in the past (initial diagnosis up to 21 years before inclusion in this study); (ii) unequivocal relapsing or progressive tumor (confirmed by successful tumor localization corresponding to “structural disease” by means of high-resolution neck ultrasonography, radioiodine whole body scintigraphy, computed tomography [CT], and/or positron emission tomography [PET]); (iii) an observation period of at least six months without any therapeutic intervention in the meantime; (iv) availability of at least three Tg measurements during this observation period under thyroid hormone therapy (TSH <0.3 mIU/L); and (v) further follow-up of at least five years after completion of the data collection unless the patient died earlier.
Exclusion criteria were: (i) elevated anti-Tg autoantibodies and/or disturbed Tg recovery test; (ii) increasing Tg levels without evidence of structural disease in the course; and (iii) patients with stable disease. A typical Tg course included four measurements over a mean ± standard deviation (SD) period of 583 ± 328 days. All patients with localized tumor progression had increasing Tg levels and vice versa.
According to the above-mentioned criteria, 144 Tg courses of 99 patients (62 females, aged 16–77 years) were identified, of whom 66 had follicular thyroid carcinoma (FTC) and 33 had PTC. Thirty-seven patients had only locoregional tumor manifestations, and 62 patients had distant metastases (74% of the patients with FTC had distant metastases, and 66% of the patients with PTC had locoregional tumor manifestations). In some courses with highly sensitive Tg measurements (see below), successful detection of tumor tissue was only possible several months to years after the initial Tg measurement when the tumor mass was large enough. In patients who had several courses of rising Tg (with therapeutic interventions in between), only the first course was used for correlation with survival analyses.
Thyroglobulin measurement
All Tg values of one course were measured with an identical type of assay (first-generation assay for routine use or highly sensitive second-generation assay for some sera in which Tg levels were below the limit of quantification of the second-generation assay). Between 3 and 11 serum Tg measurements under levothyroxine therapy (TSH <0.3 mIU/L) were performed during each course without any further therapeutic interventions in-between. The first-generation assay was a sandwich immunoradiometric assay (IRMA) with a functional sensitivity of 0.5 ng/mL and an upper limit of the working range of 250 ng/mL, which was used in 121 courses, (SELco® Tg; Medipan, Dahlewitz, Germany). In 23 courses, Tg was not detectable using the IRMA, but it was detectable with a second-generation assay, a high-sensitivity enzyme-linked immunosorbent assay (ELISA; more precisely, an immunoenzymometric assay [IEMA]) with a functional sensitivity of 0.03 ng/mL (Medizym® Tg Rem; Medipan). According to Spencer et al. (1996), functional sensitivity was defined as a Tg concentration in which the interassay coefficient of variation is 20%. Detailed data of both assays—including intra- and inter-assay precision profiles and dilution effects—have been published by Wunderlich et al. (2001) and Zöphel et al. (2002) (19 –21). The IEMA is strictly calibrated against the European reference preparation CRM 457, now described as BCR 459. Tg values determined by the highly sensitive IEMA are on average 1.7-fold higher compared with the routinely used IRMA (20,22).
None of the included patients had elevated anti-Tg autoantibodies (TgAb) or interferences reflected by a disturbed recovery test. Undisturbed recovery is defined as 70–130% for the routine IRMA, or as 60–140% for the highly sensitive IEMA. TgAb were measured with a direct, non-competitive two-step radioligand assay (CentAK anti-Tg; Medipan; functional sensitivity 15 IU/mL) or an automated non-competitive immunometric assay (Immulite 2000 anti-TgAb; Siemens Medical Solutions, Erlangen, Germany; functional sensitivity 20 IU/mL).
Statistical analysis
Tg-DT was calculated according to the log-slope method (12). After confirming the exponential changes of the measured Tg values, the natural log value of each Tg measurement was calculated. These numbers were plotted versus time, and the slope of the linear regression was measured through the data points.
The tumor growth is reflected in the variable λ (slope of the regression line in a semi-logarithmic plot). Tg-DT is calculated using the equation Tg-DT = ln2/λ. Zero time point was defined as the date of the first included Tg measurement with a following increase of Tg. The endpoint was defined as the date of death or an alternative endpoint (date of the last contact to the patient = censored cases).
The Kaplan–Meier method was adopted to analyze time-dependent variables. The influence of the following covariates was tested in a Cox regression model: Tg blood level, primary tumor status in TNM staging system (T1, T2, T3, or T4; 5th ed. UICC), histologic type, prevalence of distant/locoregional metastases, and degree of radioiodine accumulation (semi-quantitative scale with three levels, determined by two independent examiners). A significance level (p-value) of <5% was considered statistically significant.
Results
Distribution of Tg-DT
The median Tg-DT was 212 days (range 1 month to 4 years [confidence interval 49–961 days]; Fig. 1). There were no significant differences between Tg-DT using a highly sensitive assay for Tg-measurement or a first-generation assay (Table 1). The mean estimated error of Tg-DT (23) was approximately 14%, which was inversely correlated with the number of Tg measurements, starting with an error of 21% for three measurements and decreasing to 8% for seven or more measurements (Table 2).

Distribution of thyroglobulin (Tg) doubling time (DT).
The rows of the table contain data for different ranges of the geometric means of the individual Tg courses: row 1, highly sensitive Tg measurements; rows 2–5, routine assay measurements.
Tg, thyroglobulin; DT, doubling time; IEMA, immunoenzymometric assay
Tg-DT and prognosis
Patients were classified into five groups on the basis of the geometric mean of Tg values of each course: highly sensitive IEMA range (0.14–1.0 ng/mL), ≤10 ng/mL, >10–100 ng/mL, >100–1000 ng/mL, and >1000 ng/mL. Kaplan–Meier cause-specific survival rate curves showed a clearly worse survival rate for patients with higher Tg level, regardless of Tg-DT (p < 0.001; Fig. 2).
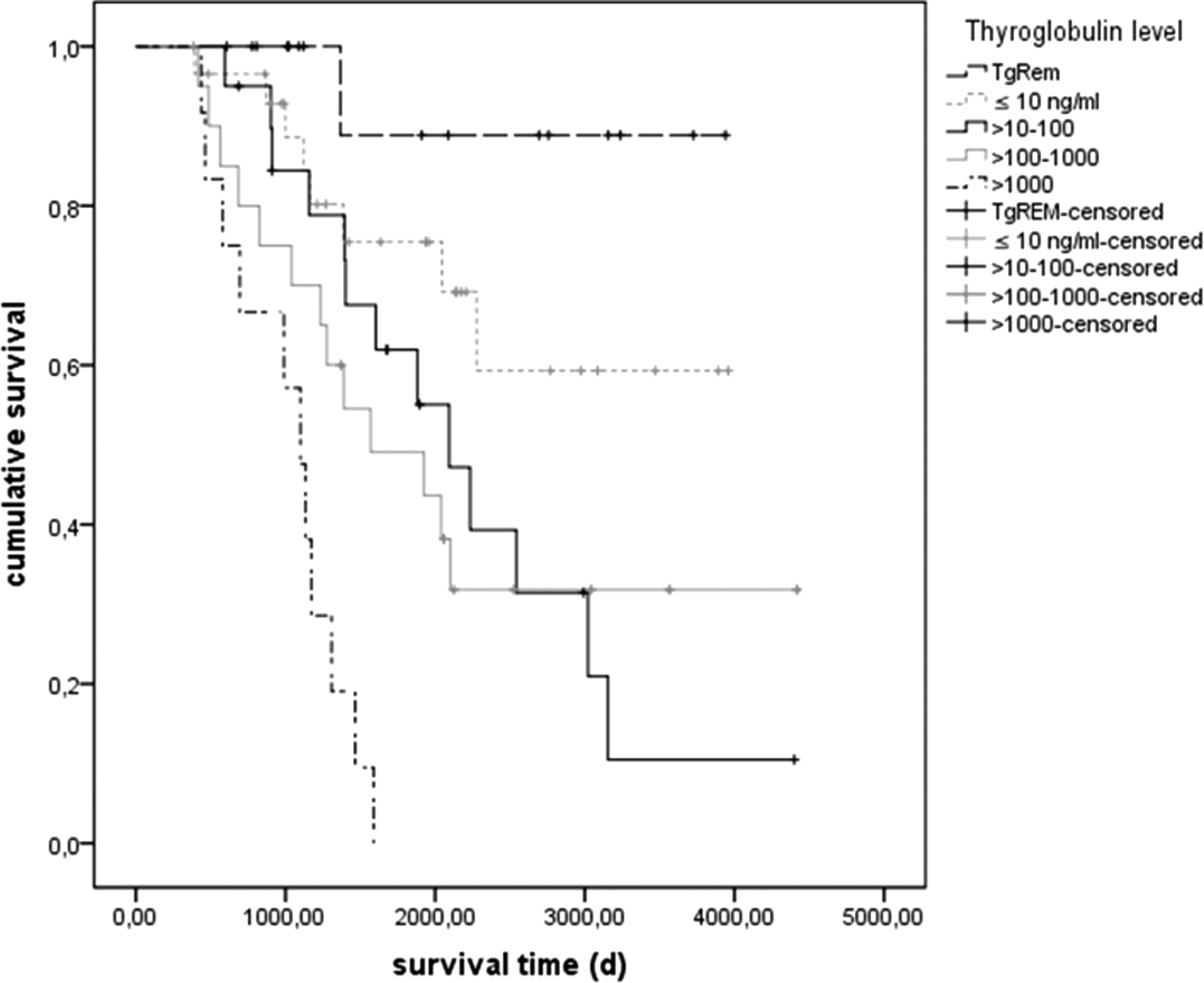
Survival rates dependent on Tg levels. The endpoint was defined as the date of death or an alternative endpoint (date of the last contact to the patient = censored cases).
Not surprisingly, higher prevalence rates of distant metastases were associated with a worse outcome compared with solely locoregional metastases (p < 0.01). In contrast, histologic types, capability of radioiodine accumulation and the primary tumor status in TNM staging system (T1, T2, T3, and T4) were not significant prognostic factors in this patient cohort.
In univariate analysis of Tg-DT, no simple correlation was found between Tg-DT and survival regarding the total patient sample (exp[B] = 0.9). Including age and sex did not result in significant differences between male and female or young and old patients (p = 0.37).
One classification referred to cutoff values from publications concerning DT of tumor markers other than Tg (e g., PSA in prostate cancer) included four groups: Tg-DT < 3 months, 3–6 months, >6–12 months, and >12 months. There were no significant differences in patient survival between these groups.
Another classification on the basis of quartiles led to the following groups: Tg-DT <5 months, 5 months to <7.5 months, 7.5 months to <14 months, and >14 months. The mortality risk of patients with a Tg-DT <5 months was more than twice as high as the mortality risk of patients with a Tg-DT of >14 months. Multivariate analysis including the covariates of the prevalence of distant or locoregional metastases, Tg blood level, and degree of radioiodine accumulation confirmed a doubling of mortality risk of patients with a Tg-DT <5 months compared to a Tg-DT of >14 months (adjusted to the above-named covariates, exp[B] = 2.7).
Interestingly, analyzing exclusively patients with a Tg level (geometric mean) >100 ng/mL (which concerns 29 of our total sample of 99 patients) representing a high tumor load, significant differences were found in survival rates when the Tg-DT was classified into the three groups < 3 months, 3–12 months, and >12 months (p < 0.05; Fig. 3).

Survival rates of patients with a Tg level >100 ng/mL (geometric mean) dependent on Tg-DT. The endpoint was defined as the date of death or an alternative endpoint (date of the last contact to the patient = censored cases).
Discussion
Patient sample and study performance
By applying our above-described inclusion and exclusion criteria a patient sample was selected, which does not reflect the normal distribution of histological tumor types and risk profiles. Furthermore, focusing on courses with long observation periods without therapeutic interventions in the meantime led to selection of patients in whom no effects from established treatment modalities (e.g., curative surgery or radioiodine therapy) could be expected.
Thus, in this series of patients, the percentage of FTC is above average compared with PTC (in contrast, in German epidemiologic surveys, the incidence of PTC is about four times higher than that of FTC) (24). However, in several other studies that deal with progressive thyroid cancer, the percentage of FTC is higher than that of PTC; this also applies to studies of patients selected for tyrosine kinase inhibitor therapy (25,26). Thus, applying the above-mentioned inclusion criteria, those patients in which the Tg-DT plays a critical role were selected.
Distribution of Tg-DT compared to DT of other tumor markers
Most DTC are well treatable and have a better prognosis than other tumor types. It is noteworthy that the median Tg-DT in the present cohort is considerably shorter (approximately seven months) than other reported tumor marker DTs, for example calcitonin or CEA for medullary thyroid cancer (27). The median calcitonin-DT calculated by Giraudet et al. (27) was 19 months, and the median CEA-DT was 24 months. These findings reflect the relatively good prognosis of medullary thyroid cancer in the majority of patients. In the present cohort consisting of DTC patients, the Tg-DT showed a wide variation, ranging from one month to four years. Similarly, Giraudet et al. (27) demonstrated values between 2 and 146 months for calcitonin- and CEA-DT for medullary thyroid cancer.
Tg-DT in patients with progressive disease
The relatively short median Tg-DT of only 212 days is likely due to the fact that this study focused exclusively on patients with progressive disease and increasing Tg levels. The percentage of patients with an advanced tumor stage was disproportionately high in the patient sample: 61% had distant metastases, 29% had a mean Tg blood level of ≥100 ng/mL, and the highest Tg measurement was 190,000 ng/mL. Many of these patients had no effective treatment options, since there was insufficient radioiodine accumulation in tumor tissue. Kelders et al. (28), who analyzed Tg-DT in nine patients with DTC revealed even shorter DT (median 148 days; range 16–382 days) due to the fact that their patient sample comprised mainly patients with high-risk profiles and/or radioiodine negative metastases.
In contrast, Miyauchi et al. (18) included not only patients with progressive diseases, but also those with stable and even declining Tg blood levels. They calculated Tg-DT in 137 patients with PTC, who had at least four Tg measurements under suppression of TSH. They selected the same method for Tg-DT calculation as the present study (log-slope method). As described above, the DT depends on the slope of the regression line plotted Tg measurements plotted semi-logarithmically. Using this method, falling Tg values would be interpreted as negative DT. Indeed, the study of Miyauchi et al. (18) contains 69 cases with negative Tg-DT. These patients obviously do not have progressive disease. To avoid this aspect, the present study deliberately included only patients with tumor progression. After excluding patients with negative DT, only 68 patients remained in Miyauchi et al.'s study (18). Among them, Tg-DT was three or more years in 26 cases (38.2%), between one year and less than three years in 22 cases (32.4%), and less than one year in 20 cases (29.4%). In contrast to the present study, the authors did not define whether their patients had progressive disease, which could have been proven by imaging modalities. Therefore, one can assume that the cohort with a DT of three or more years contains mostly patients with complete remission and stable disease, from which it can be concluded that only the remaining 42 cases are comparable to patients in the present study. Within the current cohort, 68% had a Tg-DT of less than one year, 28% between one year and less than three years, and only 4% three or more years.
Furthermore, Miyauchi et al. (18) included 253 patients without radioiodine therapy and postulated that postoperative measurable Tg levels indicate a high risk of recurrent disease. In the authors' opinion, this statement is hard to accept, since Tg is often present after thyroidectomy without adjuvant radioiodine treatment, and its diagnostic specificity increases with the radicalness of thyroid ablation.
Tg-DT as a survival predictor
There was no simple correlation between Tg-DT and survival including the total sample of 99 patients. Focusing exclusively on patients with progressive disease, the results from Miyauchi et al. (18), who showed that a Tg-DT of less than one year has a worse outcome than a Tg-DT of one to three years in general, could not be confirmed. These discrepancies are certainly due to the differences in the study protocols. In the multivariate analysis by Miyauchi et al. (18), the Tg-DT was found to be an independent prognostic parameter, where the 20 patients with a Tg-DT of less than one year were compared to the whole cohort of the remaining patients, including 69 patients with a negative Tg-DT. This leads to a stronger statistical weighting of the patients with shorter Tg-Dt compared with the present study.
Nevertheless, the analysis using the classification on the basis of quartiles showed the following tendency: the mortality risk of patients with a Tg-DT of less than five months was more than twice as high as the mortality risk of patients with a Tg-DT of >14 months. These findings are comparable to PSA-DT for patients with prostate cancer: PSA-DT of less than three months had been found to predict a worse outcome (higher mortality rate and higher probability of distant metastases) than a DT of >15 months (11).
However, it was not possible to confirm Tg-DT as an independent predictor for survival rate for all patients with progressive disease. Only in patients with Tg levels >100 ng/mL (regarded as surrogate parameter for high tumor load) were significant differences in survival rates found. A positive correlation between Tg level and tumor mass has been demonstrated. However, the range of the estimated tumor mass for a given Tg level is rather large, and various additional factors influence the Tg level (e.g., grade of tumor differentiation, stimulation of tumoral TSH receptors, and histological tumor type: in PTC, mean serum Tg is lower than it is in FTC) (29,30). The following example demonstrates that this is not really surprising: a patient with lymph node metastases and a short Tg-DT has a better chance of being cured (by surgical intervention) than a patient with disseminated visceral metastases and a longer Tg-DT. In this context, the authors agree with Elisei et al. (31), who postulated that the prognostic relevance of a short Tg-DT seems to be applicable mainly in patients with advanced tumors.
Wong et al. (32) analyzed the dynamic of unstimulated Tg values during the follow-up of 87 patients who had undergone curative thyroidectomy and subsequent radioiodine therapy because of PTC, and in whom at least one Tg value was >0.2 ng/mL (analytical sensitivity of the assay). In 29 of these patients, recurrences could be localized. The authors did not calculate the Tg-DT, but they analyzed the rate of Tg change (Tg velocity [TgV]), which was found to be an independent predictor of tumor recurrence. A TgV cutoff of 0.3 ng/mL/year (as determined by receiver operating characteristic analysis) predicted a recurrence with a sensitivity of 83% and a specificity of 94%, and TgV was proved to be a predictor for survival. However, the calculated TgV cutoff does not take into account the exponential course of Tg increase. Furthermore, one single absolute TgV cutoff is not appropriate for all ranges of Tg. In particular, it does not consider the potential of highly sensitive assays.
Compared to the DT of other tumor markers, a distinct cutoff value for Tg-DT, which was correlated with a significant worse outcome, could not be defined. Regarding medullary thyroid carcinoma, Meijer et al. (15) analyzed CEA- and calcitonin-DT, and determined a cutoff value of 12 months for both tumor markers, although the predictive value of CEA-DT was higher than that of calcitonin-DT. Giraudet et al. (27) analyzed the correlation between tumor progression (verified by morphologic criteria such as RECIST) and CEA-DT, and calculated a cutoff value of 24 months for long-term follow-up.
In the context of Tg-DT in DTC, Giovanella et al. (33) compared 18F-FDG-PET/CT (FDG) scans, Tg levels, and Tg-DT in patients with biochemical recurrence. The authors described a high rate of true positive FDG scans when the Tg-DT was less than one year or Tg levels were >5.5 ng/mL. They postulated that the Tg-DT might be of special interest in patients with dedifferentiated thyroid cancer and a low Tg level. Because the cutoff was arbitrarily selected, the authors conceded that further studies are needed to confirm their findings. In a comparable study, Kelders et al. (28) showed that Tg-DT is positively correlated with FDG-positive and iodine-negative metastases. Thus, Tg-DT might be a criterion in selecting patients for FDG as primary imaging modality.
Distribution of Tg-DT for both highly sensitive and routine assays
There were no significant differences between the Tg-DT calculated based on the highly sensitive Tg-measurements (second-generation assay) or with Tg measurements obtained with a routine first-generation assay. This finding provides evidence for the hypothesis that the dynamics of highly sensitive Tg measurement reflect the tumor progression in the early stages of tumor recurrence, which is comparable with the dynamics of high Tg levels in patients with advanced tumors, and it confirms the validity of the highly sensitive IEMA. Thus, rising Tg levels measured by highly sensitive assays reflect tumor growth, even when it might not (yet) be localized by imaging modalities. Figure 4 shows the course of Tg values from patients with recurrent DTC, in which the measurements were performed with the highly sensitive assay.

Representative Tg courses from highly sensitive Tg measurements. In all cases, recurrences finally could be localized. The Tg-DT does not depend on the site of the recurrence (locoregional or distant metastases). The Tg increase is often objectified already in “subclinical” stages.
Footnotes
Author Disclosure Statement
No competing financial interests exist.