
Abstract
Background:
Anaplastic thyroid cancer (ATC) is a rare and extremely aggressive malignancy, with a median survival of less than 6 months due to rapid progression and resistance to multimodal therapies. Effective treatment strategies have not been identified. A prospective clinical study was performed to objectively evaluate outcomes of treatment with paclitaxel.
Methods:
An investigator-initiated, multicenter, nonrandomized, open-label, single-arm study to evaluate the feasibility and efficacy of weekly paclitaxel (80 mg/m2) administration for patients with pathologically confirmed ATC was conducted in a nationwide organization.
Results:
Feasibility was analyzed in 56 patients. More than one course of treatment was performed in 52 (93%) patients retaining sufficient dose intensity (>84%). No patient had to terminate the treatment because of an adverse event. The median overall survival was 6.7 months [confidence interval 4.4–9.0]. The 6-month survival was 54%. Among the 42 patients with an evaluable lesion, none demonstrated complete remission, 9 (21%) showed partial remission, 22 (52%) achieved stable disease, and 8 (19%) exhibited progressive disease; 3 did not complete the initial treatment course. The objective response rate was 21%, and the clinical benefit rate was 73%. The median time to progression was 1.6 months. Statistically, no additional effect of concomitant radiation was demonstrated in 6 patients receiving combined therapy. Eight patients, in whom a complete post-treatment surgical removal of the tumor was feasible, survived significantly longer (median 7.6 months [CI 8.1–23.0]) than the other 34 patients in whom the tumor could not be completely removed after chemotherapy (5.4 months [CI 3.0–7.8], p = 0.018).
Summary:
The study demonstrates objective and accurate information concerning the feasibility and efficacy of a standardized treatment with weekly paclitaxel administration for ATC patients.
Conclusions:
Weekly paclitaxel administration for ATC patients can be of clinical benefit in a neo-adjuvant setting.
Introduction
A
We have established a nationwide research organization, the Anaplastic Thyroid Carcinoma Research Consortium of Japan (ATCCJ), and we assembled the available clinical information into a large database including over a thousand patients with ATC. According to the obtained data, approximately 40% of patients already have invasive disease that has spread to adjacent organs, and another 40% of patients have demonstrated disease dissemination to distant organ(s) at the initial presentation before the initiation of treatment (8). Systemic chemotherapy is therefore indicated in most ATC patients. Several strategies have been employed to control the disease, but conventional chemotherapeutic treatment using doxorubicin or cisplatin did not demonstrate any significant effect (1,9). More recent studies have suggested a potential benefit of taxanes to control advanced disease (10 –12), but these small studies used different protocols, and there is currently no reliable objective information concerning the outcomes of a practical standardized treatment plan for ATC patients.
The members of the ATCCJ have addressed this critical situation and planned an investigator-initiated prospective clinical study to determine the present status of the outcomes of a frequently used chemotherapy protocol for patients with ATC (13).
Methods and Patients
Patients
The details of the study's concept and protocol have been reported (13). Patients with clinically diagnosed ATC, aged 20 years or older were eligible for this study, if they met the following criteria: Eastern Cooperative Oncology Group performance status of 0 to 2—adequate bone marrow, hepatic, and renal function. The major exclusion criteria included previous chemotherapy or radiation therapy for ATC (Supplementary Table S1; Supplementary Data are available online at
The study protocol was approved by the institutional review board of Osaka City University Medical School in March 2012 (#2248), and then the study was approved by the institutional review board at each of the participating institutions (Supplementary Table S2). The study was performed in accordance with the Declaration of Helsinki. This trial is registered on the clinical trials site of the University Hospital Medical Information Network Clinical Trials Registry Website (UMIN 000008574). All patients were evaluated and treated at the institutions at which they were registered after obtaining written informed consent.
The initial pathology-based diagnoses were made by local pathologists. A central pathology review board was held after the termination of recruitment, by accumulating the tissue specimens from each institution. Three pathologists (described in Acknowledgments) who specialize in this field gathered and reviewed every sample to confirm the ATC diagnosis. Confirmation of the pathological diagnosis of ATC was made when all three members agreed. Patients without pathological review data were excluded from final analysis.
Study oversight
The present study was an investigator-initiated, multicenter, nonrandomized, open-label, single-arm, phase 2 clinical trial to prospectively evaluate the feasibility and efficacy of chemotherapy with weekly paclitaxel administration for patients with ATC (13). The enrolled patients received chemotherapy with a weekly paclitaxel administration [80 mg/m2, once every week (12)]. One course consisted of three paclitaxel administrations (Fig. 1). At least one course of therapy was necessary for each patient. The therapy was continued until the appearance of disease progression or until the time when the patient's physician decided to terminate the protocol. The dose was reduced to 30 mg/m2 when concomitant extra-beam radiation therapy (EBRT) was conducted.
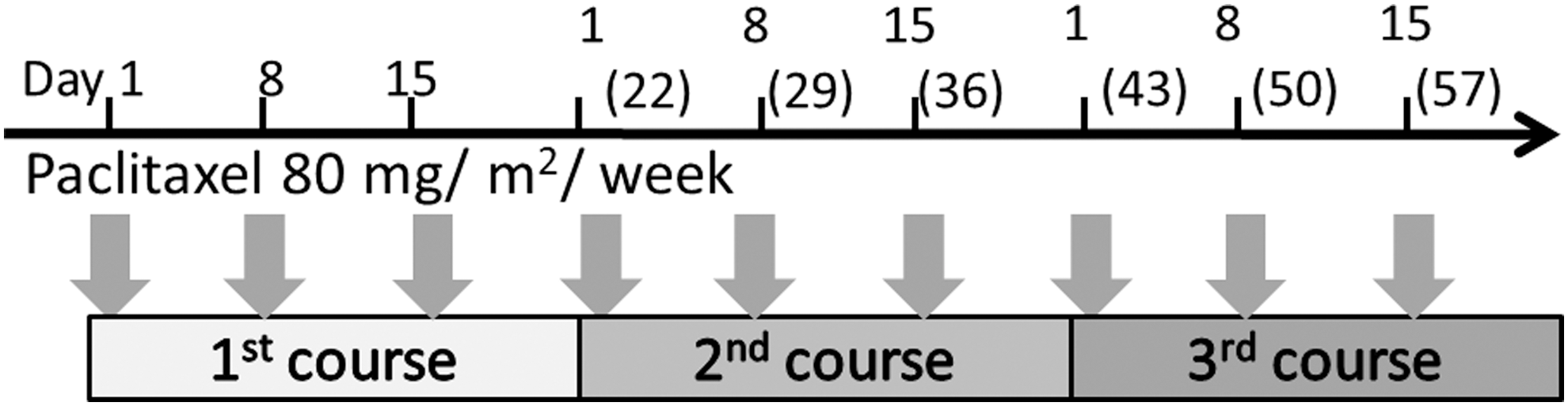
The schedule of weekly paclitaxel administration (80 mg/m2).
For the evaluation of the treatment's feasibility and safety, we analyzed the relative dose intensity (RDI) and the occurrence of treatment-related adverse events (AE). AEs were reported and graded according to Common Terminology Criteria for Adverse Events v4.0 (15). The RDI was calculated by the following equation:
For the analysis of the treatment's efficacy, we determined the overall survival (OS) of all pathologically confirmed ATC patients. The overall response rate, time to progression, and time to treatment failure were evaluated in the patients with RECIST (14)-defined target lesion. The assessments were performed at baseline and every 3 weeks during treatment by computed tomography, and each patient's outcome was classified as a complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The clinical response (CR, PR, or SD) had to be confirmed at least 3 weeks after it was first noted (13).
Initially, 50 patients were set as the target population. This sample size was estimated to be able to provide an evaluation of possible survival benefit. The protocol was then modified to include as many patients as possible until the study period closed (details were described in a previous report) (13). Survival curves are illustrated by the Kaplan-Meier method, and the log-rank test was used to compare the differences in survival. A p-value of <0.05 was considered significant. The statistical analyses were performed using SPSS 13.0 statistical software (SPSS, Chicago, IL).
Results
Subjects
Between April 26, 2012, and March 24, 2014, a total of 71 patients from 14 institutions were enrolled. One patient could not be treated because of the progression of the disease during the evaluation period. The diagnosis of four patients was corrected as disease other than ATC after enrollment. A total of 66 patients thus formed the intended-to-treat series with the study regimen. Specimens for pathological review could not be obtained for four patients, and the remaining 62 patients were evaluated by the central pathology review board, which determined that five patients had thyroid cancers other than ATC. Therefore, 92% of the pathological diagnoses at the local referral institutions were revealed to be correct after the central review. The final follow-up data could not be obtained for 1 patient. Thus, 56 patients (40 females and 16 males) treated with the study protocol were included in the feasibility and survival analysis. Among these 56 patients, 42 had RECIST (14)-defined target lesion, and these cases form the cohort for the efficacy analysis (Fig. 2). The baseline characteristics of the patients are summarized in Table 1.
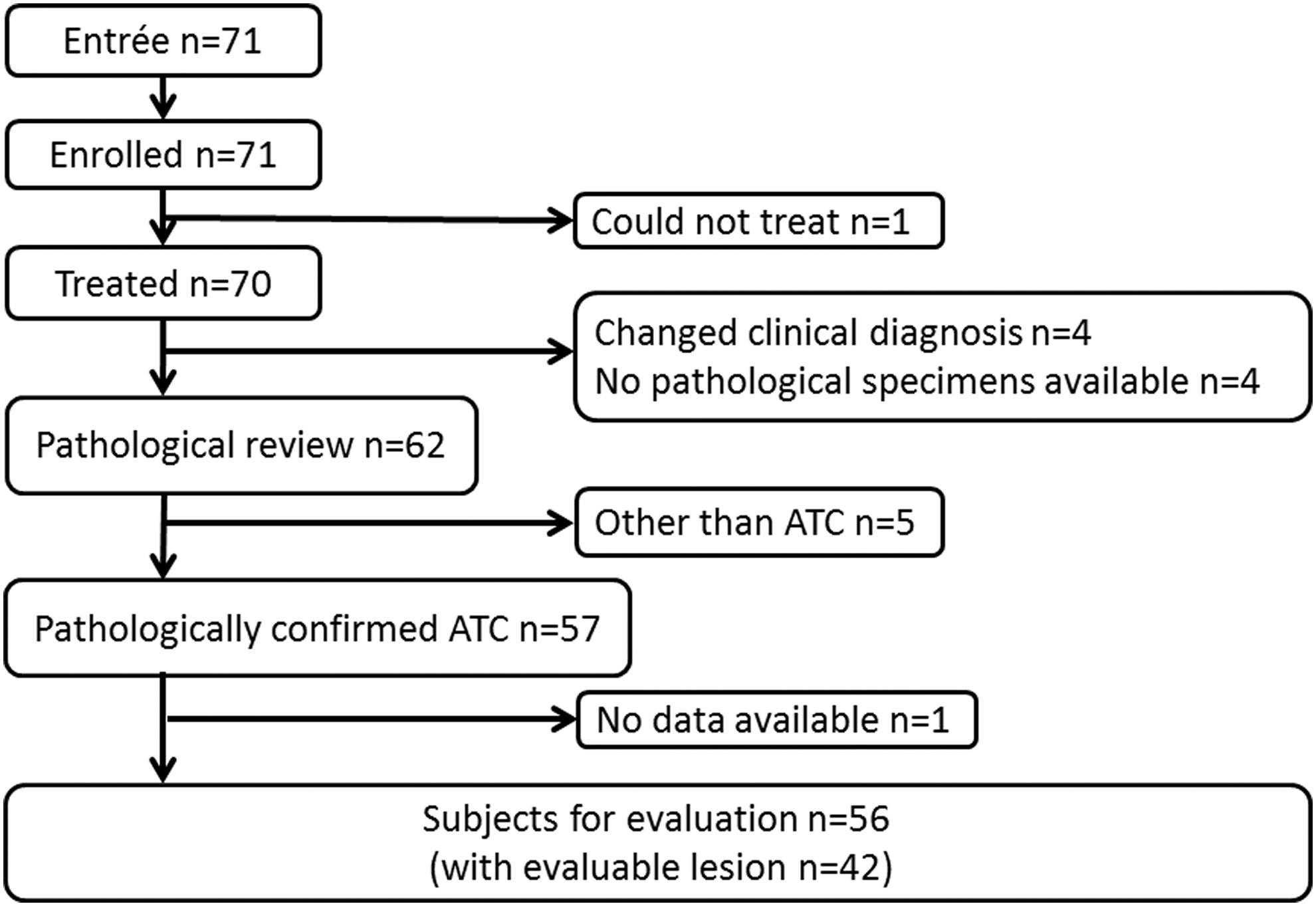
Cohort diagram. ATC, anaplastic thyroid cancer.
Feasibility assessment
Fifty-two of the 56 patients (92.9%) were successfully treated with more than one course of the protocol. Four patients could not complete a single course of treatment because of complete atrioventricular block (one case), rapid progression of the disease (one case), or patient refusal (two cases). Two to 69 administrations of paclitaxel (0 to 23 courses) were conducted with a median number of six administrations (2 courses). The protocol treatment had to be postponed in 29 patients: in 12 patients during the first course, 11 patients during their second course, 1 patient in the third course, 2 during the fourth course, 1 during the fifth course, and 2 patients during a later course of the treatment. The median time to treatment failure was 1.6 months [confidence interval (CI) 0.9–2.3]. The RDI in every course is shown in Supplementary Table S3. The average RDI of more than 80% could be maintained during the initial two courses of the treatment.
No death or severe AE occurring during the treatment was reported. The AEs that were reported are listed in Table 2. A total of 55 patients (98.2%) had at least one treatment-related AE during the protocol treatment. The most commonly reported AEs of all grades were anemia (76.8%) and alopecia (67.9%). AEs of grade 3 or higher were observed in 16 patients (28.6%); these included neutropenia (10.7%), leukocytopenia (8.9%), dyspnea (7.1%), anemia (5.4%), rash (3.6%), liver dysfunction (1.8%), fever (1.8%), mucositis (1.8%), peripheral neuropathy (1.8%), hypercalcemia (1.8%), and complete atrioventricular block (1.8%).
Efficacy assessment
Forty-four patients died (43 died of disease and one in an accident), and 11 patients remained alive for 15.3–26.3 months with a median of 16.1 months at the time of the data cutoff. The median OS of all 56 ATC patients was 6.7 months [CI 4.4–9.0] (Fig. 3). The 3-, 6-, and 12-month OS rates were 71.4%, 53.6%, and 26.8%, respectively. The median cause-specific survival was 6.7 months [CI 4.1–9.3].
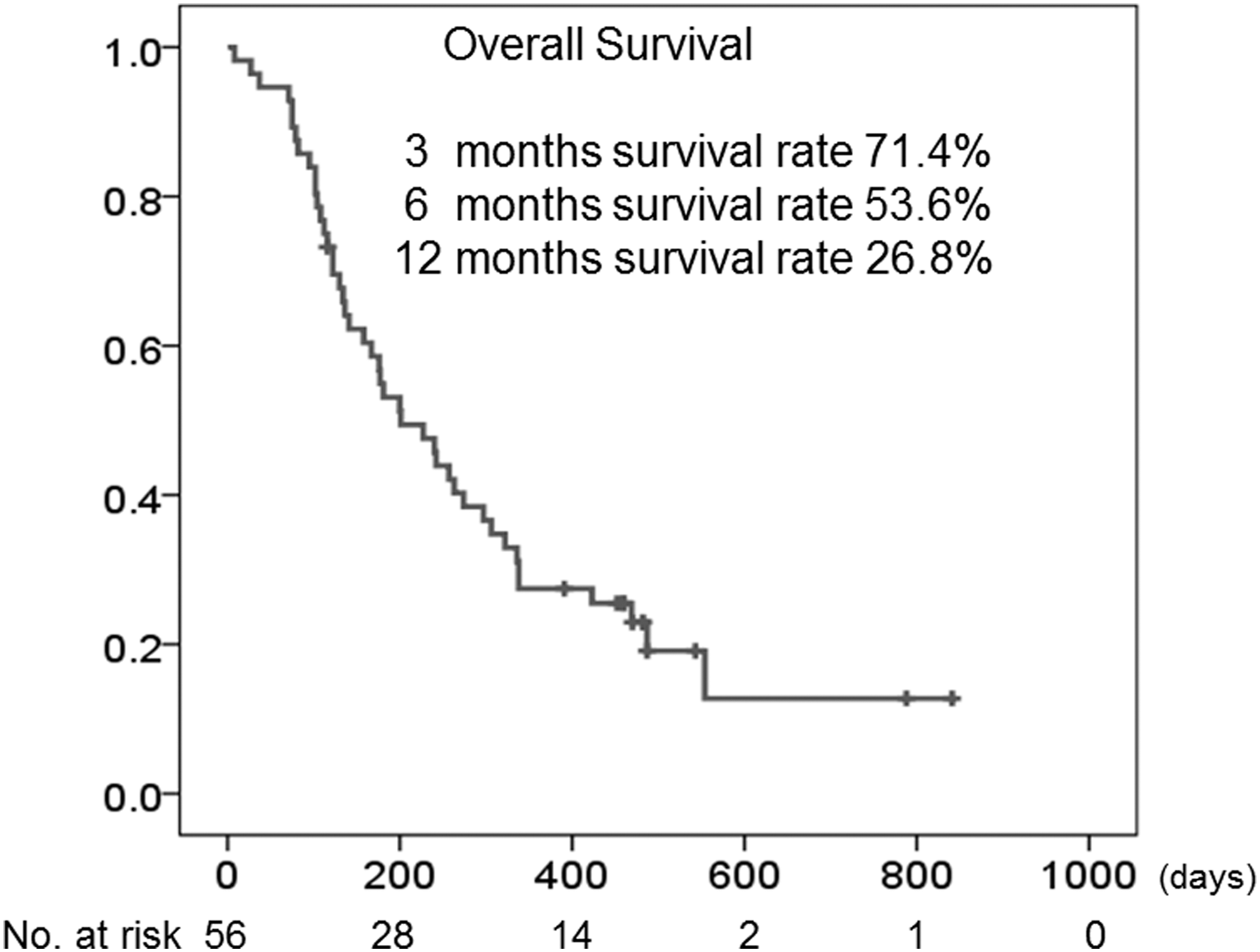
Overall survival plot of all 56 patients confirmed to have ATC pathologically determined by the Kaplan-Meier method. Fifty patients were treated with chemotherapy alone, and six patients were treated with chemotherapy and concomitant radiation therapy.
The median OS for the patients with stage IVA, IVB, and IVC disease were 14.1 [CI 6.6–21.6], 8.0 [CI 0.2–15.8], and 5.3 [CI 3.4–7.1] months, respectively. The 6-month survival rates were 80.8%, 57.9%, and 40.9% for stage IVA, IVB, and IVC patients, respectively. The patients classified as having stage IVC disease showed significantly poorer survival compared to those with stage IVA or IVB disease (log-rank test p = 0.042 or 0.049; Fig. 4).
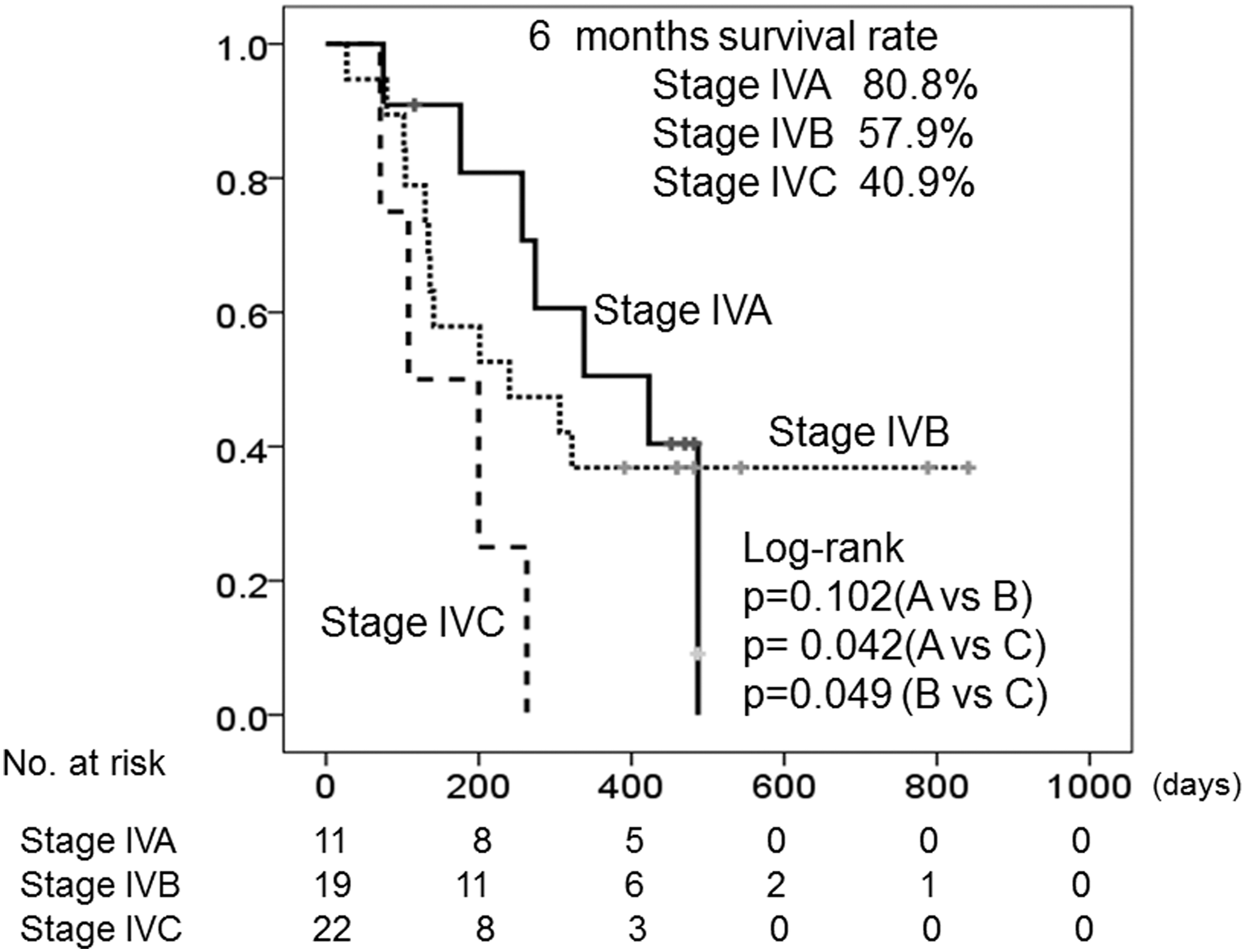
Overall survival plot and 6-month survival rates determined by the Kaplan-Meier method, stratified by the clinical stage (IVA to IVC) of the disease. Four out of all 56 patients with anaplastic thyroid cancer in the locally recurrent disease of previously treated thyroid cancer group were excluded from stage classification.
Although a measurable target lesion was identified in 42 patients, 3 patients could not complete a single course of the protocol treatment. Of the 42 evaluable tumors, 21 (50.0%) showed a variable extent of tumor shrinkage (Fig. 5). No patient demonstrated a CR or durable SD (i.e., SD persisting for >3 months). Nine, twenty-two, and eight of these 42 patients (21%, 52%, and 19%) demonstrated PR, SD, and PD, respectively. An objective response (CR + PR) was thus confirmed in 9 (21.4%) patients, and a clinical benefit (CR + PR + SD) was observed in 31 (73.8%) patients. The time to progression was 0.4–26.3 months (median 1.6 months). Three patients received concomitant EBRT.
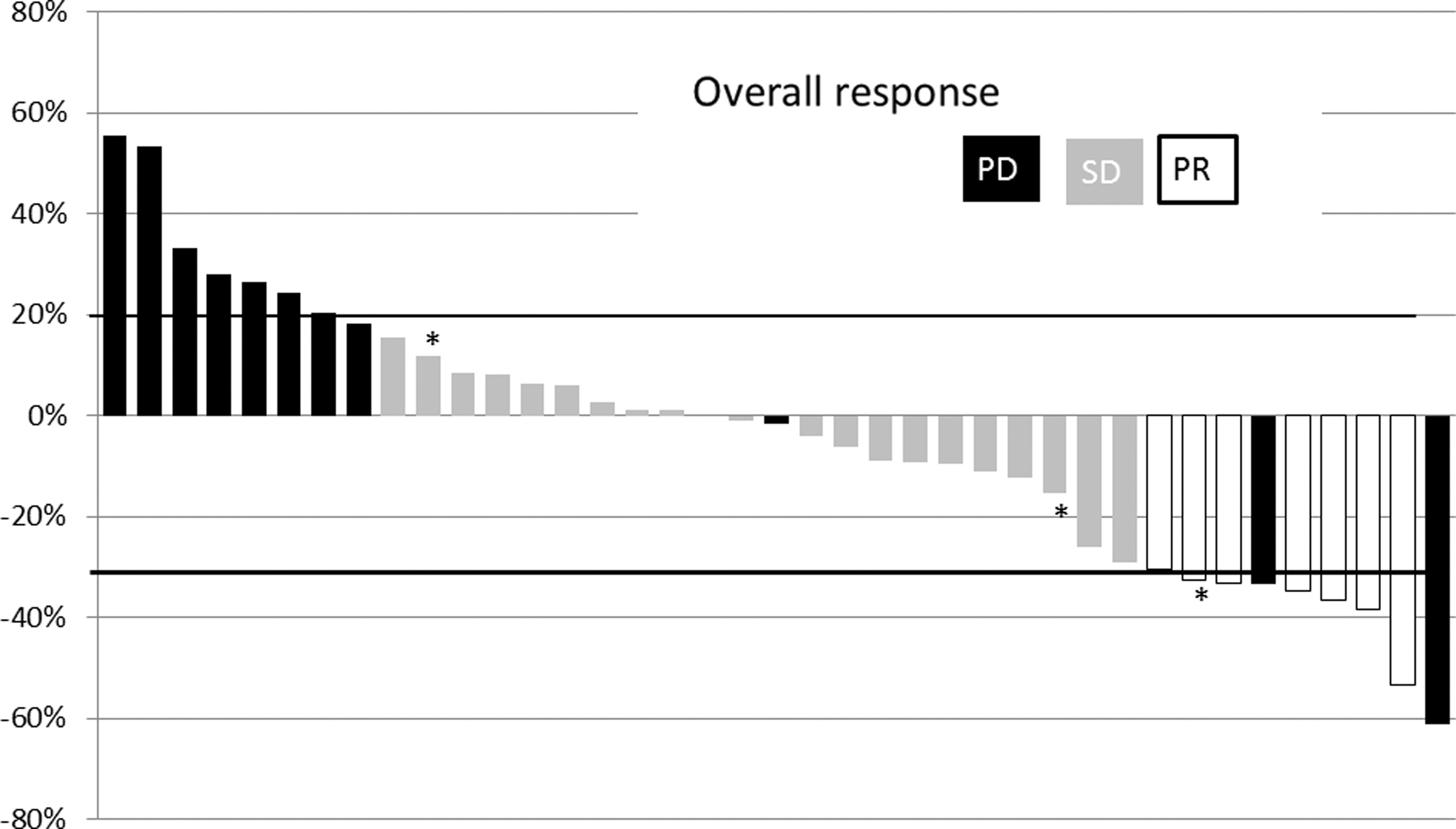
Waterfall plot showing the effect of the treatment on Response Evaluation Criteria in Solid Tumors–defined target lesion. The result of 39 patients who accomplished at least one course of protocol treatment was demonstrated within the cohort of 42 patients with evaluable lesion. Patients who received concomitant radiation therapy were included (*).
Overall, EBRT was conducted in six patients with a dose of 40 (three patients) or 60 (three patients) Gy. A patient with stage IVA disease and two patients with stage IVB disease received EBRT as an adjuvant therapy after curative surgery and survived 10.7 to 28.1 months. Two other patients with stage IVC disease received EBRT for the primary neck tumor as a part of systemic therapy; they showed PR or SD and survived 3.3 and 11.3 months, respectively. Another patient received EBRT for a lung metastasis after locally curative operation for stage IVA disease and survived 9.1 months with confirmed SD. The median OS of these patients were longer (10.7 months [CI 8.2–13.3]) than those who did not receive EBRT (5.9 months [CI 4.2–7.6]) but no statistical difference was identified (log-rank test p = 0.204). The study protocol was initially conducted as neo-adjuvant chemotherapy in 14 patients. Of these, 2, 8, and 4 patients were classified to have stage IVA, IVB, and IVC disease, respectively. Complete removal of the local tumor could be achieved in 8 patients (5 patients with stage IVB and 3 with stage IVC disease) after chemotherapy. They survived from 3.3 to 26.3 months, and that was significantly longer (median 7.6 months [CI 8.1–23.0]) than the other 34 patients (5.4 months [CI 3.0–7.8], p = 0.018) (Fig. 6). Of these 34 patients, 4, were classified as having stage IVA, 9 as IVB, 17 as IVC, and 4 as having stage X disease.

Cause-specific survival plot determined by the Kaplan-Meier method. Survival was compared between the patients whose tumor has completely removed after neo-adjuvant chemotherapy (NAC; n = 8), and other patients in whom the tumor could not be completely removed (including no surgery) after chemotherapy (n = 34) in the cohort for efficacy analysis.
Discussion
Several observations suggested that taxanes might be beneficial agents for controlling ATC (3,10 –12). For example, Ain et al. demonstrated the efficacy of paclitaxel in 19 patients with ATC for the first time in 2000; they administered a 96-hour continuous infusion of the agent in a 21-day cycle, and the results demonstrated a response rate of 53%, with one CR patient (10). Kawada et al. used docetaxel in a 21-day cycle for 7 ATC patients, and they reported a response rate of 43% with one CR (11). Higashiyama et al. reported their retrospective experience with a weekly paclitaxel administration in 13 patients: a response rate of 31% with one CR was observed. They concluded that weekly administration of paclitaxel could be beneficial to extend the survival of ATC patients with stage IVB disease (12). Our present findings objectively confirm the feasibility and efficacy of paclitaxel-based chemotherapy in ATC patients. Our study also demonstrates the potential usefulness of weekly paclitaxel treatment as a neo-adjuvant chemotherapy for patients with ATC, as suggested by Higashiyama et al. (12).
Haymart et al. reported a median OS of stage IVA, IVB, and IVC ATC patients as 9.0, 4.8, and 3.0 months, respectively, by analyzing a large cohort of a national cancer database (2). Our results demonstrate much longer OS of 14.1, 8.0, and 5.3 months, respectively. A clinical trial by Sosa et al. investigating the efficacy of fosbretabulin in addition to a combination protocol with paclitaxel and carboplatin enrolled mainly patients with stage IVC metastatic ATC (16). The results presented here concerning the survival of stage IVC patients (median OS 5.3 months; 6-month survival 40.9%) seems better compared to the control arm of the study by Sosa et al. (OS 4.0 months, 34.9%), and they are in line with the results of the fosbretabulin arm (OS 5.2 months, 48.1%). Other studies reported that the median survival of ATC patients with stage IVC disease was 2.5 (6) or 2.7 months (8). However, it is difficult to compare these outcomes due to differences in eligibility and treatment approaches in each study.
We could not exclude the administration of EBRT in this study, because radiation was the only recommended treatment stated in the Japanese guideline for ATC at the time when the study started (9). The OS of the six patients receiving EBRT was longer, though it was not significantly different and it may, at least in part, be caused by patient selection bias. Radiation therapies were performed as an adjuvant therapy after surgical removal of the tumor in three patients. Several previous studies have demonstrated a benefit of EBRT to control local ATC disease (17 –19). Further structured studies are required to clarify the role and significance of EBRT.
All the AEs observed in the present study were tolerable and manageable. The results of our study confirm that the protocol used could be performed without changes and with a sufficient dose intensity during early courses. This protocol might also be conducted in an outpatient setting. We were also able to terminate the protocol, when necessary, without any prolonged AEs that would delay the start of treatment following chemotherapy or AEs that would impair patients' quality of life.
The progress of the patient enrollment was much smoother than had been expected (13). There was no patient who did not meet the criteria at the initial eligibility evaluation and no protocol violation during the course to exclude a patient from the study. In addition, 92% of the pathological diagnoses at local referral institutions were confirmed to be correct. These substantial baseline qualities of the registered institutions were clearly due to the concordant desire and coordination of the ATCCJ study group members. The lack of a standardized therapeutic strategy and the simple protocol used in this study contributed positively to enroll patients for active participation in this study.
The treatment protocol presented here can be used for ATC patients, and it showed marginal clinical benefit. In conclusion, this study clearly demonstrates the feasibility and objective outcomes of a standardized chemotherapy by weekly paclitaxel for ATC patients.
Footnotes
Acknowledgments
We thank all of the patients who participated in this study. The study was approved and supported by all of the members of ATCCJ. The authors sincerely thank Professor Yoshihide Fujimoto and Professor Michio Sowa for reviewing and monitoring the study as members of the safety review board, and Dr. Mitsuyoshi Hirokawa, Professor Kennichi Kakudo, and Professor Atsuhiko Sakamoto for reviewing the tumor samples as members of Central Pathology Review Board. This study was initiated with thoughtful support from Professor Kosei Hirakawa of Osaka City University. We also thank Ms. Yuka Matsumoto and the members of the Center for Drug and Food Clinical Evaluation of Osaka City University Hospital for the data accumulation and management.
This work was supported in part by a grant-in-aid for scientific research from the Japan Society for the Promotion of Science (JSPS KAKENHI #25461992) to N.O., a grant-in-aid for strategic research from Osaka City University (Novel Priority Research B) to N.O., and a study grant from the nonprofit organization TODoc Network.
Author Disclosure Statement
N.O. received honoraria and research funding from Eisai and Bayer and is a member of the advisory boards of Eisai and Bayer. I.S. received honoraria from Eisai and Bayer; research funding from Eisai; travel expenses from Bayer, Eisai, Genzyme; and is a member of advisory board of AstraZeneca and Bayer. All remaining authors have declared no conflicts of interest.