
Abstract
Background:
Marijuana is legalized for medical use in 24 states and for recreational use in 5. However, effects of marijuana use on thyroid function and autoimmunity are unknown.
Methods:
We performed a cross-sectional analysis of data from the National Health and Nutrition Examination Survey (NHANES) conducted between 2007 and 2012 to assess the effects of marijuana on thyroid function and autoimmunity in users. We included 5280 adults ages 18 to 69 years, who responded to questions related to marijuana use and had laboratory results related to thyroid parameters. Subjects were categorized as nonusers (never used), past users (used prior to 30 days ago), and recent users (used within last 30 days). Using NHANES normative cut offs for thyroid parameters, we compared recent users with nonusers and past users and calculated the odds ratios for the relative rate of clinically significant thyroid dysfunction in those groups. Multivariate logistic regression was then performed to control for confounders.
Results:
Fifty-four percent of subjects reported lifetime cannabis use, with 15% using it recently. Univariate regression analysis showed that recent marijuana users had significantly lower frequency of elevated thyrotropin (TSH) and positive anti-thyroperoxidase antibody (TPOAb) versus nonusers/past users. After controlling for confounders, recent marijuana use remained an independent predictor for TSH <5.6 μIU/mL (odds ratio of 0.344 with 95% CI of 0.127–0.928; p = 0.04) but not for negative TPOAb.
Conclusion:
Recent marijuana use was not associated with thyroid dysfunction but was significantly associated with lower levels of TSH.
Introduction
M
With respect to thyroid function, there are very limited published data available, mostly from animal experiments. The first study, published in 1965, reported that the administration of marijuana to rats leads to reduced iodine accumulation in the thyroid (2,3). Subsequently, in 1970 Lomax et al. showed that systemic injection of marijuana's active compound Δ9-tetrahydrocannabinol (Δ9-THC) in rats inhibits the hypothalamus, leading to suppression of thyrotropin (TSH) (4). Hillard et al. also reported similar findings after the intraperitoneal injection of Δ9-THC to rats with a dose-dependent decrease in circulating TSH, as well as thyroid hormone levels (5). In human subjects there are only two limited studies available; one study on chronic marijuana users at a detoxification center showed lower thyroxine (T4) levels in chronic users 10–14 days after abstinence; however, TSH levels were similar as in the controls. This study did not examine the effects during active marijuana use (6). Another uncontrolled study examined the thyroid profile of 24 chronic marijuana users and found them to be all within the normal population reference range (7).
Due to current federal restrictions on human research related to marijuana, we elected to evaluate data available from the National Health and Nutrition Examination Survey (NHANES) from 2007 to 2012 conducted by the Centers for Disease Control. Our primary objective was to explore the impact of marijuana use on thyroid function parameters, including free triiodothyronine (fT3), free thyroxine (fT4), TSH, anti-thyroglobulin antibody (TgAb), and anti-thyroperoxidase antibody (TPOAb). Furthermore, the effect of cannabis on thyroid autoimmunity has never been evaluated, while several studies on subjects with other autoimmune conditions, including rheumatoid arthritis and multiple sclerosis have suggested an immune modulatory potential for cannabis (8,9). Autoimmune thyroiditis is the leading cause of hypothyroidism that clinically presents as positivity of TPOAb and/or TgAb, and elevation of TSH combined with low circulating levels of thyroid hormones. Therefore, evaluation of the effect of marijuana on thyroid autoimmunity was an important secondary objective for this study.
Materials and Methods
Study population
The NHANES is a program of studies designed to assess the health and nutritional status of adults and children in the United States. The survey employs a complex, multistage probability sampling design to select a nationally representative sample of individuals in the United States' population and uses interviews, physical examination, and laboratory components to assess health and nutritional status. The NHANES survey design oversamples certain subgroups of individuals (e.g., adolescents and minority individuals) to ensure adequate representation of these groups. Descriptions of the survey, sampling procedures, and details of the laboratory tests evaluated can be found on the Centers for Disease Control and Prevention website (
For this study, we merged three waves of NHANES to maximize power: NHANES 2007–2008 (“E” data), NHANES 2009–2010 (“F” data), and NHAHES 2011–2012 (“G” data). We included data related to subjects aged 18–69 years who participated in questionnaires regarding marijuana use. To assess the effect of recent marijuana use on thyroid parameters and autoimmunity, we focused on data related to timing and amount of marijuana use.
Marijuana use assessment
NHANES data on marijuana use were based on self-report. Subjects were asked the following questions, using the audio computer assisted personal self-interview at the mobile examination center MEC: (i) Have you ever, even once, used marijuana or hashish? Answers were recorded as yes, no, refused, or don't know. (ii) How old were you the first time you used marijuana or hashish? Answers were recorded as age in years, responses not to exceed number 69. (iii) How long has it been since you last used marijuana or hashish? Answers were given as number of days, weeks, months, or years. (iv) During the past 30 days, on how many days did you use marijuana or hashish? Answers were recorded as numbers, not exceeding 30.
Responses to these questions were used to classify participants into three categories: nonusers were those who reported that they had never used marijuana; past users were those who reported using marijuana, but had not used marijuana in the past 30 days; and current or recent users were those who reported using marijuana in the past month, no matter how frequent.
Thyroid outcomes
The thyroid profile includes several tests for the measurement of thyroid function, including fT3, fT4, TSH, TPOAb, and TgAb. From 2007 to 2008, thyroid blood specimens were processed, stored, and shipped to the University of Washington. For the subsequent NHANES data set from 2009 to 2010 and 2011 to 2012, the samples were additionally sent to Collaborative Laboratory Services. Testing was done using the Beckman Access or Access II Immunoassay System (Beckman Coulter).
The TSH assay used by NHANES is a third generation two-site immunoenzymatic (“sandwich”) assay with the normative reference range of 0.34–5.6 μIU/mL. The fT4 assay is a two-step enzyme immunoassay with a normative reference range of 0.6–1.6 ng/dL. The fT3 assay is a competitive binding immune enzymatic assay with a normative reference range of 2.5– 3.9 pg/mL. Similarly, the assays for TPOAb and TgAb are two-step immune enzymatic “sandwich” assays with reference ranges of 0–9.0 IU/mL and 0–4.0 IU/mL respectively. To evaluate prevalence and odds ratio, we used cut-off values recommended by NHANES to define normal and abnormal values for TSH, fT3, fT4, and thyroid antibodies. An abnormal low TSH was defined as TSH <0.34 μIU /mL; elevated as TSH >5.6uIU/mL; similarly, low fT3 as <2.5 pg/mL; low fT4 < 0.6 ng/dL; antibody positivity was defined as TPOAb >9.0 IU/mL and TgAb >4.0 IU/mL.
The NHANES survey has data related to self-reported thyroid disease (in general without specifications), as well as self-reported data related to prescription use, including use of levothyroxine and liothyronine. Since type of thyroid disease was not specified in the survey, we decided to include information related to the use of levothyroxine and liothyronine as markers of possible hypothyroidism.
Statistical analyses
SAS 9.3 (SAS Inc.) was used for all analyses since it incorporates appropriate sampling weights to adjust for the complex sample design in order to produce corrected estimates of standard errors. SAS procedures PROC SURVEYFREQ, PROC SURVEYMEANS, PROC SURVEYREG, and PROC SURVEYLOGISTIC were used for the primary descriptive results and statistical testing. All analyses applied two-sided tests with a significance level <0.05. Sampling weights were calculated for the three consecutive waves of data that were merged together, as recommended by NHANES.
Data were described in terms of weighted mean and standard error adjusted for sampling weights in the case of normally distributed data (e.g., age), in terms of median and 95% confidence limit estimated from weighted frequencies for skewed data (e.g., TSH), and in terms of actual frequency and weighted percent for categorical data (e.g., sex). Both TPOAb and TgAb were categorized as below and above clinical thresholds due to severe non-normality or truncation of range. Univariate analysis was done using SAS PROC SURVEYREG for group comparisons of means and using PROC SURVEYFREQ for group comparisons of rates based on the Rao-Scott chi-squared test. Further chi square analyses were done to look at clinically significant levels of thyroid parameters in recent users (<30 days).
Based on dichotomous marijuana usage (never/>30 days user versus recent user), we then performed univariate logistic regression analyses using SAS PROC SURVEYLOGISTIC to predict the presence of clinically significant levels of TSH (below or above reference range), and TPOAb positivity. Odds ratios to compare the relative rate of clinically significant levels of TSH (elevated TSH, >5.6 uIU/mL) and TPOAb (positive TPOAb, >9.0 IU/mL) in recent users versus other users were estimated from results of the b-coefficients of the logistic regression. This was done to assess the risk of hypothyroidism (elevated TSH) and autoimmune hypothyroidism (positive antibodies) in recent users and to see if marijuana use is protective against the disease. Multivariate logistic regression models were then done to determine whether the odds ratios for marijuana usage changed after controlling for possible confounders (e.g., age, sex, and white ethnicity for antibody positivity, and body mass index [BMI] and use of levothyroxine and liothyronine for TSH levels). As a sensitivity analysis, multiple imputations were carried out using SAS PROC MI and PROC MIANALYZE. Five imputations per model were performed and averaged to replicate the analyses that were based on nonimputed data as well as to verify that results for the multivariate models based on the nonimputed data were not affected by any bias or lack of power as a result of missing data in the control variables.
Results
Subjects and demographic characteristics
A total of 5280 subjects responded to the NHANES questionnaire regarding marijuana use. For the main analysis, we only included subjects with complete data regarding cannabis use and individual thyroid levels of interest. Approximately 54.5% (2878) of the total subjects reported cannabis use at some point during lifetime, with 45.5% (2402) of subjects reporting that they have never used marijuana. Of the total marijuana users, 28.5% (821 subjects) reported recent use (within the last 30 days) and 71.4 % (2057 subjects) reported past use (prior to the last 30 days).
Demographic characteristics of the groups are shown in Table 1. Age, sex, ethnicity, and BMI are presented as adjusted weighted mean and standard deviation, and thyroid variables are presented as weighted median and standard deviation. Overall, recent marijuana users (<30 days) were significantly younger and had lower BMI means as compared with the other two groups of past users (>30 days) and the non-marijuana users (never used marijuana). Past users/non-marijuana users reported a significantly higher rate of thyroid hormone (levothyroxine and liothyronine) intake compared with the recent users, suggesting a higher prevalence of hypothyroidism among past users/non-marijuana users compared with recent marijuana users (4.4% versus 1.8%; p = 0.009) (Table 1). In terms of sex, the recent marijuana user group had a higher number of males than females compared with the other two groups. As shown in Table 1, there were significant differences between median levels of TSH (p < 0.001) and fT3 (p < 0.001) as well as the rate of positive TPOAb among the three user groups (p = 0.04).
Actual frequency (weighted percentage).
Weighted mean (standard error) [95% CI for mean].
Weighted median [95% CI for median].
BMI, body mass index; fT3, free thyronine; fT4, free thyroxine; TgAb, anti-thyroglobulin antibody; TPOAb, anti-thyroperoxidase antibody; TSH, thyrotropin.
Marijuana use and thyroid variables
To assess the specific effect of current marijuana use, we then combined the two groups of nonusers (never used) and past users (used marijuana prior to 30 days ago), and compared them with the group of recent users (used marijuana in the last 30 days) as a separate analysis (Fig. 1). This was clinically relevant since after any exposure, changes in thyroid function (T3 and T4 hormones), and even TSH typically equilibrate within 4 weeks. Therefore, the recent users group (i.e., used marijuana within past 30 days) is thought to be a clinically distinct group in terms of thyroid effects versus the past user group, which was inclusive of all subjects who reported any lifetime marijuana use, even decades prior to the study. When we compared the combined group of nonusers/past users with the recent users in terms of prevalence of abnormal TSH, fT3, and TPOAb positivity, the rate of subjects showing positive TPOAb (>9 IU/mL) and an elevated TSH (>5.6 μIU/mL) were significantly higher among nonusers/past users compared with recent users (Table 2, Fig. 1). When rates of abnormal low TSH (based on the cutoff <0.34 μIU/mL) were compared between nonusers/past users and recent users, the rate of a low or suppressed TSH (<0.34 μIU/mL) in both groups was not different (1.61 % versus 1.60 % respectively). In addition, frequencies of abnormal fT3, fT4, and TgAb positivity were not significantly different between the two groups based on the univariate analysis with NHANES specified cutoff values to define abnormal function.
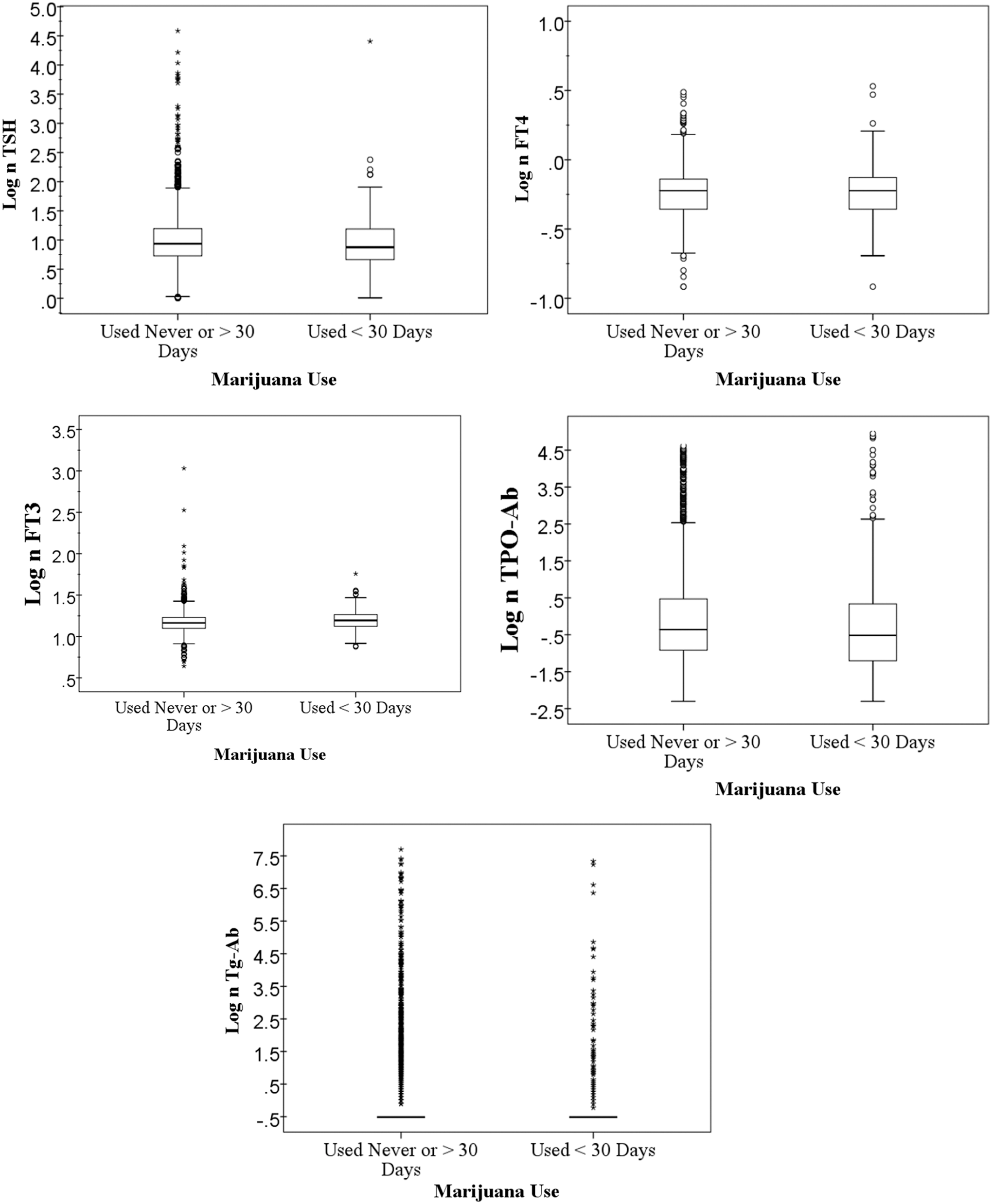
Box plots of natural log transformed of thyroid parameters. Panels show a natural log transformed of each thyroid parameter on the y axis. On the x axis marijuana groups are shown; combined past and never marijuana user groups (never/>30 days) on the left side and recent marijuana users (<30 days) on the right side. Boxplots show the median (middle line of box); interquartile range (top and bottom of box); top and bottom whiskers which extend an additional ±1.5 × interquartile range from box; and outliers which are ≥3.0 × interquartile range. Over 80% of subjects in each sample were below the lower limit of TgAb assay (0.9 IU/mL). Therefore, median, 25th percentile and 75th percentile all equal to one another and interquartile range = 0. This explains the lack of a box in the plot for TgAb. TSH, thyroid stimulating hormone; fT3, free triiodothyronine; fT4, free thyroxine; TPOAb, anti-thyroperoxidase antibody; TgAb, anti-thyroglobulin antibody.
Frequency (weighted percentage).
Since the earliest manifestations of compensated autoimmune hypothyroidism (mildest form of hypothyroidism) are positive thyroid antibodies and elevated TSH, we compared the odds ratio of elevated TSH and TPOAb positivity of the recent users group to the nonusers/past users group, as shown in Table 3. Univariate logistic regression analyses indicate that recent cannabis use was a significant predictor for a normal TSH values <5.6uIU/mL and negative TPOAb (<9 IU/mL). Several reports have indicated that TSH is elevated in obese subjects (10 –12) and rises with aging (13,14). In addition, it is known that autoimmune thyroiditis increases with aging, and is more common among women and in white population (13,14). Yet another potential confounder was the use of thyroid hormone (levothyroxine and liothyronine) that could affect the TSH level but is also an indicator of a history of hypothyroidism. Since hypothyroidism was one of our study outcomes, we did not exclude subjects on thyroid hormone but included the use of thyroid medication as a confounding factor to control in our multivariate analyses of TSH.
Multivariate model controlling for age and BMI, and thyroid medication.
Multivariate model controlling for age, sex, white ethnicity, and thyroid medication.
In a multivariate model for TSH, the odds ratios comparing recent users relative to nonusers/past users after controlling for the use of thyroid hormone, BMI and age remained significant (OR 0.344 [CI 0.127–0.928]; p = 0.04) (Table 3). In contrast, while the univariate analysis based on unimputed data showed that recent marijuana use was significantly predictive of negative TPOAb (p = 0.04), the multivariate analysis after controlling for age, sex and white ethnicity was no longer significantly associated with TPOAb in recent users (p = 0.36). Sensitivity analyses based on imputed data for TSH and TPOAb missing data showed similar results and confirmed our findings (OR 0.359 [CI of 0.149–0.863], p = 0.02, and OR 0.699 [CI of 0.452–1.08], p = 0.11, respectively).
Discussion
We found that subjects who reported recent marijuana use within the past 30 days have significantly higher frequency of TSH in the normal range (<5.6 uIu/mL) after controlling for confounders. Of note, the rate of suppressed TSH below the lower limit of normal or <0.34 μIU/mL was not significantly different in recent marijuana users. Other thyroid parameters were similar when we compared the two groups.
Subclinical hypothyroidism presents as only elevated TSH level with normal fT3 and fT4 (15) and is an important entity that may be linked to adverse cardiovascular risk factors such as alterations in blood pressure, lipid levels, and atherosclerosis. (16) Therefore, our findings may suggest that recent cannabis use is either protective for subclinical hypothyroidism, or the lower TSH level seen among recent marijuana users may be due to hypothalamic suppression of TSH as noted in prior animal studies. The NHANES data do not allow the elucidation of an exact mechanism.
Currently, there are no controlled studies on the effect of marijuana on thyroid function in human subjects who are active users. Pioneering studies in rodents noted that cannabis exposure may lead to suppression of TSH and hypothalamic function (4,5). The first study, by Lomax et al., reported that injection of marijuana's active compound Δ9-THC inhibits the release of radioiodine from the thyroid gland of the rat. Administration of TSH reversed this effect and resulted in increased output of iodine in animals pretreated with Δ9-THC. The authors concluded that reduced TSH secretion was the primary cause of the thyroid inhibition induced by marijuana. Furthermore, in the same experiment bilateral electrolytic lesions in the region of medial mammillary nuclei of hypothalamus eliminated the decrease in thyroid function, suggesting a hypothalamic origin (4). The second pioneering report by Hillard et al. showed that Δ9-THC administration decreases the circulating TSH, as well as thyroid hormones, with a maximal effect at 10 mg/kg dose. The effect was abolished when exogenous thyrotropin-releasing hormone was administered to rats pretreated with Δ9-THC, suggesting that marijuana's active component may inhibit thyrotropin-releasing hormone release from the hypothalamus (5).
However, recent reports in rodents are conflicting and hypothalamic suppression by marijuana may not be the sole potential mechanism for decreased TSH. One study by Porcella et al. from 2002 was not able to show the same decrease in TSH using the synthetic cannabinoid receptor type 1 (CB1) agonist WIN 55,212-2 in rats (17), but another study using anandamide (another potent CB1 agonist) in rats showed suppression of TSH and T4 after treatment (18). In humans, CB1 receptors have been identified on corticotrophs, mammotrophs, somatotrophs, and folliculostellate cells of the anterior lobe of the normal pituitary, but there is no data specifically related to thyrotropes (19). Overall, the data related to human subjects is sparse. Therefore, pathophysiologic mechanisms are speculative, although animal data support potential mechanism of hypothalamic suppression.
Secondarily, we compared the groups with respect to thyroid autoimmunity. Endocannabinoids seems to have an important immunomodulatory function. Of the two well recognized cannabinoid receptors (20 –22), cannabinoid receptor 2 seems to be primarily involved in immune function, and is expressed by hematopoietic cells (22,23). The effect of marijuana use on the immune system and autoimmunity has been explored previously in other conditions, such as rheumatoid arthritis, colitis, and hepatitis (8,9). Marijuana is even being investigated as a treatment modality for certain autoimmune disorders (24), but its effect on thyroid autoimmunity is entirely unknown. Since thyroid autoimmunity is the most common underlying pathophysiology leading to hypothyroidism (25), the effect of marijuana use on thyroid autoimmunity was another important aspect of this study.
Our initial analysis suggested that prevalence of thyroiditis may be lower among recent users compared with nonusers/past users, as demonstrated by the lower rate of TPOAb positivity in this group. However, after controlling for confounders such as age, white ethnicity and female sex, the differences in TPOAb were no longer significant. Due to other published reports on the positive role of marijuana in treatment of autoimmune conditions, it may be worth revisiting the association of marijuana use and thyroid autoimmunity in future controlled prospective studies.
Overall, this study is the first to examine the effect of current marijuana use on thyroid function and autoimmunity in human subjects. Our study suggests that marijuana use, at least in short term, is associated with lower levels of TSH. This finding may indicate a protective role against hypothyroidism or could also be due to hypothalamic suppression of TSH. Unfortunately, analysis of the NHANES data does not allow clarification of these potential hypotheses, since much of the data are based on self-report and also lack certain relevant clinical data such as family history. Another potential weakness may be due to the relatively small number of subjects responding to the NHANES questions regarding marijuana use. This probably underestimates the actual prevalence of cannabis use in the general population and may also have reduced our ability to detect differences between our groups. There are few published human studies and with the rapid pace of legalization of marijuana use, there is a significant gap in this area. Therefore, future prospective clinical studies evaluating potential effects of marijuana use on the hypothalamic-pituitary-thyroid axis and other hormonal axes in human subjects are needed.
Footnotes
Acknowledgment
Support for this work was provided by the Maimonides Research Foundation.
Author Disclosure Statement
No competing financial interests exist.