
Abstract
Background:
Metastatic deposits to the spine in thyroid cancer patients represent the most common site of bone involvement and can contribute to pain, neurologic deficits, and death. This study sought to determine the efficacy and safety of spine stereotactic radiosurgery (SSRS) for thyroid cancer patients.
Methods:
Thyroid cancer patients with spine metastases were selected and analyzed from a cohort of patients who were prospectively enrolled in two single-institution Phase I/II studies. SSRS was delivered in single or multi-fraction schedules. Dose regimens ranged from 16–18 Gy in one fraction to 27–30 Gy in three to five fractions. Toxicity was graded according to the NCI-CTC toxicity scale. Local control was determined by serial post-treatment magnetic resonance imaging scans showing no evidence of progressive disease. Patients were followed until date of death or date of last known visit for survival analyses. Local control and overall survival rates were carried out using Kaplan–Meier estimates. The log-rank test was used to assess the equality of the survivor function across groups. A p-value of ≤0.05 was considered to be statistically significant.
Results:
A total of 27 spine lesions were treated in 23 patients over a six-year period. Median follow-up was 28.9 months (range 5–93 months). Local control was 88% at two years and 79% at three years. In patients with progressive disease following conventional radiation therapy, local control for salvage SSRS remained at 88% at three years. Patients requiring upfront surgical intervention and treated with adjuvant SSRS achieved sustained control rates of 86% at three years. Overall survival rates were 85% and 67% at one and two years, respectively. In patients classified with oligoprogression and controlled extra-spinal disease, overall survival was significantly higher than those with evidence of systemic progression (81% vs. 45% at two years; p = 0.01). Univariate analysis did not show significant correlations between local control and age, systemic disease status, prior 131I therapy, SSRS fraction regimen, spine location, histological subtype, or time from initial diagnosis to evidence of spinal metastasis. No patient experienced any grade 3–5 toxicity. Pain flare was reported in 30% of patients, with only three patients (13%) requiring narcotics or short-course steroids. There was no evidence of vertebral body fracture in any patient that achieved local control in the treated area.
Conclusions:
SSRS for thyroid metastases as a primary or adjuvant/salvage therapy is well tolerated and yields high rates of local control.
Introduction
A
For patients diagnosed with spine metastases, several treatment options exist for the management of local disease, including steroids, conventional radiotherapy, surgical intervention, or a combination of these therapies (9). Surgery is often reserved for patients who present with acute neurologic injury requiring decompression or spine stabilization. Previously, for non-surgical candidates, conventional radiotherapy was the treatment of choice. However, due to the proximity of the spinal cord and its low radiation tolerance, the dose prescribed to the lesion was frequently below ablative value (9,10). Recent advances in radiation therapy with stereotactic body radiation therapy allow for higher doses of radiation to be delivered to targets in close proximity to critical organs. Spine stereotactic radiosurgery (SSRS), sometimes referred to as stereotactic ablative radiotherapy, has been recently adopted to treat metastatic disease near the spinal cord. It achieves a high level of conformality around the target, with a steep dose fall-off, thereby sparing surrounding organs at risk. Several studies have reported local control rates >80% using SSRS to treat metastatic disease from various primary tumor types (11,12). However, as mentioned in a recent review by Kushchayeva et al., there are no studies devoted to assessing the efficacy of SSRS on thyroid spinal metastases only (4).
This study presents the authors' experience of SSRS in thyroid cancer patients diagnosed with spinal metastases. The outcomes of patients who were enrolled in two prospective clinical trials designed to determine the efficacy and tolerability of this treatment modality are analyzed.
Materials and Methods
Patients with evidence of spine metastases from solid malignancies were prospectively enrolled in two clinical trials initiating in 2004. Prior to enrollment, patients were adequately screened to ensure eligibility, and appropriate informed consent was obtained. Both were single-institution Phase I/II trials, one evaluating multifraction SSRS, as the technology was initially adopted, for the treatment of metastatic spine disease, and the other investigating single-session SSRS for previously unirradiated spinal or paraspinal metastases. For the purpose of this study, patients with primary thyroid cancer were selected from the cohort, and their outcomes analyzed. The trials had similar inclusion criteria, enrolling patients with radiographically documented spine or paraspinal metastases on spine magnetic resonance imaging (MRI) within four weeks of registration; a maximum of two metastatic sites to be irradiated with stereotactic technique with one to five fractions; diagnosis of cancer including but not limited to lung, breast, prostate, renal cell, thyroid, melanoma, and unknown primary tumors; and a Karnofsky performance status of at least 40. Patients were excluded from the initial studies if they presented with worsening neurological status due to radiographic evidence of spinal-cord compression requiring immediate surgical decompression or emergent conventional external beam radiotherapy. Additionally, patients were excluded if prior irradiation of the site was within three months of registration or if the prior course of radiation exceeded maximum cord tolerance of 45 Gy in five weeks conventional fractionation. Finally, patients with cervical spine metastases were not eligible to receive single-fraction SSRS.
Upon enrollment, patients underwent a complete history and neurological examination. A pretreatment computed tomography (CT) scan was obtained for planning and was fused with the spine MRI for appropriate target delineation. Treatment was conducted with a near-simultaneous CT, image-guides SSRS, intensity-modulated technique as previously described (13). Patients were immobilized with a stereotactic body-frame system comprised of a whole-body vacuum cushion, vacuum system, and plastic fixation sheet. Treatment planning for SSRS was performed with inverse-planning intensity-modulated radiation therapy (IMRT) software (Pinnacle; Phillips Medical Systems). All patients received IMRT to maximize conformality to the tumor while attempting to spare the spinal cord. For both single and multi-fraction SSRS, a simultaneous integrated boost technique was employed. The gross tumor volume (GTV) was defined as the gross tumor present on the most recent pretreatment MRI scan. The clinical target volume consisted of an at-risk region of continuous bone marrow or soft-tissue margin for patients with evidence of paraspinal disease. Mean GTV was prescribed to receive prescription dose with at least 90% coverage while respecting spinal-cord tolerance. Patients received either single fraction SSRS to a total dose of 16–18 Gy or three fractions at a dose of 9 Gy each so that a peripheral dose of 27 Gy was delivered to the tumor. Of note, one patient included in the study was treated in five fractions to a total dose of 30 Gy. A representative single-fraction SSRS plan is detailed in Figure 1. Per the protocol for single-fraction treatment, the dose to the spinal cord was limited to 8 Gy, and the spinal cord plus an additional 2 mm margin was not permitted to exceed 12 Gy. No more than 0.01 cc of the spinal cord received 10 Gy based on tabular dose volume histogram (DVH). For multi-fraction SSRS, the maximum allowable dose to any portion of the spinal cord was 9 Gy in three fractions to permit future irradiation. Patients with prior irradiation of the area to be treated were also permitted to receive a maximum allowable additional dose of no more than 9 Gy in three fractions to the spinal cord. Treatments were separated by a minimum of 48 hours. Patients were evaluated at two and four weeks, and at two months following completion of the radiation treatment. Patients were then seen for follow-up with MRI imaging at 3, 6, 9, 12, 18, and 24 months and then every six months thereafter.

The left panel details a spine stereotactic radiosurgery (SSRS) plan in axial view. The bold isodose line representing 16 Gy, the prescription dose, encompasses the involved vertebral body with superior conformality compared with conventional forms of radiotherapy. Additional isodose curves and their respective doses are shown in the top left corner. The right panel shows the sagittal view of a patient treated to two separate vertebral bodies utilizing SSRS.
Biological equivalent dose (BED), a historical method developed to compare different radiation fractionation schemes, was calculated for each fraction scheme with an α/β ratio assumed to be 10, according to the following equation: BED10 = (prescription dose) × [1 + (dose per fraction/α/β)].
Toxicity monitoring was focused on neurological, gastrointestinal, musculoskeletal, hematologic, and dermatologic systems. Toxicity was graded according to the National Cancer Institute Common Toxicity Criteria v2.0 toxicity scale performed at each visit. Dosimetric data regarding maximum doses to the spinal cord and cauda equina as well as target coverage, including the volume of the target receiving at least 95% of the prescription dose (V95) and the dose delivered to 95% of the target (D95), were extracted directly from individual DVHs.
Tumor control was based on spinal MRI showing absence of progression. Treatment failures were defined by radiographic assessment. Data were collected on the treated lesions and classified as “progressive” defined as larger in volume, “stable2 defined as radiographically unchanged, or “smaller.” When provided, exact differences in measurement of each dimension—x, y, z, or right-left, anterior-posterior, medial-lateral—were utilized to determine response. If initially inconclusive, review with the radiologist decided final disease status by thorough comparison of the prior and current studies.
Statistical analyses were performed using Stata/MP v14.0 statistical software (StataCorp, College Station, TX). Fisher's exact test was used to assess measures of association in frequency tables with the equality of group medians assessed using nonparametric tests for equality. The survival function was carried out using Kaplan–Meier estimates. The log-rank test was used to assess the equality of the survivor function across groups. A p-value of ≤0.05 was considered to be statistically significant. Statistical tests were based on a two-sided significance level. Overall survival was defined as the time between the date of SSRS and death from any cause. Local failure was defined as the time between SSRS date and MRI evidence of progression. Cox's proportional hazard model was used for univariate analysis to assess the effect of patient, tumor, and other predictors of significance on the endpoints. Although not pre-specified, the factors chosen for univariate analyses were based on their potential significance as reported in the literature and appropriate statistical corrections conducted. The estimated hazard is reported.
Results
Patient characteristics
The baseline characteristics of the patients included in the study are outlined in Table 1. A total of 27 lesions in 23 patients were treated with SSRS between 2004 and 2010. Among the 23 patients, 43% were women. The median age of this cohort at the time of SSRS treatment was 58.4 years for all patient years (range 33.4–79.4 years). In terms of primary histological classification, 39% of patients presented with papillary thyroid cancer, 26% with follicular, 17% with Hürthle cell, and 17% with medullary thyroid carcinoma. The mean BED of SSRS was 49.9 Gy–1 (range 48–51.3) delivered in one, three, or five fractions. The follow-up duration of the study ranged from 5 to 93 months (median 28.9 months). Of note, spinal metastasis was the only site of distant disease in one patient (Table 1).
KPS, Karnofsky performance status; SSRS, spine stereotactic radiosurgery; Gy, Gray; fx, fraction.
Local control
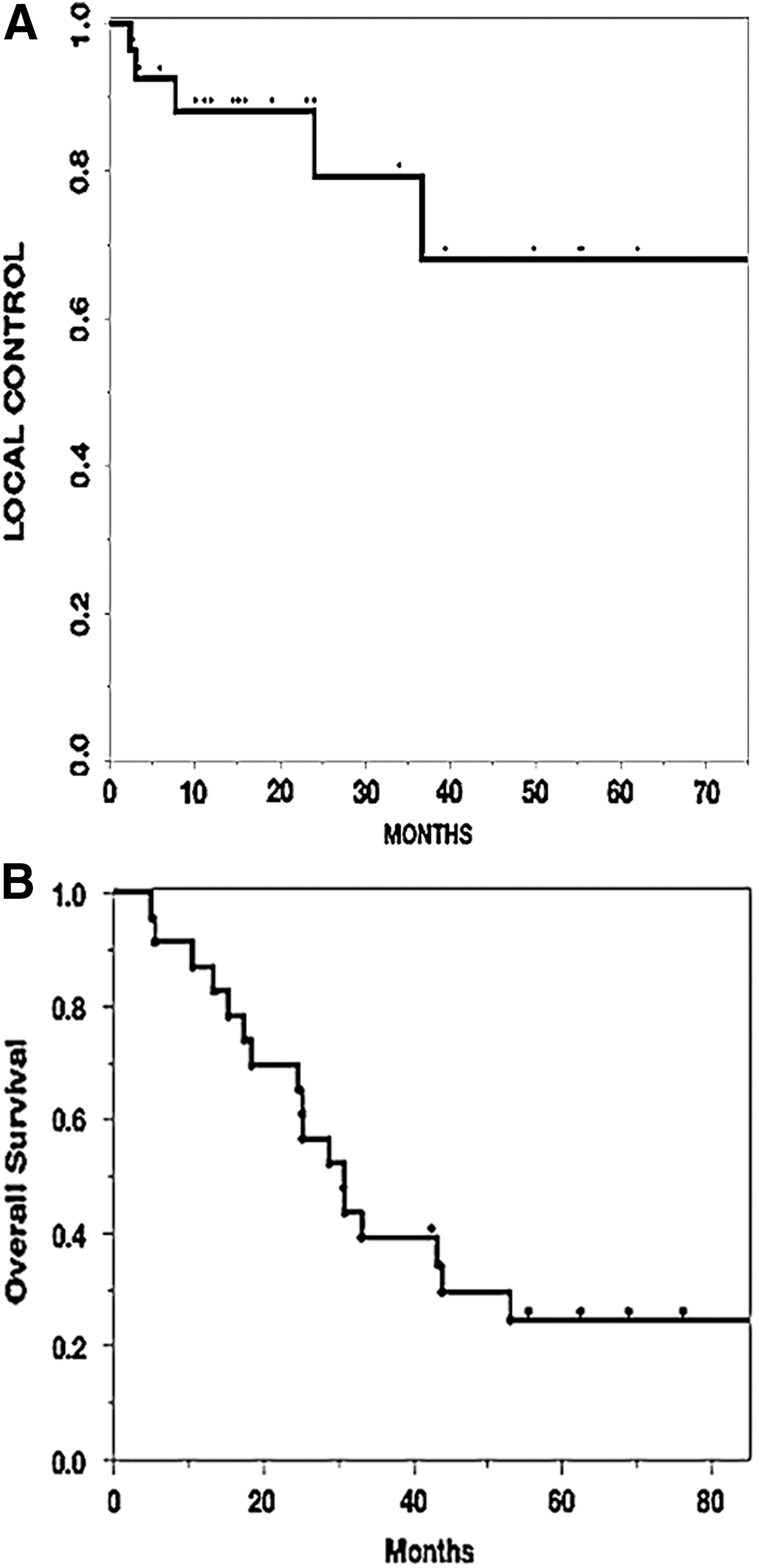
Following completion of the study, five sites treated with SSRS failed therapy as defined by radiographic progression on MRI. These results translated into local control rates of 88% at two years, and 79% at three years (Fig. 2A). In the eight metastases that were previously treated with conventional fractionation, one showed evidence of further progression. Similarly, at the eight sites that had undergone prior surgical intervention, only one failed to be controlled with adjuvant or salvage SSRS. In addition, as a potential surrogate for disease aggressiveness, time from initial diagnosis to evidence of spinal metastasis was recorded. Despite these patients presenting with distant disease, local control at these sites remained 80% at one year. Univariate analysis was performed to determine patient or treatment characteristics that predicted local failure. As shown in Table 2, there was no significant correlation between SSRS failure and sex, age at time of SSRS, prior therapy (radiation and/or surgery), prior 131I therapy, single or multi-fraction therapy, BED, histologic subtype, time from initial diagnosis to evidence of spine metastases, or spine location. Specific characteristics of the five failures are further detailed in Table 3.
(
RT, radiation therapy; HR, hazard ratio; CI, confidence interval; BED, biological equivalent dose.
GTV, gross tumor volume; D95, dose delivered to 95% of the target volume; V95, volume of the target receiving at least 95% of the prescription dose; EP, epidural; VB, vertebral body; PS, paraspinal; PE, posterior elements; IF, in-field recurrence; MP, marginal recurrence in paravertebral soft tissue; ME, marginal recurrence in epidural space.
Overall survival
The median survival time for all study patients was 28.9 months. The actuarial 12- and 24-month survival was 85% and 67%, respectively (Fig. 2B). Of the 23 patients, 18 died, with a median time to death from SSRS treatment of 25.3 months (range 5–93 months). To determine the status of disease burden, patients were recorded as having oligoprogression, defined as radiographic evidence of stable disease at all other extra-spinal metastatic sites. In patients with controlled extra-spinal disease, there was a statistically significant improvement in survival compared with those with evidence of active disease at extra-spinal metastatic sites (p < 0.01; Fig. 3). Univariate analysis detailing factors predicting for overall survival is shown in Table 4.
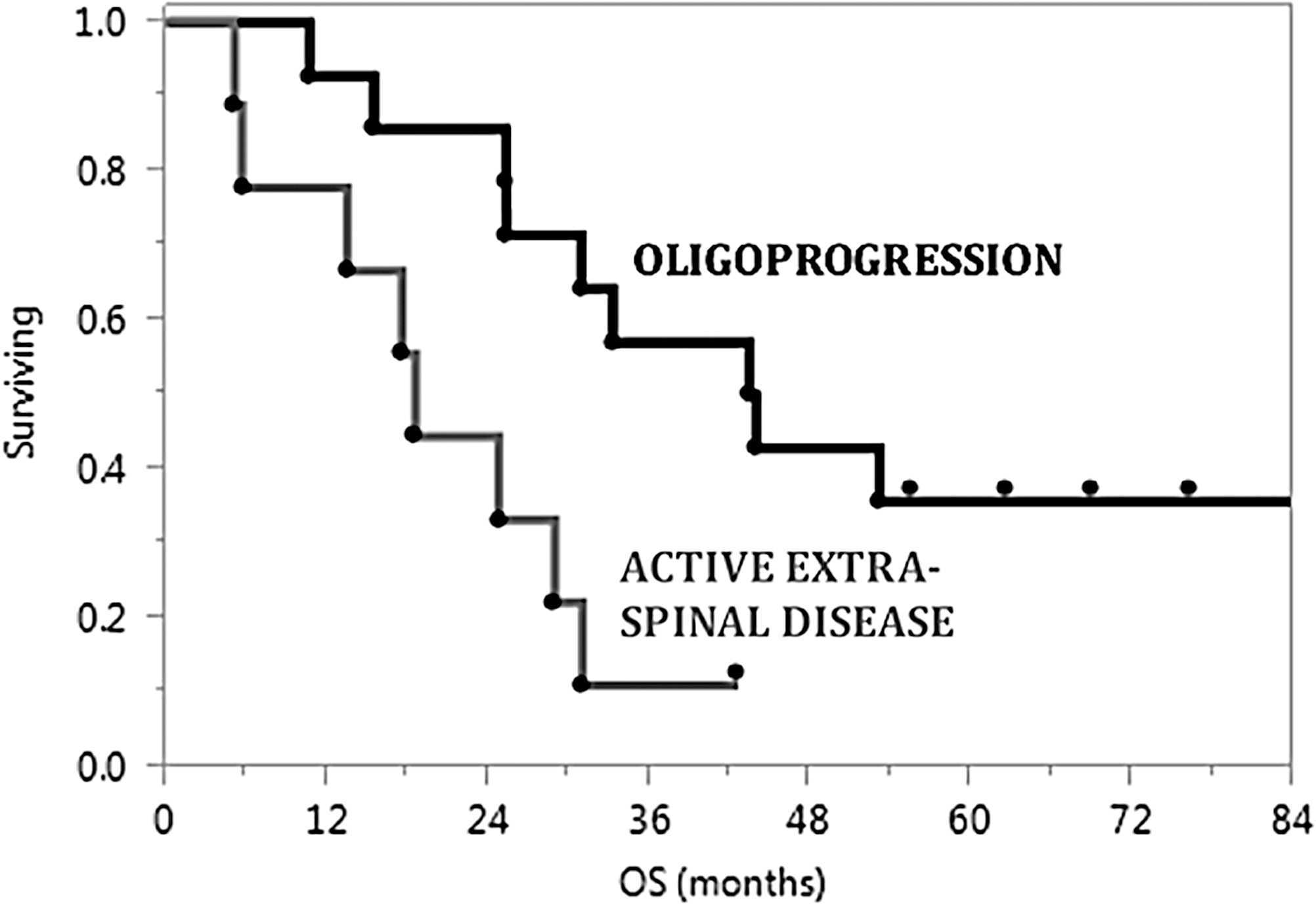
Kaplan–Meier plot detailing overall survival in patients with oligoprogression of spinal metastases only compared with patients suffering from active extra-spinal disease. Censored subjects are represented by filled black dots. In patients with controlled extra-spinal disease, there was a statistically significant improvement in survival compared with those with evidence of active disease at extra-spinal metastatic sites (p < 0.01).
Dosimetry
As shown in Table 1, patients were treated with either single or multi-fraction SSRS. The mean maximum dose to the spinal cord and cauda equina for single fraction treatment was 12.1 Gy and 13.8 Gy, respectively. For multi-fraction SSRS, the mean maximum dose to the spinal cord and cauda equina was 10.1 Gy and 12.8 Gy, respectively. Optimal coverage was achieved in all patients, despite proximity to the spinal cord and other critical structures. The median percentage of the target volume receiving at least 95% of the prescribed dose was 100% for single fraction and 94% for multi-fraction SSRS. The median percentage of the prescribed dose delivered to 95% of the target volume was 100.8% for single fraction SSRS and 91% for multi-fraction therapy.
Toxicity
No patient experienced clinical or radiographic evidence of myelopathy or radiculopathy following SSRS therapy. There were no reported events of grade 3–5 toxicity for any patient at time of death or last known follow-up. Pain flare, defined by a temporary increase in pain in the immediate period after radiation, was observed in seven (30%) patients. Only three (13%) patients required conservative management with narcotics or short-course steroids. Lastly, another potential concern with SSRS is the occurrence of vertebral body fractures. In the present cohort, only two patients had evidence of vertebral body fracture on follow-up MRI exam. However, both patients were also diagnosed simultaneous progression of disease, contributing to the documentation of pathologic compression fracture. In patients who achieved local control following SSRS, none experienced vertebral body fracture in the treated field.
Discussion
The overall prognosis for most patients diagnosed with thyroid cancer is excellent, with 10-year survival rates of 93%, 85%, and 76% for patients with papillary, follicular, and Hürthle cell carcinoma, respectively (14). Even patients who eventually develop metastatic disease have reported 10-year overall survival rates of nearly 40% (15 –17). Therefore, as these patients can experience long and indolent disease courses, aggressive palliation at metastatic sites to delay significant declines in quality of life is warranted.
Bone metastases are a frequent site of distant disease, with one study reporting rates as high as 44% (18). Previously, patients receiving radiation therapy for spinal metastases were treated with conventional fractionation encompassing one or more vertebral bodies above and below the area of involvement. However, the allowable dose to treat these lesions was limited due to spinal cord tolerance. More recently, technological advances utilizing stereotactic techniques enable the delivery of a high dose of focused radiation to the lesion while sparing the surrounding organs at risk. Several studies have shown safety and efficacy with the use of SSRS to treat spinal metastases. In one of the earliest and largest studies of SSRS, Gerszten et al. reported nearly 90% long-term tumor control with SSRS as the primary modality of therapy or as salvage treatment for progression (19). Of the 500 patients in this report, only 11 had a diagnosis of primary thyroid carcinoma, although specific tumor control in this cohort was not stated. To the authors' knowledge, this study is the first report documenting outcomes of SSRS solely focused on spinal metastases in thyroid cancer patients.
Patients included in this analysis were enrolled in two trials investigating the safety and efficacy of SSRS and prospectively followed. Consistent with previously published data (20 –23), the results show excellent local control rates of nearly 90% for the entire cohort at two years (Fig. 2A). As a primary treatment modality, SSRS resulted in control rates of 92% and 80% at one and two years, respectively. Additionally, when SSRS was utilized for progressive disease following surgery or conventional fractionation, local control rates remained at 82% at two years. Taken together, these results show that SSRS for spinal-cord metastases in patients with thyroid cancer is not only effective as upfront therapy, but also in the setting when other therapies fail. As a potential surrogate for disease aggressiveness, the time from initial diagnosis of thyroid cancer to evidence of spinal metastasis was documented. In this study, five patients had spinal metastases as their initial presentation of thyroid cancer. Despite these patients presenting with distant disease, local control at these sites was at 80% at one year.
Although there were few events in this study, a univariate analysis was performed to determine patient or treatment characteristics that may predict local failure. There was no significant correlation between recurrence and sex, age at time of SSRS, prior therapy (radiation and/or surgery), single or multi-fraction therapy, BED, histologic subtype, time from initial diagnosis to evidence of spine metastases, prior 131I therapy, or spine location (Table 2).
Since there were no significant factors that predicted recurrence, a closer look was taken at the specific characteristics of the five treatment failures. As shown in Table 3, all five lesions that progressed after SSRS had an element of epidural extension on post-therapy MRI scans. However, due to the proximity to the spinal cord, escalating the dose of SSRS while satisfying cord constraints and maintaining adequate coverage poses significant challenges. To address these situations, patients were enrolled in two Phase I clinical trials to establish the feasibility of SSRS in the primary management of inoperable metastatic epidural spinal-cord compression in previously unirradiated or irradiated patients (NCT01254903, NCT01256554). SSRS was delivered in a single fraction to total doses of either 18 or 24 Gy.
Studies have shown that patients with spinal metastases from thyroid cancer have improved survival compared with those with spine involvement from other primary histologies. One report states an average survival of 33 months for thyroid cancer patients versus seven months for patients with metastases from other primary tumors (6 –8). The median overall survival in the present study was nearly 30 months (Fig. 2B), which is comparable to these prior data. It has also been documented that patients with spine-only metastases have significantly higher survival rates than patients with evidence of solid organ involvement have (24). Consistent with this report, patients in this study with oligoprogression had significantly improved overall survival compared with those with active extra-spinal metastases (Fig. 3).
An additional issue worth noting is the role of systemic therapy in reported outcomes. A previous study detailed enhanced inhibition of bone disease with the combination of radiation and bisphosphonates compared with either modality alone (25). In the present cohort, only two (8%) patients received bisphosphonates during the course of SSRS. Additionally, no patient received receptor activator of nuclear factor kappa-B ligand (RANKL) agonist therapy, which has been shown to decrease bone turnover and increase bone mineral density (26). Therefore, it is unlikely that systemic treatment significantly contributed to the efficacy of SSRS in this study.
No patient in this study experienced any clinical or radiographic signs of neurologic toxicity. SSRS was well tolerated, with no reports of radiation myelitis, radiculopathy, or late signs of myelopathy at time of death or last available follow-up. Additional concerns regarding SSRS toxicity include the development of a pain flare or vertebral body fracture. One prospective study reported pain flare rates as high as 68% following SSRS (27). In a more recent secondary analysis at the authors' institution, the incidence of pain flare was 23% (28). In the present cohort of metastatic thyroid patients, 30% had documented pain flare events, with only three patients requiring conservative management. Lastly, no patient in this study who achieved local control showed evidence of vertebral body fracture on post-treatment MRI scans. In the two patients who had reported fractures, both were associated with locally progressive disease as well.
In summary, SSRS is the preferred modality of therapy over conventional radiotherapy for spinal metastases in many clinical scenarios. It delivers a highly conformal dose of radiation to the target, with a steep dose gradient to spare neighboring critical structures. A review by Sahgal et al. summarized the results of several reports detailing excellent local controls and minimal toxicity with SSRS (21). However, these studies included a heterogeneous patient population in terms of primary tumor type. To the authors' knowledge, this study is the first to report on SSRS outcomes for thyroid cancer patients only. The findings are consistent with prior reports and confirm that SSRS is a safe and effective therapy for patients with spinal metastases from primary thyroid cancer, with acceptable toxicity profiles and high rates of disease control.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to disclose.