
Abstract
Background:
Thyroid lymphoma is a relatively rare disease often posing a diagnostic challenge. Reaching the final diagnosis can be delayed if insufficient biopsy material is obtained for immunohistochemistry analysis. The aim of this study was to evaluate the clinical, biochemical, and radiological features of thyroid lymphoma.
Methods:
A retrospective analysis was conducted of all Mayo Clinic patients evaluated between 2000 and 2014 who had a tissue biopsy positive for thyroid lymphoma.
Results:
Seventy-five subjects had biopsy-proven thyroid lymphoma, and 62.7% were primary thyroid lymphomas. The median age at diagnosis was 67 years (range 20–90 years). A total of 50.7% were male, and 54.7% had a history of Hashimoto's thyroiditis. Presenting symptoms included neck mass (88%), dysphagia (45.3%), and hoarseness (37.3%). The typical ultrasound appearance consisted of a solid, hypoechoic mass with increased vascularity and variable edge characteristics. Fine-needle aspiration (FNA) biopsies were abnormal in 70.7% of cases, and 42% indicated a specific lymphoma subtype. The diagnosis was confirmed in 53.3% by core biopsy, in 21.3% by thyroidectomy (partial or total), in 12% through incisional biopsy, and in 12% by lymph node biopsy. Core biopsy had a higher sensitivity compared with FNA (93% vs. 71%, p = 0.006).
Conclusion:
A rapidly enlarging neck mass in the setting of Hashimoto's thyroiditis should raise suspicion for thyroid lymphoma. Radiologically, this usually presents as a large, unilateral, thyroid-centered mass, hypoechoic by ultrasound, and expanding into adjacent soft tissues. Core-needle biopsy should be the first diagnostic test to expedite reaching the final diagnosis and decrease patient burden of additional tests and interventions.
Introduction
T
Unlike other types of thyroid cancer, thyroid lymphoma arises from lymphocytes, most commonly B lymphocytes (7). While fine-needle aspiration (FNA) cytology may be sufficient for the diagnosis of most thyroid masses, its accuracy in thyroid lymphoma is quite variable (2,8,9). This is due to the sample size needed to perform immunohistochemistry, which is necessary for a precise diagnosis with subtype confirmation. Thus, more tissue is required for diagnosis than it is for typical thyroid malignancies. The treatment chosen and overall prognosis are dependent on the subtype of lymphoma, making it imperative to determine the diagnosis expeditiously and accurately. With recent advances in treatment, primary thyroid lymphomas are very responsive to therapeutic interventions, with excellent overall survival rates compared with more aggressive types of thyroid malignancies such as anaplastic thyroid cancer (10,11).
As thyroid lymphoma is an overall uncommon disease, there are only a few large studies in the literature specifically looking at the clinical pattern and presentation (2,12). The aim of this study was to identify unique clinical, biochemical, and radiological presenting features of thyroid lymphomas treated at a single institution. This can aid the clinician to determine more accurately the pretest probability of thyroid lymphoma and aid in selecting the diagnostic tests with the highest yield to reach a final diagnosis for this entity.
Methods
An electronic search of all patients with a tissue diagnosis of thyroid lymphoma from January 1, 2000, to December 31, 2014, was conducted using the Mayo Clinic Lymphoma Database. Demographic, clinical, and laboratory data were extracted from the electronic medical record. Each case had a tissue diagnosis reviewed by lymphoma hematopathologists. Radiological data were independently reviewed by a radiologist expert in neck imaging. Laboratory data collected included sensitive thyrotropin (TSH), free thyroxine, and serum thyroid peroxidase antibody (TPO), with reference ranges of 0.3–4.2 mIU/L, 0.9–1.7 ng/dL, and <9.0 IU/mL, respectively.
Reported age and laboratory data correspond to the time of first diagnosis. Presence of hypothyroidism was defined as either having an elevated TSH value or being on levothyroxine replacement therapy at the time of diagnosis. A diagnosis of Hashimoto's thyroiditis was defined as either having positive TPO or carrying the diagnosis in the medical history if the patient was not diagnosed at the Mayo Clinic. On ultrasound imaging, hypoechoic was defined as having decreased echogenicity relative to adjacent thyroid tissue, and very hypoechoic as decreased echogenicity relative to adjacent musculature. FNA biopsy was defined as a biopsy performed with a needle gauge of 25–27G. Core-needle biopsy was defined as a biopsy performed with a spring-loaded tru-cut configured biopsy needle with a gauge of 18G or 20G. Primary thyroid lymphoma was disease confined to the neck, and secondary lymphoma consisted of a positive thyroid tissue biopsy of lymphoma combined with radiologic confirmation of disease outside of the neck.
Statistical analysis
Continuous variables are expressed as means with standard deviations (SD) for normal distributions, and median with interquartile range (IQR) for non-Gaussian distributions. Categorical variables are reported as percentages and were analyzed with Pearson's chi square. Continuous variables were subjected to two-sample t-tests or non-parametric testing (Mann–Whitney U-test) if not normally distributed. A p-value of <0.05 was considered significant.
Results
Clinical presentation
Seventy-five patients were identified as having thyroid lymphoma during the specified time period. The median age at presentation was 67 years (range 20–90 years), with an almost 1:1 ratio of males to females (38 males, 37 females). The median age and male-to-female ratio were the same when comparing primary and secondary lymphoma. The most common presenting symptoms were a rapidly enlarging neck mass (88%) with symptoms of compression (dysphagia 45.3%, hoarseness 37.3%, and difficulty breathing 24%). The median duration of symptoms before presentation was four weeks (IQR 3–12 weeks). The presenting features of primary versus secondary thyroid lymphoma were similar, with no statistical difference. A complete summary of symptoms and the reported frequency is presented in Table 1. A total of 65.3% of patients had primary hypothyroidism before the diagnosis of thyroid lymphoma, with a known etiology in 54.7% (Hashimoto's thyroiditis) and a median duration of eight years (IQR 1–15 years). Of all patients, 34.7% had an elevated TSH at the time of diagnosis of thyroid lymphoma, and of those, half had subclinical hypothyroidism. Three patients had iatrogenic subclinical hyperthyroidism. The mean TSH at presentation was 9.52 ± 20.99 mIU/L. TPO was tested in 29 patients, and of these, 48.2% had positive TPO antibodies. There was a tendency for TPO positivity to occur more often in primary thyroid lymphoma than in secondary thyroid lymphoma (66.7% vs. 33.3%; p = 0.78). Eight patients (10.7%) had B-type symptoms (fever, weight loss, night sweats), with a median age of 70 years, and with the majority diagnosed with primary thyroid lymphoma (62.5%). The most common descriptors used in documenting the thyroid physical exam were a palpable unilateral mass (52.9%) and diffuse thyroid enlargement (47.1%). Documented palpable lymph nodes were found in 10.1% of patients.
Radiologic data
Fifty-eight patients had ultrasound images available for review. Electronic images with another imaging modality were available for the remainder of the cohort (17), as the initial thyroid ultrasound was performed at another facility, and patients were referred for further evaluation. Thyroid lymphoma was described as a solid and hypoechoic mass, where echogenicity was less than that of the adjacent thyroid parenchyma in all cases, with 67.2% classified as very hypoechoic, where the echogenicity was less than that of the adjacent neck musculature (Fig. 1). The typical appearance consisted of increased vascularity relative to normal thyroid parenchyma, no internal calcifications, and variable edge characteristics (from well-defined to ill-defined; Fig. 2). The median volume was 70.2 cm3 (IQR 29.8–136.7 cm3). Computed tomography was performed in 53.3% of patients, and 76% had positron emission tomography (PET) imaging, with 64.9% of the lesions described as PET avid. In 15 cases, SUV data were reported, with a median SUVmax of 22.7 (range 10.6–37.6). Tracheal deviation was present on imaging in 21.3% of patients. There was no association between ultrasound characteristics and histologic subtype or stage of thyroid lymphoma.
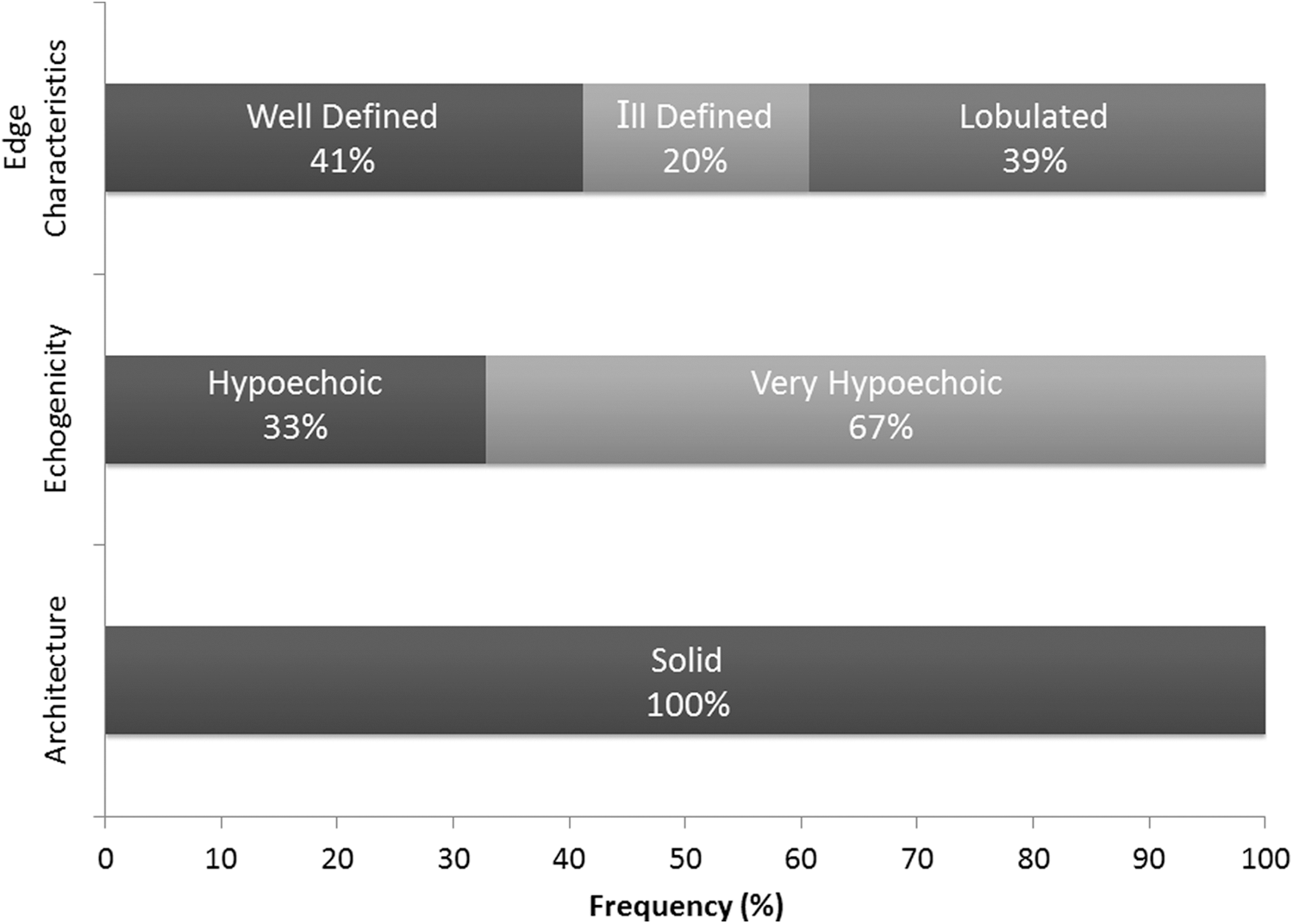
Ultrasound characteristics of thyroid lymphoma.
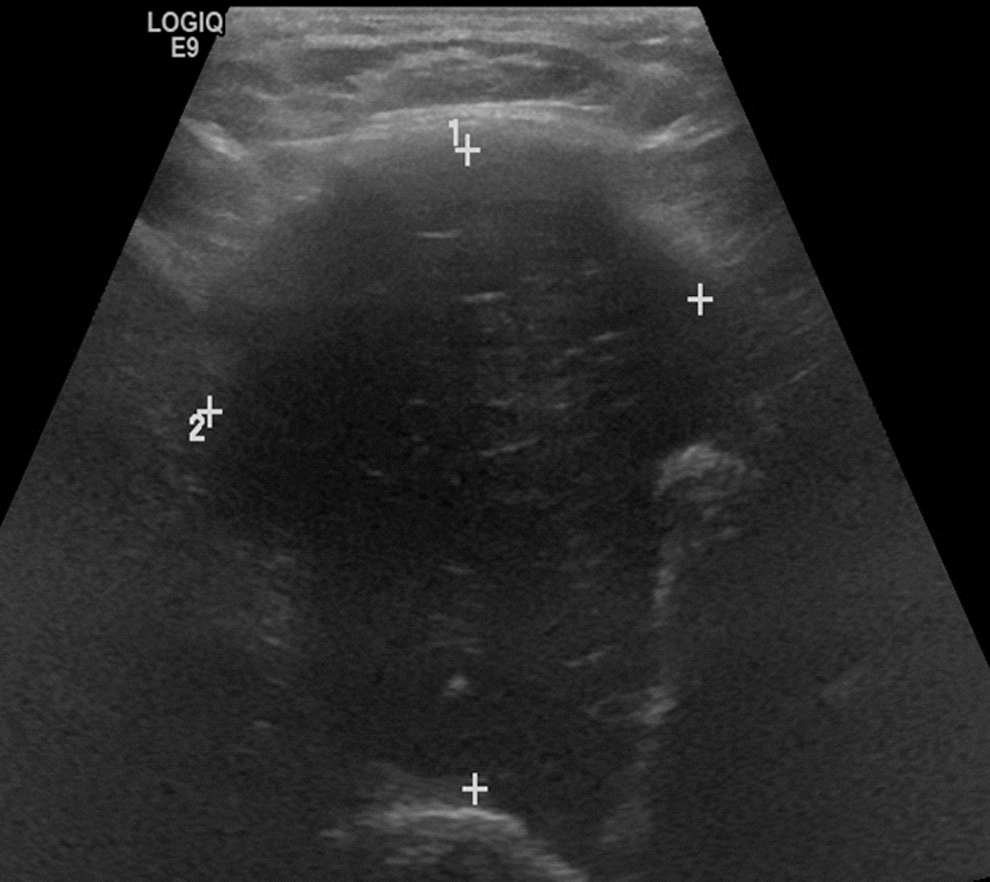
Typical ultrasound appearance of thyroid lymphoma.
Diagnosis
Sixty-five patients underwent a FNA biopsy as their first diagnostic test. In the remainder of the cohort, six (8%) patients underwent surgery (four lobectomies and two total thyroidectomies), three patients had thyroid core biopsies, and one patient had an open incisional thyroid biopsy. Those who underwent surgery as their first diagnostic step presented with concerning symptoms of aero-digestive tract compression. The open incisional thyroid biopsy was performed while the patient was intubated due to airway compromise from the rapidly enlarging thyroid mass. Initial diagnostic FNAs were reported as abnormal in 70.7% of cases (12 “large B-cell lymphoma,” 10 “suspicious for lymphoma,” 2 “high-grade malignancy”), with 41.5% indicating a specific lymphoma subtype. Of all FNAs, 26.2% were interpreted as benign (20% were labeled Hashimoto's thyroiditis) and 3.1% as non-diagnostic (Fig. 3). Of FNA reports that were lymphoma subtype specific, 89% were consistent with the final diagnosis. FNA was more likely to be accurate when the final diagnosis was diffuse large B-cell lymphoma (DLBCL) than when it was other subtypes of lymphoma (p = 0.003). Despite this, all patients who had FNA as their first diagnostic step required further tissue for subtype confirmation (Fig. 4). The diagnosis was confirmed in 53.3% by core biopsy, in 21.3% by thyroidectomy (partial or total), in 12% through incisional biopsy, and in 12% by lymph node biopsy. The overall sensitivity for core biopsy was 93% compared with 71% for FNA. For mucosa-associated lymphoid tissue (MALT) lymphoma, core biopsy was far superior to FNA (100% vs. 25%; p = 0.01). Histologic subtypes included DLBCL (72%), MALT lymphoma (12%), follicular lymphoma (5.3%), MALT/DLBCL (4%), T-cell lymphoma (2.7%), and Hodgkin's lymphoma (2.7%). A total of 88.9% of cases of MALT lymphoma had a positive history of Hashimoto's thyroiditis (relative risk 6.6 compared to non-MALT lymphoma [confidence interval 0.87–50.44]; p = 0.06).
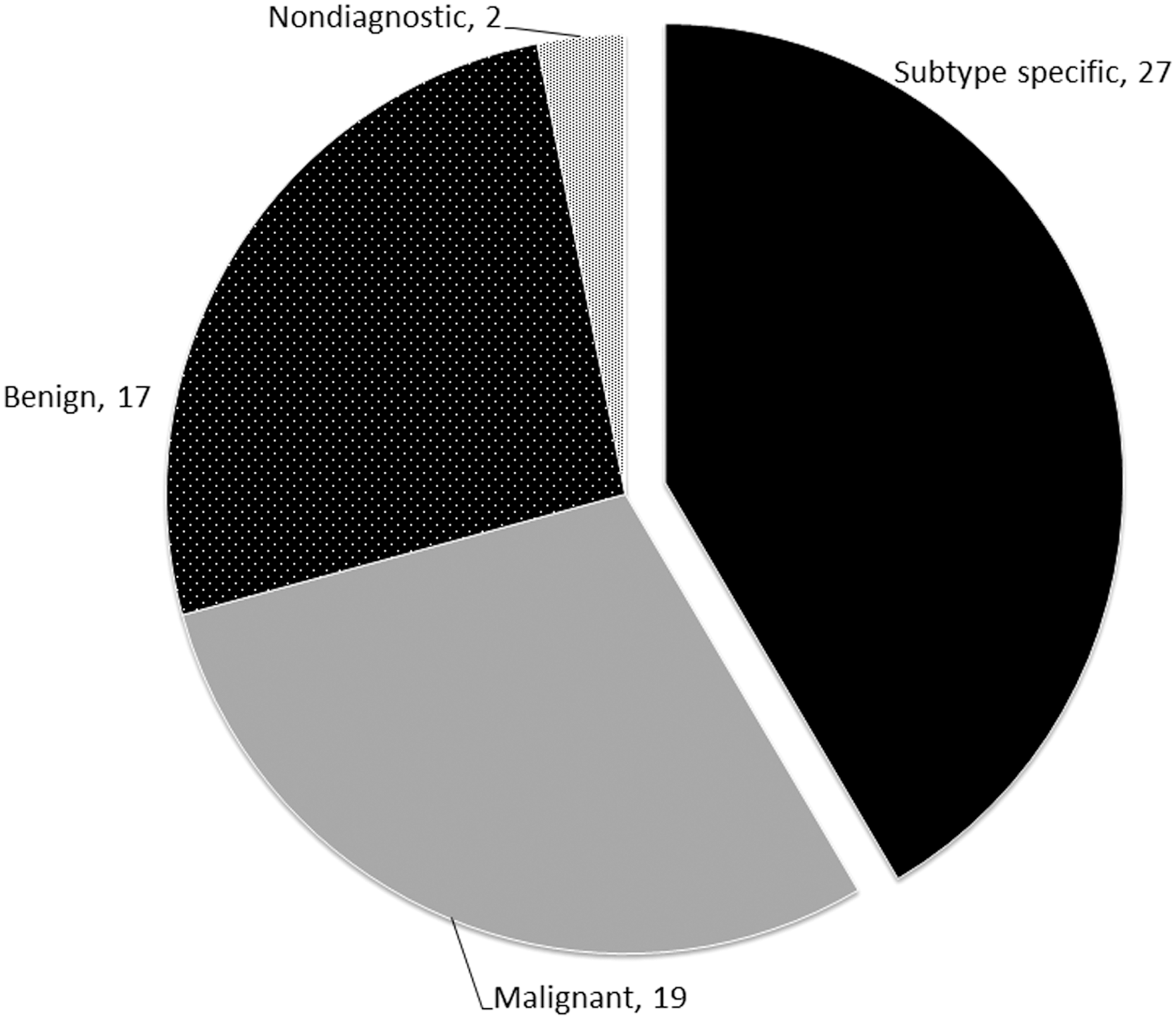
Fine-needle aspiration diagnoses reported.
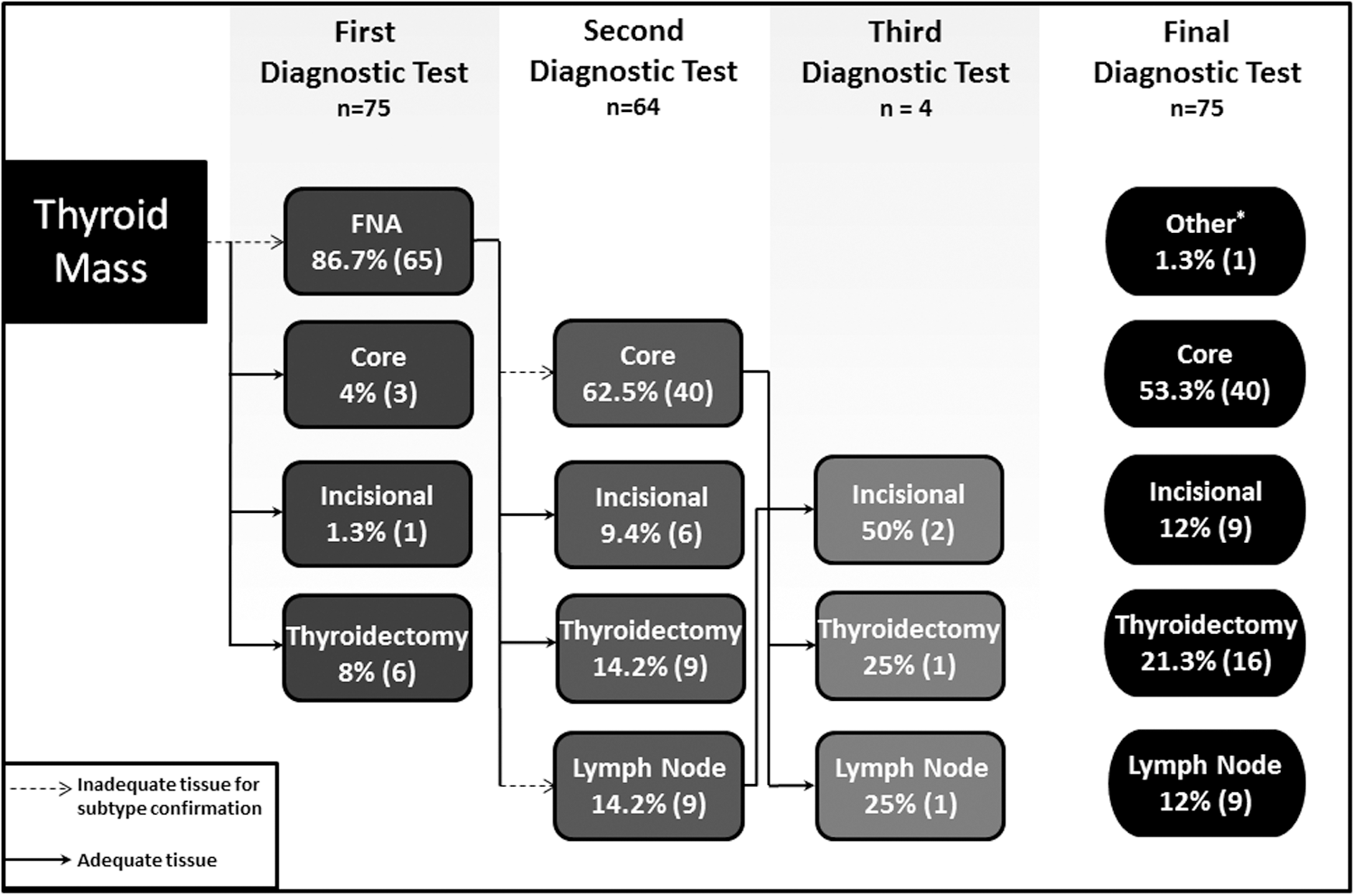
Diagnostic steps taken to reach subtype confirmation of thyroid lymphoma. Core, core thyroid biopsy; Incisional, incisional thyroid biopsy; *Stage IV lymphoma with gastric biopsy subtype confirmation.
Discussion
This series, which is among the largest published (2,12), identifies thyroid lymphoma as a rapidly enlarging mass occurring in patients with a history of Hashimoto's thyroiditis, usually developing in the sixth and seventh decades of life. These key elements are consistent with prior reports (2,10,12), the main difference being that a sex predisposition was not identified, similar to the report by Sirota et al. (13). This can be due to referral bias, as the center is a tertiary/quaternary facility and would have an inherent bias favoring more advanced and complex cases. This series also has a much larger proportion of secondary thyroid lymphomas compared with previous reports. Yet, the sex distribution in both primary and secondary thyroid lymphomas was relatively even, with the primary thyroid lymphoma group having 60% males. The presentation of thyroid lymphomas in the cohort has significant overlap with that typically seen in anaplastic thyroid cancer (14,15), making it difficult for the clinician to distinguish between the two based on history. A history of Hashimoto's thyroiditis is one of the differentiating historical factors between anaplastic thyroid cancer and thyroid lymphoma (16,17). Previous reports have identified the risk of developing thyroid lymphoma to be 67 times higher in patients with Hashimoto's thyroiditis compared with those with colloid goiter (3), and as high as 90% of subjects with primary thyroid lymphoma having a positive history of thyroid autoimmunity (4). The present study found that thyroid autoimmunity is more commonly associated with MALT lymphomas compared with the other subtypes (relative risk 6.6) in keeping with the previously postulated mechanism of a slow malignant transformation from chronic antigenic stimulation of marginal cells (18).
Ultrasonography is usually the first imaging modality performed in the evaluation of a thyroid mass. Previous studies have categorized ultrasound findings into three categories: diffuse, nodular, or mixed (19,20). A decision was made not to report the data in the present study in this manner, as the clinical utility is questioned due to the low positive predictive value found previously (19). In addition, the general endocrinologist will not receive an ultrasound report ascribing the mass to one of these categories, as this has not been incorporated as standard of care in thyroid ultrasound reporting (21,22). The present data suggest that the typical ultrasound signature of thyroid lymphoma is that of a solid mass that is hypoechoic to very hypoechoic. This is consistent with prior studies (6,20,23) and has significant overlap with anaplastic thyroid cancer (24,25). The presence of significant internal vascularity and absence of calcifications may be distinguishing features between thyroid lymphoma and anaplastic thyroid cancer on ultrasonography (26,27). Table 2 summarizes features found in the present cohort of thyroid lymphoma compared with those published for anaplastic thyroid cancer. It is also reported that PET-avid thyroid lymphoma lesions have a median SUVmax of 22.7, which is about the same as that reported for anaplastic thyroid cancer (mean SUVmax = 24.8 ± 15.8) (28), and much higher than that reported for differentiated thyroid cancer (median SUVmax = 10.4–11.8; range 1.9–53) (29) and Hashimoto's thyroiditis (mean SUVmax = 7.69; range 4.3–13.4) (30). A history of Hashimoto's thyroiditis associated with the presence of these ultrasound features (solid, very hypoechoic, increased internal vascularity, and no calcification) can significantly increase the pretest probability of thyroid lymphoma during the diagnostic workup of a rapidly enlarging thyroid mass.
Thyroid lymphoma data obtained from the authors’ data set.
Data obtained from Ha et al. (8).
After imaging, the next diagnostic step undertaken for most thyroid masses is FNA biopsy. The prognosis of lymphoma has improved significantly over the years, in part due to more specific disease subtyping and specific therapeutic interventions. Adequate tissue sampling is essential for subtype confirmation with immunohistochemistry. Prior to availability of immunohistochemistry, open incisional biopsy was recommended in order to obtain a specimen adequate for histological analysis (2,13). Sangalli et al. (31) reported improved accuracy of FNA when combined with immunohistochemistry. However, the needle gauge used in their protocol was 22G, which is larger than the authors’ standard for FNA (25G or 27G). Unfortunately, other reports of an improved positive predictive value of FNA for thyroid lymphomas did not report needle gauge, making an accurate comparison impossible (9,32). Despite the high rate of correctly suggesting the lymphoma subtype based on FNA cytology, all of the present cases required further tissue for subtype confirmation. A recent review of 99 cases of both thyroid lymphomas and anaplastic thyroid cancer reported that FNA had a decreased sensitivity compared with core-needle biopsy for thyroid lymphoma (8). Thyroid lymphoma was misdiagnosed in one case of core needle biopsy compared with 16 cases of FNA (5% vs. 55%) (8). Alternate diagnoses listed in the FNA group included benign, non-diagnostic, and atypia of undetermined significance. This is similar to the present cohort where three core-needle biopsies were falsely negative compared with19 FNAs (7% vs. 29.2%; p = 0.048). Seventeen of these inaccurate FNAs were given the reassuring label of “benign.” Fortunately, the clinical picture led to further testing, where the most common next step consisted of a core biopsy (62.5%). Core biopsy had a higher overall sensitivity compared with FNA (93% vs. 71%; p = 0.006). For MALT lymphoma, which is a very difficult cytopathologic diagnosis, core biopsy was far superior to FNA (sensitivity 100% vs. 25%; p = 0.01). Differentiating MALT lymphoma from Hashimoto's thyroiditis is difficult, given the similar morphology of the lymphocytes. The use of flow cytometry has significantly increased the sensitivity of FNA (31,32). However, difficulties still exist in terms of diagnostic accuracy for MALT. The quantity of tissue provided and preparation of the sample (e.g., exposure to alcohol or formalin) affect flow cytometry results. Core biopsy provides more tissue for flow cytometry and immunohistochemistry, and it maintains tissue architecture, which is often necessary for the classification and grading of lymphoproliferative disorders. Core biopsy has been previously shown to improve the diagnostic accuracy for lymphomas to 93% from 82% with FNA alone (33). As reported by Matsuzuka et al. (2), when the diagnosis was delayed due to repeated false negative testing by FNA, two patients died of progressive lymphomas, highlighting the importance of choosing a more accurate test first. In the present cohort, core biopsy was frequently delayed by one week after the initial FNA failed to establish a diagnosis (median 7 days; IQR 4–15 days). In addition, major complications with core and FNA biopsies are usually not encountered, with only a small increase in local discomfort with larger needle gauges (34). Thus, performing a core-needle biopsy as the first diagnostic step is recommended when thyroid lymphoma is suspected. This would likely decrease the burden of repeat biopsy testing and potentially obviate the need for invasive diagnostic procedures such as an open incisional biopsy or lobectomy to obtain more tissue.
In six cases, despite the use of core biopsy (three were true positives), a more invasive procedure was needed to ascertain the final diagnosis (four thyroidectomies, one incisional open thyroid biopsy, and one lymph node biopsy). This sequence is depicted in Figure 4. This possibility has to be considered and discussed with the patient at the time of the initial evaluation.
One of the main limitations of this study is that it is a retrospective review, which has its inherent biases. The incidence and prevalence of thyroid lymphoma were not determined. No control group was included. Test characteristics of the various diagnostic techniques therefore were unable to be calculated. Clinicians should be aware that positive and negative predictive values will vary according to the prevalence of the disease in the population. Therefore, results should be extrapolated with caution. Needle gauge size used for FNA and core biopsies vary by institution. Therefore, the ordering provider should be aware of this when interpreting results.
In conclusion, thyroid lymphoma should be high on the differential list for clinicians who encounter patients with an enlarging neck mass in the setting of Hashimoto's thyroiditis—the most consistent presentation in the present series. The ultrasound characteristics that should further increase the clinician's index of suspicion consist of a very hypoechoic, solid mass with increased vascularity and absence of internal calcification. Core-needle biopsy should be the first diagnostic step in this clinical scenario, as it will likely provide the final diagnosis with sufficient tissue for accurate subtype confirmation through one diagnostic test. This will not only decrease the procedure burden on the patient, but also prevent delays in diagnosis, thereby allowing earlier initiation of therapeutic interventions. If FNA was initially performed and failed to reach a final diagnosis or subtype, core-needle biopsy should be rapidly performed as the next step.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.