
Abstract
Background:
Only about half of papillary thyroid carcinoma (PTC) cases are classified as conventional PTC (CV-PTC), whereas various histologic variants constitute the remaining cases. Since controversies about the clinical behavior and outcomes of PTC variants continue, the purpose of this study was to compare the outcomes of patients with PTC variants who were treated at a large tertiary referral center in Korea.
Methods:
The medical records for 15,598 CV-PTCs, 435 follicular variants of PTC (FV-PTCs), and 66 diffuse sclerosing variants of PTC (DSV-PTCs) were retrospectively reviewed. Loco-regional recurrences (LRR) among PTC variants were compared using propensity score matching.
Results:
Analysis I compared CV-PTC with FV-PTC. After rigorous matching, 367 pairs were established. Recurrence-free survival (RFS) rates in CV-PTC were 96.1% at 5 years, 92.2% at 10 years, and 92.2% at 15 years, while those for FV-PTC were 98.8% at 5 years, 98.8% at 10 years, and 98.8% at 15 years (p = 0.026). Analysis II compared CV-PTC with DSV-PTC. Rigorous matching yielded 56 pairs. RFS rates for CV-PTC were 87.4% at 5 years, 87.4% at 10 years, and 87.4% at 15 years, while those for DSV-PTC were 68.9% at 5 years, 57.5% at 10 years, and were not available at 15 years (p = 0.013).
Conclusions:
Compared with CV-PTC, FV-PTC showed less aggressive behaviors and more favorable outcomes. However, DSV-PTC showed more aggressive behaviors and a less favorable outcome than CV-PTC did. Therefore, the management strategy and follow-up plan for PTC should be differentiated according to the histologic variant.
Introduction
P
Among all PTC variants, follicular variant of PTC (FV-PTC) is the most common PTC subtype, and occurs in up to 41% of PTC cases (4). A study by Crile et al. in 1953 (5) initially described FV-PTC as having a predominantly follicular architecture that is lined by cells having nuclear features typical of PTC (3,6). Although FV-PTC was first reported >60 years ago, the clinical behavior and outcomes of FV-PTC remain controversial. In previous studies, a greater tendency for pulmonary metastasis (7 –9) and a higher rate of persistent disease (10) were observed for FV-PTC compared with CV-PTC. However, other studies reported that FV-PTC showed less aggressive behavior with similar (11,12) or better long-term prognosis (13,14) compared with CV-PTC.
Another PTC variant, diffuse sclerosing PTC (DSV-PTC), is rare and accounts for only 2–6% of all PTC cases (15,16). Vickery et al. first described DSV-PTC in 1985 (17), and it was adopted as a histologic variant of PTC in 1988 (18). DSV-PTC is characterized by diffuse involvement of the thyroid gland, with extensive squamous metaplasia, abundant psamomma bodies, stromal fibrosis, and prominent lymphocytic infiltration (3,19). Similar to FV-PTC, there have also been controversial findings concerning DSV-PTC prognosis. Previous studies suggested that DSV-PTC has a higher incidence of regional/distant metastasis and a less favorable prognosis compared with CV-PTC (20 –22). However, other studies indicated that DSV-PTC and CV-PTC prognoses did not significantly differ (23 –26).
Thus, the purpose of this study was to compare the clinicopathologic features and CV-PTC prognosis with two common histologic variants of PTC—FV-PTC and DSV-PTC—in the Korean population. Because the mortality rate for PTC is extremely low (27), loco-regional recurrence (LRR) was adopted as a primary endpoint. Although there have been many multicenter (13) and Surveillance, Epidemiology, and End Results (SEER) database studies (12,20), these used only univariate analysis or did not fully adjust for baseline clinicopathologic characteristics. Therefore, a single-center base study was conducted using propensity score matching for rigorous adjustment of baseline clinicopathologic characteristics (28).
Materials and Methods
Patient selection
Between January 1997 and June 2015, 20,030 patients underwent thyroidectomy with or without neck dissection at the Thyroid Cancer Center of Samsung Medical Center, a tertiary referral center in Korea (Fig. 1). Initially, patients with the following conditions were not included: previous history of thyroidectomy, age <18 years, non-PTC (follicular, medullary, or anaplastic), mixed-type PTC, presence of distant metastasis at the time of diagnosis, or follow-up duration less than six months (residual tumor or lymph node [LN] that was detected within six months after the initial surgery, underwent reoperation within six months after the initial surgery, or lost to follow-up within six months). There were only 70 patients with minor variants of PTC (33 oncocytic, 10 tall cell, 10 cribiform morular, 10 solid, 4 columnar cell, 2 insular, and 1 clear cell), and these patients were also excluded. Finally, two distinct analyses were performed for 16,099 PTC patients, including 15,598 CV-PTC, 435 FV-PTC, and 66 DSV-PTC. Using propensity score matching, LRR was compared between CV-PTC and FV-PTC in Analysis I and between CV-PTC and DSV-PTC in Analysis II.
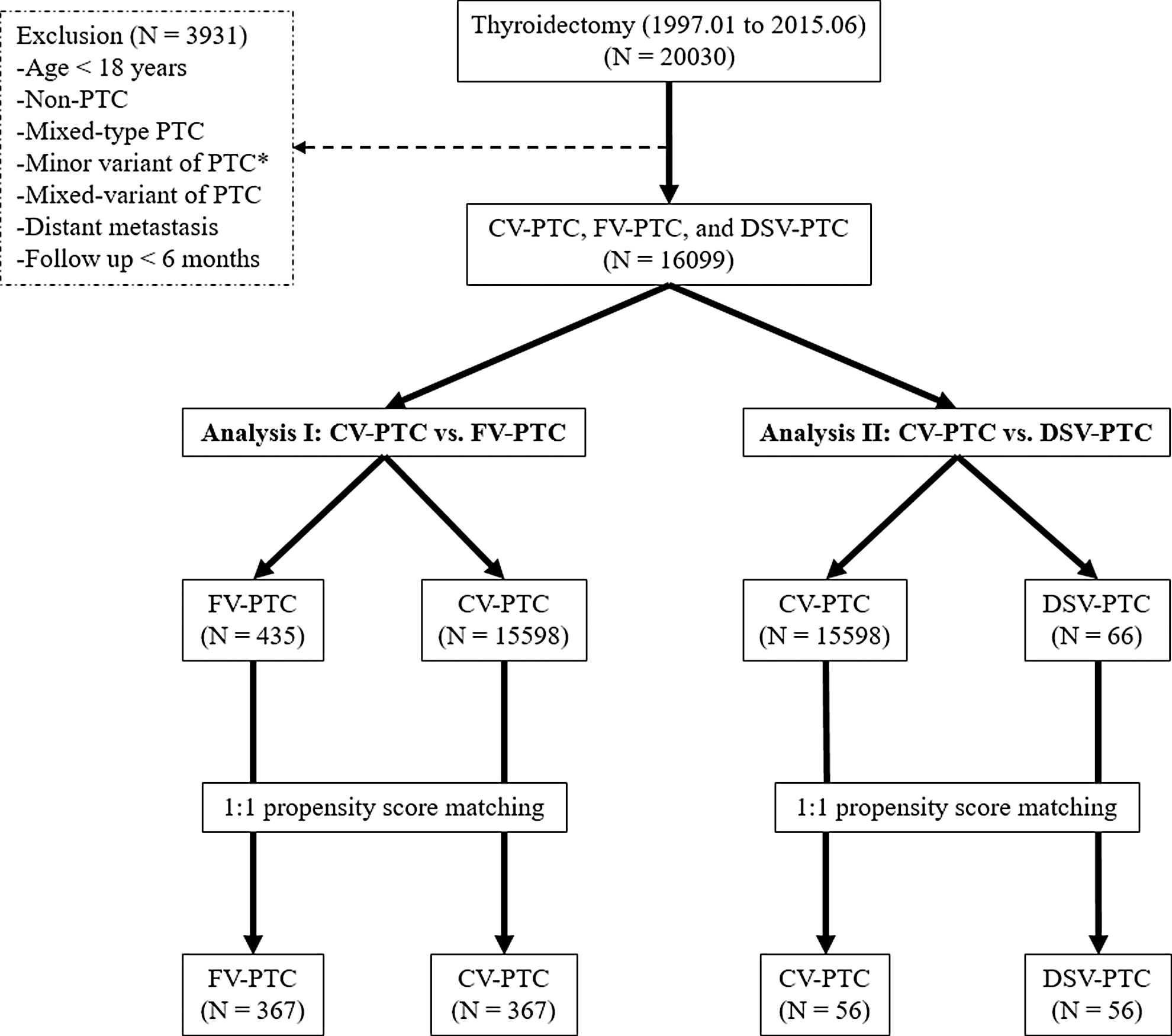
Study flow chart. PTC, papillary thyroid carcinoma; CV-PTC, conventional papillary thyroid carcinoma; FV-PTC, follicular variant of papillary thyroid carcinoma; DSV-PTC, diffuse sclerosing variant of papillary thyroid carcinoma. *33 oncocytic, 10 tall cell, 10 cribiform morular, 10 solid, 4 columnar cell, 2 insular, and 1 clear cell.
Surgical strategy
Following the 2009 American Thyroid Association (ATA) guidelines (29), total thyroidectomy was performed when the primary tumor size was >1 cm, and when multifocality, bilaterality, extrathyroidal extension (ETE), or regional LN metastasis was detected during the preoperative or intraoperative examination. This study included cases with both therapeutic and prophylactic central neck dissection (CND). Therapeutic CND was performed when suspicious lymphadenopathy was detected during the preoperative or intraoperative examination. Prophylactic CND was performed on PTC patients with clinically uninvolved central neck tumors, and in particular for advanced primary tumors (T3/T4) (29), or according to the surgeon's preference at the time of surgery. CND was performed immediately after completion of thyroidectomy, and involved removal of all nodes and fibro-fatty tissue extending vertically from the hyoid bone to the thoracic inlet and laterally from the medial border of the common carotid artery to the trachea midline. The recurrent laryngeal nerve was mobilized and skeletonized along its entire cervical course. In the authors' institution, lateral neck dissection (LND) was only performed in patients with clinically suspicious lateral LN metastasis (LLNM) confirmed by US, computed tomography (CT), and/or FNAB. LND was defined as excision of lateral neck LNs, including modified radical neck dissection (MRND) and selective neck dissection (SND) (30). MRND refers to the excision of lateral neck LNs, including level II–V LN, with preservation of one or more non-lymphatic structures such as the spinal accessory nerve, internal jugular vein, or sternocleidomastoid muscle. Level I dissection was not performed unless indicated. SND refers to the excision of suspicious lateral neck LNs in which there is preservation of one or more of the LN groups that are routinely removed in MRND.
Histopathologic examination of surgical specimens
Surgical specimens were microscopically examined by two or more experienced pathologists who assessed the following histopathologic factors: histologic type of the main lesion, primary tumor size (measured as the longest diameter of the largest lesion), location, multifocality, ETE, lymphovascular invasion, margin involvement, LN metastasis, and underlying thyroid conditions such as chronic lymphocytic thyroiditis (CLT). FV-PTC was considered to be present in cases of PTC showing a follicular growth pattern with virtually no papillary structures together with nuclear features of PTC (3,6). DSV-PTC was considered to be present in PTC cases showing diffuse involvement of the thyroid gland with extensive squamous metaplasia, abundant psamomma bodies, stromal fibrosis, and prominent lymphocytic infiltration along with nuclear features of PTC (3,19).
Postoperative follow-up and management
All patients underwent regular follow-up with clinical evaluations, including physical examinations, US, 131I scans, serum thyroglobulin (Tg), and Tg antibodies at 6- to 12-month intervals. Thyrotropin (TSH) suppression therapy (serum TSH level <0.5 mIU/L) by levothyroxine with or without radioactive iodine (RAI) ablation was considered as an initial postoperative therapy. Although RAI ablation was generally proposed for aggressive features, as recommended by the ATA guidelines (29), the final decision was based on physician or patient preference. The number of RAI administrations and cumulative doses of RAI by the end of follow-up were counted. RAI ablation after recurrence and diagnostic doses of RAI were not included. When RAI treatment was no longer needed for these patients, they received regular follow-up. Loss to follow-up, withdrawal, and deaths were censored as of the last date of follow-up. When LRR was suspected, patients underwent US-guided FNAB with or without measurement of washout Tg levels and/or a thyroid CT or a positron emission tomography/CT. In this study, LRR was defined as the presence of tumor or metastatic LN that was confirmed histologically (FNA or core biopsy) and/or serologically (washing Tg) at least six months after the initial surgery.
Statistical analysis
The statistical analysis was performed using SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY), and statistically significant differences were defined as those with p-values of <0.05. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as the percentage of cases. Chi-square and Fisher's exact tests were used for categorical variables, and the Student's t-test was used for continuous variables. In this study, propensity score matching (28) was performed to adjust stringently for differences in baseline characteristics among PTC variants. The clinicopathologic characteristics that can influence LRR were stringently adjusted using propensity score matching: sex, age (per 10 years), the extent of thyroidectomy (lobectomy or total thyroidectomy), the extent of neck dissection (absent, CND, or LND), tumor size (≤0.5 cm, 0.5–1.0 cm, 1.0–2.0 cm, 2.0–4.0 cm, or >4.0 cm), multifocality, bilaterality, ETE, regional LN metastasis (absent, CLNM, or LLNM), and administered RAI. Under the matched condition, the Kaplan–Meier method and the log-rank test were adopted to compare LRR between PTC variants.
Results
Analysis I: Comparison of CV-PTC with FV-PTC
In total, 15,598 CV-PTC and 435 FV-PTC patients were included in this analysis (Fig. 1). Before propensity score matching, total thyroidectomy (p < 0.001), extensive neck dissection (p < 0.001), multifocality (p < 0.001), ETE (p < 0.001), regional LN metastasis (p < 0.001), and history of RAI were significantly more frequent in CV-PTC than they were in FV-PTC (Table 1). However, male sex (p = 0.010), old age (p = 0.024), and large tumor size (p < 0.001) were significantly more frequent in FV-PTC. Propensity score matching between CV-PTC and FV-PTC patients yielded 367 matched pairs. After pairwise matching, there was no significant difference in the clinicopathologic characteristics between the two variants. Under the propensity score-matched condition, CV-PTC and FV-PTC were compared for prognosis with LRR as the primary endpoint. The mean follow-up time was 53.9 months (range 6.0–215.2 months). LRR was observed in 16 patients (2.2%): 13 (3.5%) with CV-PTC and 3 (0.8%) with FV-PTC. Mean time to recurrence was 34.3 ± 23.4 months, with CV-PTC and FV-PTC having times of 15.5 ± 8.6 months and 37.4 ± 22.7 months, respectively. Recurrence-free survival (RFS) rates in CV-PTC were 96.1% at 5 years, 92.2% at 10 years, and 92.2% at 15 years, while the RFS rates in FV-PTC were 98.8% at 5 years, 98.8% at 10 years, and 98.8% at 15 years (Fig. 2). There was a statistically significant difference in the log-rank test results between the two variants (p = 0.026).
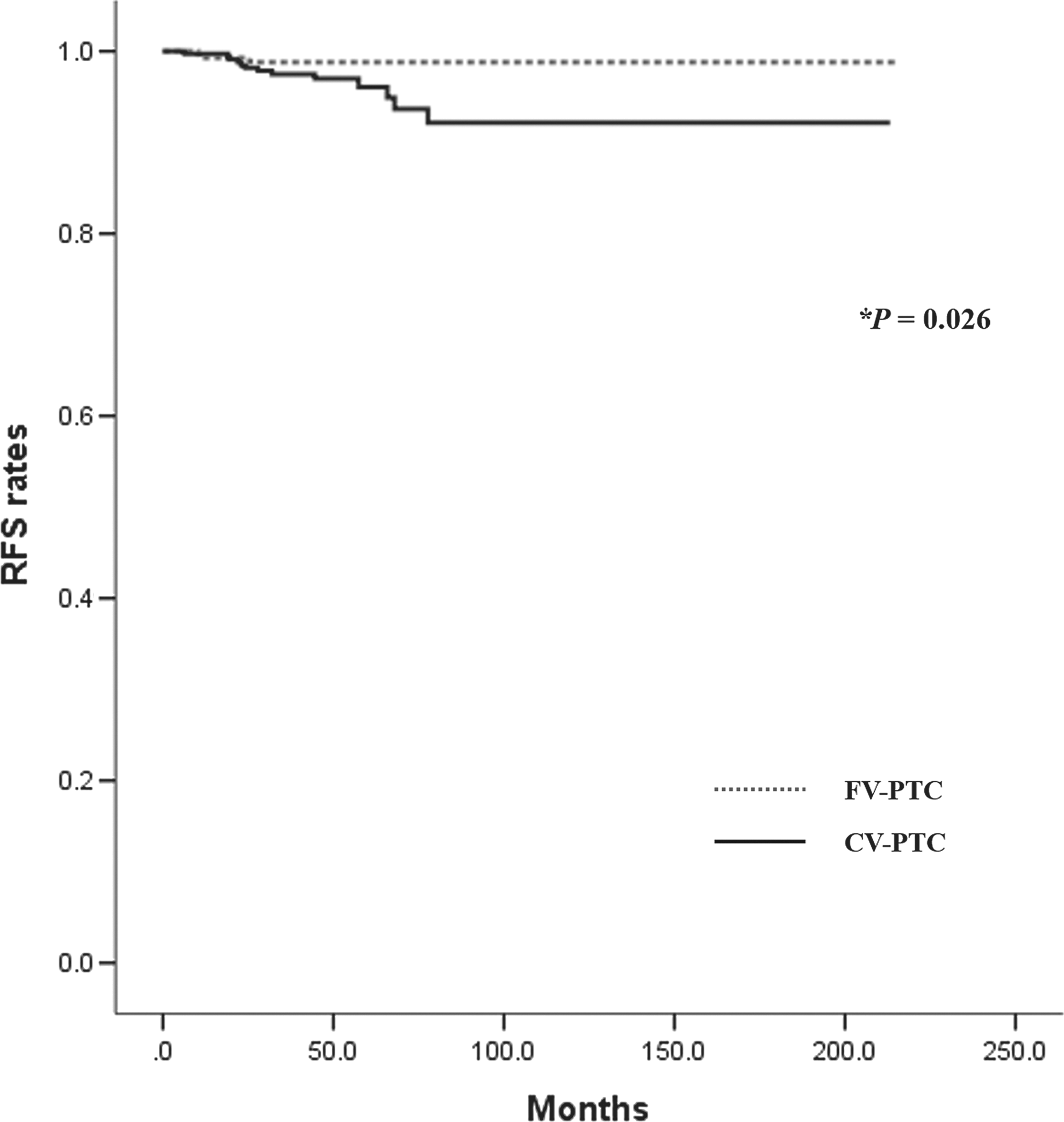
RFS between CV-PTC and FV-PTC under propensity matched conditions. RFS, recurrence-free survival. *Calculated using the log-rank test.
CV-PTC, conventional papillary thyroid carcinoma; FV-PTC, follicular variant of papillary thyroid carcinoma; SD, standard deviation; ETE, extrathyroidal extension; LN, lymph node; RAI, radioactive iodine.
Analysis II: Comparison of CV-PTC with DSV-PTC
In total, 15,598 CV-PTC and 66 DSV-PTC patients were included in this analysis (Fig. 1). Before propensity score matching, only old age (p < 0.001) was significantly more frequent in CV-PTC (Table 2). However, male sex (p < 0.001), thyroidectomy (p < 0.001), extensive neck dissection (p < 0.001), large tumor size (p < 0.001), multifocality (p < 0.001), ETE (p = 0.002), regional LN metastasis (p < 0.001), and history of RAI were significantly more frequent in DSV-PTC compared with CV-PTC. Propensity score matching between CV-PTC and DSV-PTC yielded 56 matched pairs, and between these pairs there was no significant difference in clinicopathologic characteristics between the two variants. Under the propensity score-matched condition, CV-PTC and DSV-PTC were compared for prognosis, with LRR as the primary endpoint. The mean follow-up time was 46.7 months (range 6.0–202.3 months). Among the 18 patients for whom LRR was observed (16.1%), 6 (10.7%) had CV-PTC and 12 (21.4%) had DSV-PTC. The mean time to recurrence was 24.9 ± 19.6 months, with CV-PTC and DSV-PTC showing times of 26.0 ± 12.0 months and 22.8 ± 22.9 months, respectively. RFS rates in CV-PTC were 87.4% at 5 years, 87.4% at 10 years, and 87.4% at 15 years, while the RFS rates in DSV-PTC were 68.9% at 5 years, 57.5% at 10 years, and not available at 15 years (Fig. 3). There was a statistically significant difference in the log-rank test results between the two variants (p = 0.013).
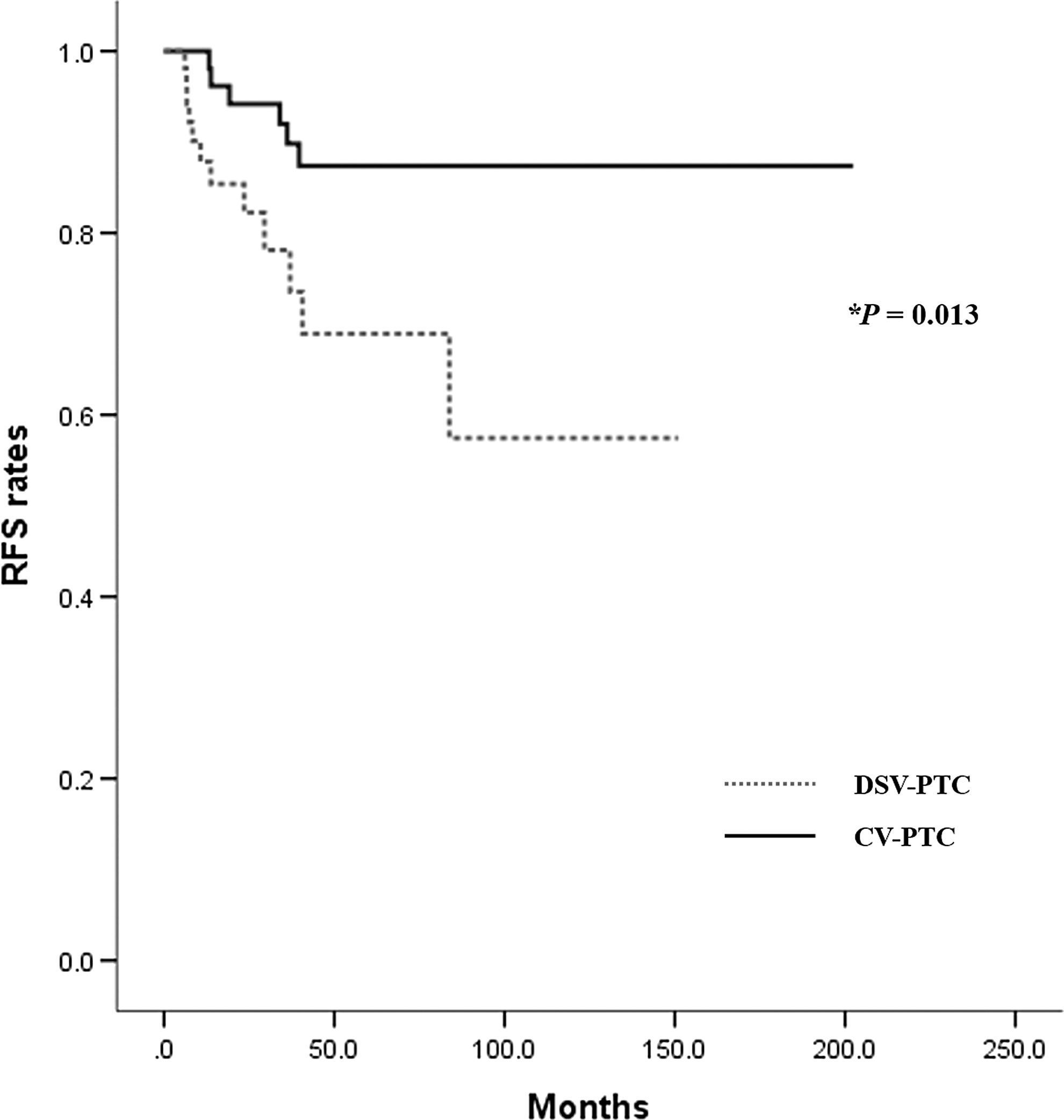
RFS between CV-PTC and FV-PTC under propensity matched conditions. *Calculated using the log-rank test.
DSV-PTC, diffuse sclerosing variant of papillary thyroid carcinoma.
Discussion
Although up to 50% of PTC cases have histologic variants other than CV-PTC (2), there are many controversial theories regarding the behavior and prognosis of these PTC variants (3). The purpose of this study was to compare the LRR of CV-PTC with two common histologic variants in the Korean population: FV-PTC and DSV-PTC. Although many studies have examined this topic (7 –11,14,21 –26), including those that had large multicenter (13) or SEER data (12,20), these studies used only univariate analysis and did not fully adjust for baseline clinicopathologic characteristics. Therefore, this study used propensity score matching for rigorous adjustment of baseline clinicopathologic characteristics (28).
As suggested previously (11 –14), FV-PTC revealed significantly fewer aggressive features such as multifocality, ETE, and LN metastasis compared with CV-PTC (before propensity score matching column in Table 1). Interestingly, a larger tumor size was the only significant factor that was greater in FV-PTC compared with CV-PTC, and similar results were obtained in previous studies (12,13,31 –34). A possible explanation for the size differences between conventional and FV-PTC is selection bias within surgical series resulting from differences in preoperative cytologic findings and indications for surgery. Previous studies (31,33,34) reported that relative to CV-PTC, FV-PTC has more benign US features and non-diagnostic/low-risk cytologic findings on FNAB. Thus, the lower rate of suspicious malignant findings in FV-PTC lesions may result in a more delayed evaluation of FV-PTC lesions by FNAB, which would allow the lesions to grow to a relatively large size. However, as suggested in previous studies (20 –22), DSV-PTC consistently revealed aggressive features, including large tumor size, multifocality, ETE, and LN metastasis, compared with CV-PTC (before propensity score matching column in Table 2).
After stringent propensity score matching between PTC variants, there were no significant differences in their clinicopathologic characteristics. Mortality is extremely low in PTC (27), and under the matched condition, there was no mortality among all cases with PTC variants. Therefore, LRR was compared among the PTC variants using the Kaplan–Meier method and the log-rank test. The RFS for FV-PTC (Fig. 2) was significantly higher than that for CV-PTC (p = 0.026), which is consistent with prior studies (13,14). Meanwhile, the RFS for DSV-PTC (Fig. 3) was significantly lower than that for CV-PTC (p = 0.013), which is also consistent with prior studies (20 –22). Although long-term survival analysis was not performed in this study, these results suggest that FV-PTC is an independent predictor of favorable outcomes and, conversely, DSV-PTC is an independent predictor of less favorable outcomes relative to CV-PTC, even under the matched condition.
This study has several limitations. First, there are inherent limitations of a non-randomized retrospective cohort study. For example, patient information in the data collection may be incomplete. The possibility of residual confounding variables of some measured or unmeasured factors also cannot be ruled out. Second, the prevalence of FV-PTC in this study was 2.7%, while those in previous studies based on Korean populations ranged from 0.9% to 8.8% (35 –40). There is a lower prevalence of FV-PTC in the Korean population compared with Western populations (12,13), and thus this study may have a geographic bias. Third, in the propensity score matching, the baseline clinicopathologic characteristics of one group were adjusted according to those of another group. Therefore, the natural prognosis of each PTC variant is not available under the matched condition. Fourth, there may be inter-observer variation for the detection and interpretation of PTC variants (41). Despite these possible limitations, this study has several strengths. First, medical records were used from a single institution rather than a national or multicenter database, with rigorous exclusion and inclusion criteria to produce a clear and accurate analysis. Second, stringent adjustment by propensity score matching was employed to reduce the differences between PTC variants maximally.
In conclusion, compared with CV-PTC, FV-PTC showed less aggressive behaviors and a more favorable outcome. However, DSV-PTC showed more aggressive behaviors and a less favorable outcome relative to CV-PTC. Therefore, the perioperative management strategy and follow-up plan should be differentiated according to the histologic variant of PTC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.