
Abstract
Background:
This study aimed to evaluate the recurrence and survival after initial curative-intent surgery of resectable anaplastic thyroid cancer (ATC) and poorly differentiated thyroid cancer (PDTC).
Methods:
A retrospective analysis was conducted on patients with ATC and PDTC who had been treated between 1985 and 2013. Among them, 119 patients who had undergone surgery with curative intent were included in this study. The outcome measures included the clinical response to treatment and the recurrence rates of three separate thyroid cancer groups: ATC, differentiated thyroid cancer (DTC) with anaplastic foci, and PDTC.
Results:
Initial remission was achieved in 100 (84.0%) patients, with higher percentages in patients with DTC with anaplastic foci (97.8%) and PDTC (96.7%) compared with ATC (60.5%). The overall recurrence rate after initial remission was 30.8% in ATC, 25.9% in PDTC, and 6.7% in DTC with anaplastic foci. Pathologic diagnosis, preexisting goiter or tumors, along with tracheal and lymphatic/vascular invasion were correlated with recurrence (p < 0.001; p = 0.001, 0.006, 0.003, and 0.016, respectively). All patients without initial remission died due to local failure, and most patients with recurrence, apart from two PDTC patients, had distant metastasis. Overall mortality after initial curative-intent surgery was 58.1% in ATC, 8.7% in DTC with anaplastic foci, and 20% in PDTC.
Conclusions:
The initial remission of resectable tumors was higher and the recurrence rate was lower in DTC with anaplastic foci and PDTC compared with ATC. Careful monitoring of the development of distant metastasis is necessary, especially in patients with aggressive pathology with tracheal and lymphovascular invasion.
Introduction
A
Elimination of ATC or PDTC can be achieved by complete surgical removal, with or without adjuvant radiation or chemotherapy, and resectability is therefore considered one of the most positive prognosis factors (8 –10). Over the years, detection of early thyroid cancer has significantly improved due to the development of diagnostic tools, resulting in the increased detection of tumors consisting of ATC or PDTC, combined with a differentiated thyroid carcinoma (DTC) component (8,10). In addition, surgical techniques, such as tracheal resection and anastomosis or vascular reconstruction, have improved (11 –13). These improvements in detection and treatment have resulted in an increased proportion of resectable ATCs and PDTCs over time, which was <30% before 1995 but >75% after 1995, resulting in a marked improvement in prognosis (10).
Therefore, knowledge of the clinical course and long-term prognosis of these resectable tumors after curative-intent surgery is very important. However, most studies have focused on the survival outcomes of patient cohorts, including resectable and unresectable tumors, and there are limited data regarding the cure rate or recurrence after initial curative-intent surgery of patients whose tumor is considered resectable on imaging studies. A previous study with a large retrospective cohort of ATC and PDTC also demonstrated a better prognosis of resectable tumors compared with unresectable tumors, while subgroup analyses of survival and recurrence outcomes of patients with curative-intent surgery was not included (10). The aim of this study was to analyze the outcomes of patients with resectable tumors with ATC or PDTC histology after curative-intent surgery, along with the clinicopathologic characteristics associated with recurrence in a large retrospective cohort.
Materials and Methods
Subjects
A retrospective chart review was authorized and performed on 188 patients who were diagnosed with ATC or PDTC at Seoul National University Hospital from January 1980 to December 2013 (10). Among them, 128 patients were presented as having a resectable locoregional tumor without distant metastasis. The initial treatment for 125 of these patients was surgery; one had radiation therapy, and two were untreated. Of the 125 patients who underwent surgery, gross total removal (R0 or R1 resection) (14) was achieved in 119 patients, and these 119 were therefore included in our analysis. Medical records, including year of diagnosis, sex, age at diagnosis, blood chemistry, tumor pathology, tumor stage, method of treatment, and survival duration, were reviewed. Pathologic diagnoses were re-evaluated by a pathologist (J.K.W.) and defined as previously described (10,15). Based on the primary diagnosis, pure ATC, ATC arising from DTC (a tumor in which >10% of its volume was occupied by undifferentiated cells), and recurring ATC from DTC (a recurrent tumor with undifferentiated cells in a patient who was diagnosed as DTC at first operation, but with a DTC component detected in recurrence) were combined together as a single group, namely “anaplastic thyroid cancer.” Patients were thus categorized into three groups: ATC, DTC with anaplastic foci (a tumor in which <10% of the tumor volume was occupied by undifferentiated cells in the background of differentiated cancer), and PDTC. PDTC was defined on the basis of the Turin proposal for the use of uniform diagnostic criteria.
The most frequent diagnosis was DTC with anaplastic foci (38.7%), followed by PDTC (25.2%), pure ATC (18.5%), ATC arising from DTC (10.9%), and recurring ATC from DTC (6.7%). Tumor size was defined as the maximal diameter of the surgical specimen (n = 91; 76.5%) or size measured by imaging modalities (n = 28; 23.5%). Nodal and distant metastases at the time of diagnosis were classified using the TNM Classification of Malignant Tumors at the time of diagnosis. Resectability of tumors was determined by interpreting the preoperative computed tomography (CT) scan or magnetic resonance imaging (MRI), as previously described (10). This study was conducted in accordance with the principles of the Declaration of Helsinki, and was approved by the Institutional Review Board of Seoul National University Hospital (No. B-1405-096-580).
Treatment and pattern of recurrence
Among the 119 patients, total thyroidectomy (n = 110, including two cases of total laryngectomy) or near- or sub-total thyroidectomy (n = 9) was performed to achieve R0 resection (n = 98) or at least R1 resection (n = 21). None of the patients underwent surgery with robotic or endoscopic thyroidectomy. Neck dissection was variously performed according to the surgeon's preference and patients’ status. Generally, comprehensive neck dissection was performed in patients with biopsy-proven neck node metastasis, while selective neck dissection was performed in patients with locally invasive primary tumors with an aggressive pathology. Adjuvant radiation therapy was performed in 97 patients (63 patients with external beam radiation therapy [EBRT], 26 with radioactive iodine [RAI], two with both EBRT and RAI, and three with both EBRT and postoperative Adriamycin-based chemotherapy), and two patients were treated postoperatively with Adriamycin-based chemotherapy only. In the first postoperative year, follow-up imaging was performed postoperatively at 3, 6, 9, and 12 months by neck CT scan or ultrasonography with biannual chest X-ray or CT scan. At two years after initial surgery and thereafter, imaging studies were repeated at 6- to 12-month intervals. In the case of new signs and symptoms, or if there were signs suggesting recurrence, additional imaging including PET or bone scans were performed in order to search for metastatic disease, and CT or MRI for suspicious lesions was performed based on clinical manifestations. Complete remission (CR) was defined as no evidence of disease (NED) on physical examination and study of images during follow-up. Initial remission was defined as the status without any evidence of disease at three months after surgery (n = 100). A partial response was defined as at least a 50% reduction of the tumor. Progressive disease was defined as at least a 25% increase in the tumor or the presence of a new lesion. Stable disease was defined as neither sufficient shrinkage to qualify for partial response nor sufficient increase to qualify for progressive disease. A partial response (n = 2), stable disease (n = 2), and progressive disease (n = 15) were regarded as “absent initial remission” (n = 19). Recurrence after initial remission (n = 18) was defined as any of the following: any locoregional or distant recurrence, which was either biopsy-proven (n = 12) or a new radiologic finding identified upon CT (n = 3); MRI (n = 2); or new RAI uptake (n = 1) found in the neck with adequate thyrotropin stimulation. Overall, one- and two-year recurrence rates, recurrence-free survival, and sites of recurrence were analyzed. Data regarding disease-specific mortality were reviewed, based on medical records or the Statistics Korea national database, and one-, two-, and five-year disease-specific survival rates were also calculated.
Statistical analyses
All continuous variables were expressed as means ± standard deviation (SD). Continuous outcomes were analyzed using independent t-tests between groups of two- and one-way analyses of variance between groups of three or more. Dichotomous outcomes were analyzed using the chi-square test for trend and logistic regression analysis. Binary logistic regression analysis was performed to assess the difference in risk factors for dichotomous outcomes (initial remission vs. no initial remission, NED vs. recurrence). Cumulative recurrence rates were calculated by life table analyses to analyze the changes in outcome. All statistical analyses were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). Statistical significance was defined as p < 0.05.
Results
Clinicopathologic characteristics and treatment outcomes of patients who had undergone R0 or R1 resection
Clinicopathologic characteristics and treatment outcomes of the patients are shown in Tables 1 and 2. Age at diagnosis was younger in patients with PDTC (47.7 ± 16.7 years) compared with DTC with anaplastic foci (56.8 ± 13.9 years) and ATC (63.1 ± 12.8 years; p < 0.001). Recurring ATC from DTC showed a relatively higher proportion of females (87.5%) than all the other diagnostic categories did (70.0–72.1%). A total of 24 (20.2%) patients had a history of preexisting goiter or a thyroid tumor, which was less frequent in patients with DTC with anaplastic foci (2.2%) than in other pathologies (p < 0.001). Gross extrathyroidal extension was also more prevalent in ATC (62.8%), while it was very low in DTC with anaplastic foci (4.3%; p = 0.026). Involvement of cervical lymph nodes was also high in ATC (58.1%), but was only 33.3% in PDTC. R0 resection was achieved in 98 (82.4%) patients, which was most frequent in DTC with anaplastic foci (97.8%), followed by PDTC (83.3%) and ATC (65.1%). Initial remission was achieved in 100 (84.0%) patients, and was more frequent in DTC with anaplastic foci (97.8%) and PDTC (96.7%) than it was in ATC (60.5%; p < 0.001). Among the three ATC groups, there were no differences in R0 resection rates (p = 0.673) or in initial remission rates (p = 0.826).
All continuous variables are expressed as means ± SD, except for follow-up duration. Resectable tumors were defined as tumors that are expected to be completely removed with an adequate safety margin. Tumors invading extensively to laryngotracheal, esophageal and/or the prevertebral space, and bilateral carotid artery and/or the jugular vein invasion, which could not be resected even by aggressive surgery (i.e., total laryngectomy, tracheal resection and anastomosis, pharyngoesophagectomy with reconstruction, and vascular reconstruction), were defined as unresectable.
Significantly different between ATC, DTC with anaplastic foci, and PDTC when shouldered on the parameters, and significantly different parameters in post hoc analysis (Tukey and Duncan) if shouldered on each number.
Significantly different between pure ATC, ATC arising from DTC, and recurring ATC from DTC.
Evaluated by CT or MRI.
ATC, anaplastic thyroid carcinoma; DTC, differentiated thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; FU, follow-up; SD, standard deviation; CT, computed tomography; MRI, magnetic resonance imaging.
All continuous variables were expressed as means ± SD, except for follow-up duration. Resectable tumors were defined as tumors that are expected to be completely removed with an adequate safety margin. Tumors invading extensively to laryngotracheal, esophageal and/or the prevertebral space, and bilateral carotid artery and/or the jugular vein invasion, which could not be resected even by aggressive surgery (i.e., total laryngectomy, tracheal resection and anastomosis, pharyngoesophagectomy with reconstruction, and vascular reconstruction), were defined as unresectable.
No initial remission: partial remission, stable disease, or progressive disease.
Significantly different between ATC, DTC with anaplastic foci, and PDTC when shouldered on the parameters, and significantly different parameters in post hoc analysis (Tukey and Duncan) if shouldered on each number.
Expressed as number of patients (relative proportion in overall patients/in patients with initial remission).
Significantly different between pure ATC, ATC arising from DTC, and recurring ATC from DTC.
Significantly different between patients with initial remission and no initial remission.
RR, recurrence rate; NA, not applicable; NED, no evidence of disease.
Among the patients who had achieved initial remission, overall recurrence was detected in 18 (15.1%) patients, and the overall recurrence rate was highest in ATC (30.8%) and lowest in DTC with anaplastic foci (6.7%; p < 0.001). Interestingly, the recurrence rates were different between the three ATC categories (p = 0.012); patients with recurring ATC from DTC showed the highest recurrence rate of 80% among patients with initial remission. Thus, there was only one patient (12.5%) who achieved a final status of NED. On the other hand, no recurrence was observed in patients with ATC arising from DTC, although the initial remission rate was the lowest (53.8%).
Median recurrence-free survival was 31.3 months (range 3.5–176.5 months) and it was also significantly shorter in ATC (6.3 months) than it was in DTC with anaplastic foci (29.0 months) or PDTC (60.2 months; p = 0.025). In ATC, all recurrences were detected within one year (16.3%), except for one case with recurring ATC from DTC. Conversely, there was no recurrence in DTC with anaplastic foci, and only one of the seven PDTC patients displayed recurrence within one year (Table 2 and Fig. 1A).
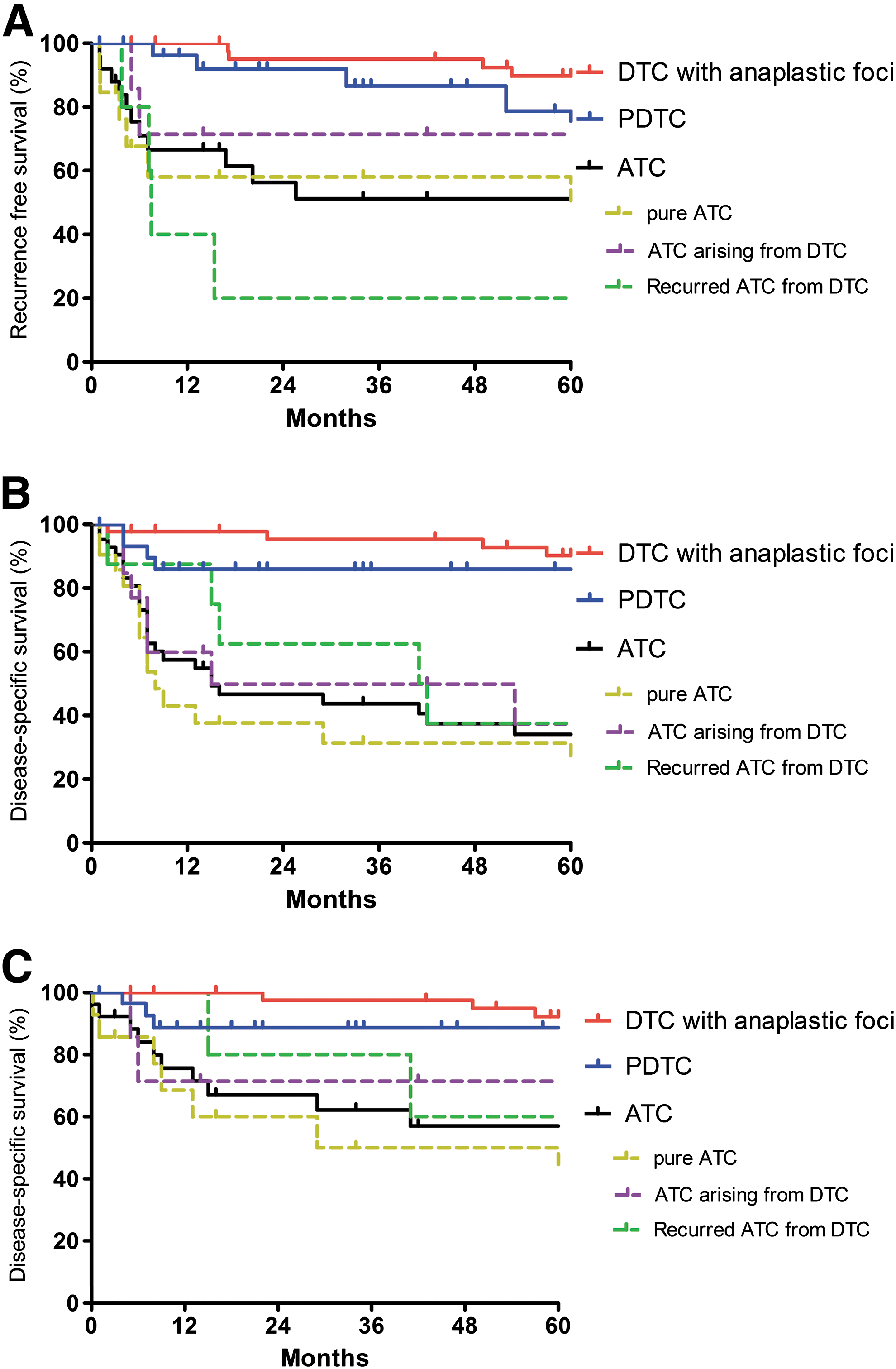
Recurrence-free survival (
Among the 18 patients with recurrence after initial remission, 16 died of the disease (duration after recurrence of 48.7 months). The death of 14 of these patients was from distant metastasis, and two died from locoregional failure. All 19 patients with absent initial remission died from locoregional failure during a median follow-up of 16.8 months (range 1–53 months) following the initial operation. Overall disease-specific mortality was 29.4%, and one- and two-year mortality rates were 19.3% and 23.5% in all patients, respectively, which was significantly higher in the patients with absent initial remission than it was in patients with initial remission (73.7% vs. 20%, respectively; p < 0.001). Both one- and two-year mortality rates were significantly higher in ATC than they were in DTC with anaplastic foci and PDTC (p < 0.001 and p < 0.001, respectively; Table 2 and Fig. 1B). The duration of survival was longer in DTC with anaplastic foci than it was in ATC or PDTC after recurrence. Among the ATC groups, the duration of survival of patients with absent remission after initial operation (median 5.0 months; range 1–7 months) or of patients with recurrence after initial remission (median 14.8 months, range 8–29 months) was shortest in pure ATC patients, while it was relatively long in patients with recurring ATC from DTC (20.0 months and 80.5 months, respectively; Table 2).
Clinical characteristics of patients with recurrence after initial remission
Overall, eight patients with ATC, three with DTC with anaplastic foci, and seven with PDTC had recurrent disease, with disease-free intervals of 6.3, 29.0, and 60.2 months, respectively (Table 3). The most common recurrence site was the lungs (11 patients; 61.1%), followed by the neck (locoregional recurrence; nine patients; 50.0%), then the liver or brain (two patients each; 11.1%). Total distant recurrence was observed in 14 patients (77.8%); six of them were found after (n = 3) or were concomitant with (n = 3) local recurrence, and the other eight displayed no local recurrence. The cause of death was failure of distant organs in all 14 patients. Exclusive locoregional recurrence was only found in four patients (nos. 7, 10, 14, and 18; 22.2%); all of these patients underwent reoperation, and two patients with PDTC (nos. 14 and 18) maintained a disease-free status for 30.5 and 161.1 months after reoperation, while the other two (one recurring ATC from DTC and one DTC with anaplastic foci) died from local failure despite surgery. Two patients with ATC were treated with palliative chemotherapy with Adriamycin, and one patient with recurrence in the buttocks and the brain underwent two operations in addition to chemoradiation therapy.
All recurrent tumors were anaplastic carcinomas.
38-year old female patients with PDTC, neck recurrence, which was cured with revision neck dissection and adjuvant radiation therapy.
46-year old female patients with PDTC, neck recurrence, which was cured with revision neck dissection.
Chemotherapy regimen: (1),(2)Adriamycin; (3)Sorafenib; (4)Adriamycin; (5),(6)unknown; (7)Paclitaxel with Carboplatin.
OP, operation; RT, radiation therapy; CTx, chemotherapy; RAI, radioactive iodine therapy.
Clinicopathologic factors associated with initial remission after surgery with curative intent
To determine the risk factors that can predict initial remission after curative-intent surgery, the clinicopathologic characteristics were compared between patients with initial remission versus absent remission after initial treatment (Table 4). Age, sex, pathologic diagnosis, pre-existing goiter or tumors, tumor size, and adjuvant treatment were the significantly different factors between the two groups (p = 0.001; p < 0.048, 0.001, 0.008, 0.042, and 0.001, respectively). White blood-cell (WBC) count, gross extrathyroidal extension, or initial cervical lymph node status, defined by preoperative CT or MRI and pathologic findings, revealed no significant differences between patients with initial remission and no initial remission. ATC patients had a higher proportion of failure to reach initial remission than patients with DTC with anaplastic foci or PDTC did (p < 0.001). However, there was no difference in reaching initial remission between the three ATC diagnostic groups (p = 0.826), although ATC arising from DTC showed a slightly higher rate of absent initial remission than the other groups did. Multivariate analysis failed to reveal the significant predictor for initial remission, probably due to the small number of patients with absent initial remission.
All continuous variables are expressed as means ± standard deviation (SD). All dichotomous outcomes are expressed number of patients and relative proportion (%) in the group. For pathologic findings, variables are expressed as number of patients/available samples and relative proportion (%). Statistically significant values are shown in bold.
Expressed as number and relative proportion in the same pathologic diagnosis.
WBC, white blood cells.
Clinicopathologic factors associated with recurrence after initial remission
For the analysis of predictive factors of recurrence after initial remission, the clinicopathologic characteristics of patients with NED were compared with those of recurrence among the subjects who achieved initial remission after surgery (Table 5). Pathologic diagnosis and pre-existing goiter or tumors were significantly correlated with recurrence (p < 0.001 and p = 0.001, respectively). Interestingly, tracheal invasion on CT/MRI and lymphatic/vascular invasion in pathologic findings were significantly different between the two groups (p = 0.006, 0.003, and 0.016, respectively). However, in contrast to the risk factors for the initial remission, age and sex revealed no significant differences between the patients with NED and with recurrence. Tumor size, WBC count, initial cervical lymph node status, gross extrathyroidal extension, and treatment modality were also not significantly different between the groups. Multivariate analysis failed to reveal the significant predictor for recurrence, probably due to the small number of patients with recurrence.
All continuous variables are expressed as means ± standard deviation (SD). All dichotomous outcomes are expressed number of patients and relative proportion (%) in the group. For pathologic findings, variables are expressed as number of patients/available samples and relative proportion (%). Statistically significant values are shown in bold.
Expressed as number and relative proportion in the same pathologic diagnosis.
Discussion
This study demonstrates the long-term outcome of patients with ATC or PDTC in which R0 or R1 resection was achieved after curative-intent surgery. The clinical course and prognosis mainly depended on the histologic subtypes; the cure rate was very high in DTCs with anaplastic foci (91.3%) or PDTCs (80.0%), while only 41.9% of patients with ATC were cured during the median five years of follow-up.
These data demonstrate that the rate of initial remission was lower in ATC (pure ATC, ATC arising from DTC, and recurrent ATC from DTC), and the incidence of recurrence was higher compared with other pathologic groups, with most recurrence developing early within one year. However, the initial remission was 60.5% in our resectable ATC subjects, showing that patients with resectable tumors could have a higher chance of initial remission of the disease than the entire (resectable plus unresectable) ATC population (16). In this study, however, further recurrence developed in 18.6% (8/43) of overall patients with ATC, that is, 30.8% (8/26) of the subjects with initial remission. Most recurrences in ATC patients developed with distant metastasis (87.5%), which is the main cause of death in these subjects. Local recurrences also occurred in half of the subjects, and only one (12.5%) subject presented with local recurrence without distant metastasis.
Although the initial remission rates were similar between the subtypes of ATC, recurrence rates and their characteristics were different. No recurrence was observed in ATC arising from DTC, while it occurred in 80.0% of subjects with initial remission in the subtype group where ATC recurred from DTC. Recurrence in pure ATC occurred in 28.6% of patients after the initial remission, which is lower than that of recurring ATC from DTC, but it developed earlier after surgery, and the duration before death was also shorter than in recurring ATC from DTC.
All these results suggest that of the different ATC subtypes, recurring ATC from DTC has the lowest chance of cure, with just a 12.5% of NED rate in this study, although the recurrence developed later and the survival was longer than it was in pure ATC. This may indicate that anaplastic transformation in the recurrent disease of DTC may show the highest potential of recurrence.
In the case of ATC arising from DTC, initial surgery can result in cure, and the duration of survival, even in subjects who were not cured, was longer than that in pure ATC, which suggests a more favorable prognosis of this category of ATC.
According to a previous study (10), resectability is the most important positive prognostic factor of ATC. Compared with the current study, survival duration of patients with resectable ATC who did not achieve initial remission was slightly longer than that of patients with unresectable ATC (10.7 months vs. 6.3 months). However, both patients with resectable ATC without initial remission and patients with unresectable ATC showed extremely high mortality rates compared with patients with resectable ATC who reached initial remission. Therefore, parameters associated with reaching remission after initial surgery of the resectable tumor may be critical in predicting treatment outcomes. Younger age, female sex, no history of preexisting goiter or tumors, and smaller tumor size showed a higher chance of reaching initial remission (Table 4). However, between the ATC groups, the only significant predicting factor for absent initial remission was age (p = 0.024; Supplementary Table S1; Supplementary Data are available online at
ATC typically has its peak of incidence in the 6th and 7th decades of life, and is associated with very poor prognosis, usually presenting with locally invasive disease and distant metastases at the time of diagnosis (17 –19). Several studies have emphasized that age is one of the significant prognostic factors for patients with ATC (8,16,20,21). However, after achieving initial remission, age itself was not a risk factor of further recurrence in this study. It was found that risk factors for recurrence were the subtype of ATC, tracheal invasion, and lymphovascular invasion, and these reflect the impact of locally invasive characteristics of the tumor. Although there were no significant variables between ATC subgroups due to the limited number of subjects, the present data suggest that tumors with microscopic invasive characteristics (lymphatic and vascular invasion) and gross invasive characteristics (tracheal invasion) may require more aggressive treatment modalities, such as super-radical surgery (22), additional radiation, or chemoradiation (23).
In the present cohort, DTC with anaplastic foci had a better prognosis than PDTC or ATC did. Although both DTC with anaplastic foci and PDTC showed a high initial remission rate, the recurrence rate in PDTC reached up to 25.9% during the median 86.2 months after initial remission, while it was only 6.7% during the median 66.3 months in DTC with anaplastic foci.
Subjects with absent initial remission (one DTC with anaplastic foci and one PDTC) had large infiltrative tumors. However, if it was possible to resect the tumor without residual gross or microscopic lesions, patients of these two categories (PDTC and DTC with anaplastic foci) had a significant chance of definite cure with surgery-based treatment (91.3% and 80.0%, respectively).
However, the recurrence rate of PDTC was comparable to ATC (24.1% vs. 30.8%), and was higher than that for DTC with anaplastic foci (6.7%). There was no relevant risk factor for recurrence of PDTC (Supplementary Table S2). In seven recurrent PDTC patients, six (85.7%) also had local recurrence, and only two subjects who presented with local recurrence could be cured after reoperation. However, the remaining subjects who had co-existing distant metastasis, or distant metastasis only, all died. Therefore, further investigations for the characterization of molecular markers and targeted therapies for metastatic lesions are necessary for PDTC, as well as for ATC.
Although most DTC with anaplastic foci are usually found incidentally after surgical resection of a predominantly non-anaplastic tumor (24 –26), the present data demonstrate that a small proportion of anaplastic foci may recur with more aggressive features at distant sites of metastasis. Therefore, physicians should carefully follow these patients for the detection of distant recurrences, especially in cases with older age, gross extrathyroidal extension, and lymphatic invasion (Supplementary Table S2).
PDTC also showed a better prognosis than ATC regarding both initial remission and definite cure rate in this study, although therapy-refractory metastatic disease was observed in five patients (15.6%), similar to the previous report by Ibrahimpasic et al. (27). They reported that with appropriate surgery and adjuvant therapy, excellent locoregional control can be achieved in PDTC, and disease-specific deaths mainly occurred due to distant metastases and rarely due to uncontrolled locoregional recurrence. The present data is in accordance with this report in that remission after initial treatment in PDTC was high (94.3%), with a low incidence of early locoregional recurrence, while the incidence of late distant metastasis was relatively high. The recommendations for postoperative adjuvant radiation remain controversial and need to be individualized. They are largely determined by the risk estimation of locoregional recurrence and the patients’ acceptance of locoregional toxicity. Considering the high locoregional control after radical surgery, it can be suggested that postoperative radiation therapy should be recommended for any patient where the physician states that gross disease is left either at the primary site or in regional lymph nodes (22,23).
In this study, there could be possible selection bias because several patients with more aggressive tumors were excluded in this study because some of the patients with untreatable tumors refused to undergo further evaluation. An additional limitation of this study is that the pathologic categorization could be incorrect in some patients whose surgical specimen was not available for the pathologic re-evaluation (n = 19). However, this study with ATC and PDTC is one of the largest cohorts in a single institute, thereby minimizing other confounding factors. The data are valuable in that the treatment outcomes and recurrence patterns of ATC and PDTC can be evaluated according to the various pathologic subgroups.
In summary, the rate of the initial remission of resectable tumors was higher in DTC with anaplastic foci and PDTC than it was in ATC. Age was significantly correlated with initial remission, and tracheal invasion and lymphovascular invasion were correlated with recurrence. More aggressive treatment and careful follow-up may be necessary for tumors with aggressive pathology, tracheal invasion, and lymphovascular invasion.
Footnotes
Acknowledgments
This study was supported by the Research Grant Number CB-2011-03-01 of the Korean Foundation for Cancer Research.
Author Disclosure Statement
The authors have nothing to disclose.