
Abstract
Background:
Iodine deficiency is a major public-health problem throughout the world, especially for pregnant women, and it is considered the most common cause of preventable intellectual impairment. In the United States, iodine status in pregnant women is considered mildly deficient. Therefore, the Endocrine Society, the American Thyroid Association, the Teratology Society, and the American Academy of Pediatrics recommend that women receive prenatal vitamins containing 150 μg of iodine daily during preconception, pregnancy, and lactation. The objectives of this study were to evaluate awareness of iodine nutrition among obstetricians and midwives in the United States, and to document current clinical practice regarding recommendations for iodine supplementation for women during preconception, pregnancy, and lactation.
Methods:
All midwife members of the American College of Nurse-Midwives (ACNM) and all obstetrician members of the American Medical Association (AMA) were invited to participate in a web-based survey.
Results:
A total of 199 midwives and 277 obstetricians participated in the survey. One third of both obstetricians and midwives considered iodine status in U.S. pregnant women to be deficient. Although almost all obstetricians and midwives would recommend prenatal multivitamins, most reported rarely or never recommending iodine-containing multivitamins for women planning pregnancy (68.7% and 70.2%, respectively), pregnant women (66% and 67.1%), or lactating women (68.7% and 71.7%). Of the respondents who did report prescribing iodine-containing supplements, 85% recommended supplementation during the first trimester and 75–80% during the second and third trimesters. However, of those who did recommend iodine supplementation, only 45% would prescribe the recommended 150 μg of iodine daily during pregnancy. Overall, 75% of U.S. obstetricians and midwives do not recommend or would recommend an inadequate amount of iodine during preconception, pregnancy, and lactation.
Conclusions:
Despite the important consequences of iodine deficiency for pregnant women and the recommendations of many medical societies, the majority of U.S. obstetricians and midwives who participated in this survey do not recommend iodine-containing vitamins in women planning pregnancy, during pregnancy, and during lactation.
Introduction
I
Several studies have demonstrated associations between iodine deficiency and impaired child neurodevelopment. The Avon Longitudinal Study of Parents and Children, performed in the United Kingdom, reported that children of women with iodine-to-creatinine ratios of <150 μg/g during pregnancy had a significant increased risk of lower verbal intelligence quotient (IQ) at eight years of age and of lower reading accuracy and reading comprehension scores at nine years of age (3). In a meta-analysis, it was shown that children of mothers residing in iodine-deficient areas had a lower IQ by 12.45 points compared with children who lived in an iodine-sufficient environment. Moreover, there was an 8.7-point increase in IQ in children whose mothers resided in areas where iodine supplementation was implemented (4). Another more recent meta-analysis, which aimed to ascertain how iodine status affects mental development of children aged five years and younger, concluded that iodine deficiency is responsible for the loss of 7.4 IQ points in children experiencing iodine deficiency in utero and in early infancy. Therefore, the authors underlined the importance of supplementation with iodine before and during pregnancy, especially in early pregnancy (5).
Iodine deficiency is common throughout the world, and is considered the most common cause of preventable mental impairment worldwide (6). According to data from the National Health and Nutrition Examination Surveys (NHANES 2005–2010), the median urinary iodine concentration (UIC) in U.S. pregnant women was below the World Health Organization (WHO) threshold for sufficiency (7). The American Thyroid Association (ATA) (8,9) and the WHO (10) recommend that pregnant and lactating women ingest approximately 250 μg of iodine daily. To achieve this goal, the ATA guidelines for the diagnosis and management of thyroid disease during pregnancy and postpartum recommend that women receive prenatal vitamins containing 150 μg of iodine daily during preconception, pregnancy, and lactation (9). Other societies, such as the Teratology Society (11), the Endocrine Society (12), and the American Academy of Pediatricians (13), have concurred with this recommendation. Indeed, since iodine deficiency in populations is easy to prevent and monitor, the persistence of iodine deficiency among pregnant U.S. women may be due to education programs that are not sufficiently effective and to a lack of awareness among healthcare professionals. Data from NHANES (2001–2006) showed that only 20% of pregnant and 15% of lactating women were taking a supplement containing iodine (14). The purpose of this study was to evaluate awareness of iodine nutrition among obstetricians and midwives in the United States, and to ascertain current clinical practices regarding recommendations for iodine supplementation for women during preconception, pregnancy, and lactation.
Materials and Methods
Survey design
Two online surveys were designed using the Survey Monkey® program (Palo Alto, CA). The two surveys had similar questions for obstetricians and midwives. The surveys included 21 questions, with the first six questions pertaining to demographic information (see Supplementary Data available online at
All questions were multiple choice, with one single best answer to be selected, except for one question where more than one answer was allowed (question 17). Respondents were not allowed to go back to previous questions to review or edit their responses. Questionnaire completion time was estimated to be 5–10 minutes. Respondents were allowed to submit answers within a six-month period from June to December 2015.
Contact of potential respondents
All obstetrician members of the American Medical Association (AMA) and the members of the American College of Nurse-Midwives (ACNM) received an e-mail containing an electronic link to the survey Web site. The e-mail was deployed three times to obstetricians by Redi-Mail® (AMA Database Licensees), and twice to midwives by the ACNM. Each time, respondents who had already answered the questionnaire were omitted. The surveys were approved by both Redi-Mail® and the ACNM, and the study was determined to be exempt by the Boston University Medical Center Institutional Review Board, since the research involved the use of survey procedures and respondents' anonymity was preserved.
Results
Response rate
The e-mail was delivered to 5220 midwives and opened by 350/5220 (6.7%), and was delivered to 21,215 obstetricians and opened by 2524/21,215 (11.9%). Four hundred and seventy-six respondents participated in the survey: 199/350 midwives (57% response rate) of whom 189 (95%) answered all the questions, and 277/2524 obstetricians (11% response rate) of whom 258 (93%) answered all the questions. In summary, 3.6% (189/5220) of all midwives and 1.2% (258/21215) of all obstetricians completed the survey.
Respondents demographic
Two thirds (63.5%) of obstetricians were women, while almost all midwives were women (99.5%). Both obstetricians and midwives were similarly distributed according to age, years of clinical practice after completing training, and practice type and setting (Table 1). All respondents except two midwives (1%) worked in the United States.
Iodine status and iodine supplementation
Only 34.8% of obstetricians considered the iodine status of U.S. pregnant women as deficient, while 46.7% believed it was adequate, and 13% did not know. Similarly, 43.4% of midwives considered it deficient, and 32.1% thought it to be adequate, while 15.3% did not know (Fig. 1). Two-thirds of both obstetricians and midwives correctly believed that iodine deficiency in pregnant women might be harmful for the fetus. Iodine supplementation was considered useful for U.S. women of childbearing age and pregnant women by approximately 60% of both obstetricians and midwives. One third of both obstetricians and midwives did not recommend that their patients use iodized salt, while another third recommended it often or always.
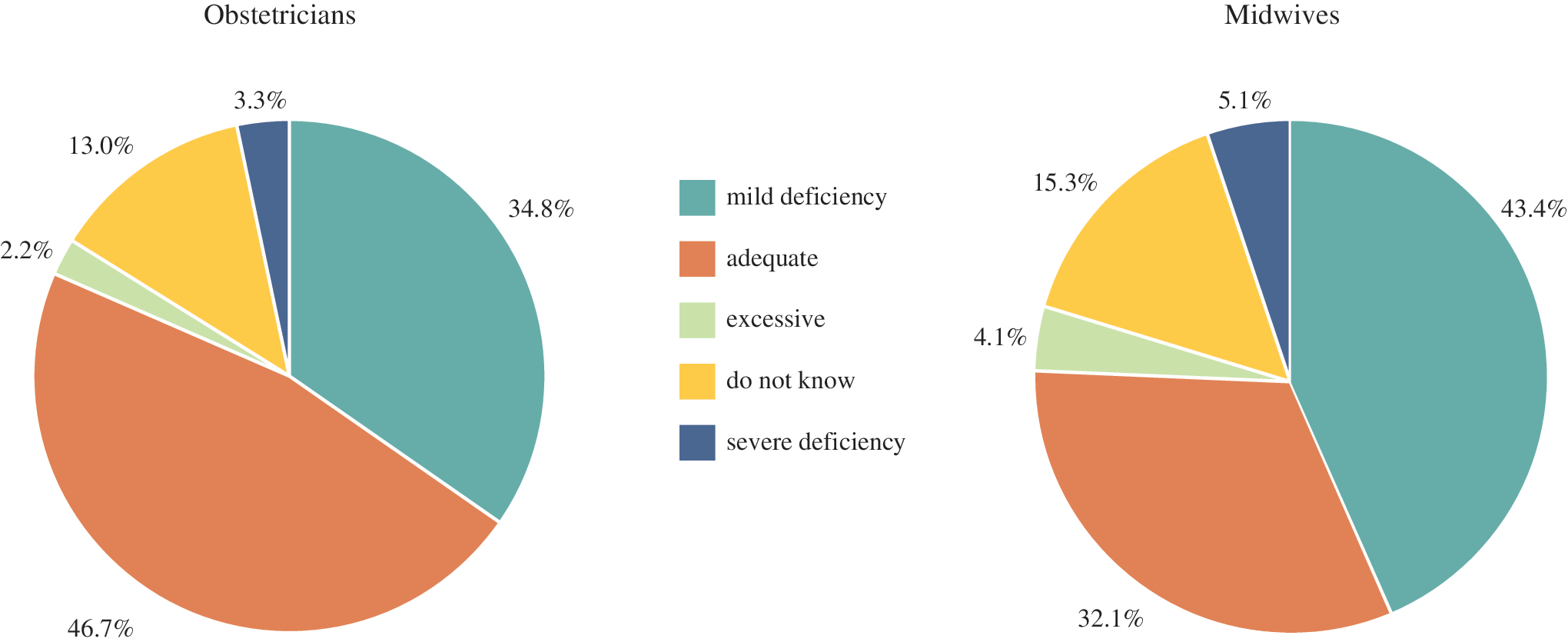
Responses of obstetricians and midwives concerning the iodine status of U.S. pregnant women (correct answer: “mild deficiency”7). Color images available online at
Prenatal multivitamins recommended
The survey asked the respondents first if they recommended prenatal multivitamins for women planning pregnancy, pregnant women, and lactating women, and then if they specifically recommend iodine-containing prenatal multivitamins. Prenatal multivitamins were widely recommended by both obstetricians and midwives. Almost all obstetricians and midwives would often or always recommend prenatal multivitamins for women planning pregnancy (96.2% and 95.3%, respectively), for pregnant women (98.5% and 95.8%), and for lactating women (98.1% and 93.7%). In contrast, most obstetricians and midwives would rarely or never recommend iodine-containing prenatal multivitamins for women planning pregnancy (68.7% and 70.2%, respectively), for pregnant women (66% and 67.1%), or for lactating women (68.7% and 71.7%; Fig. 2).
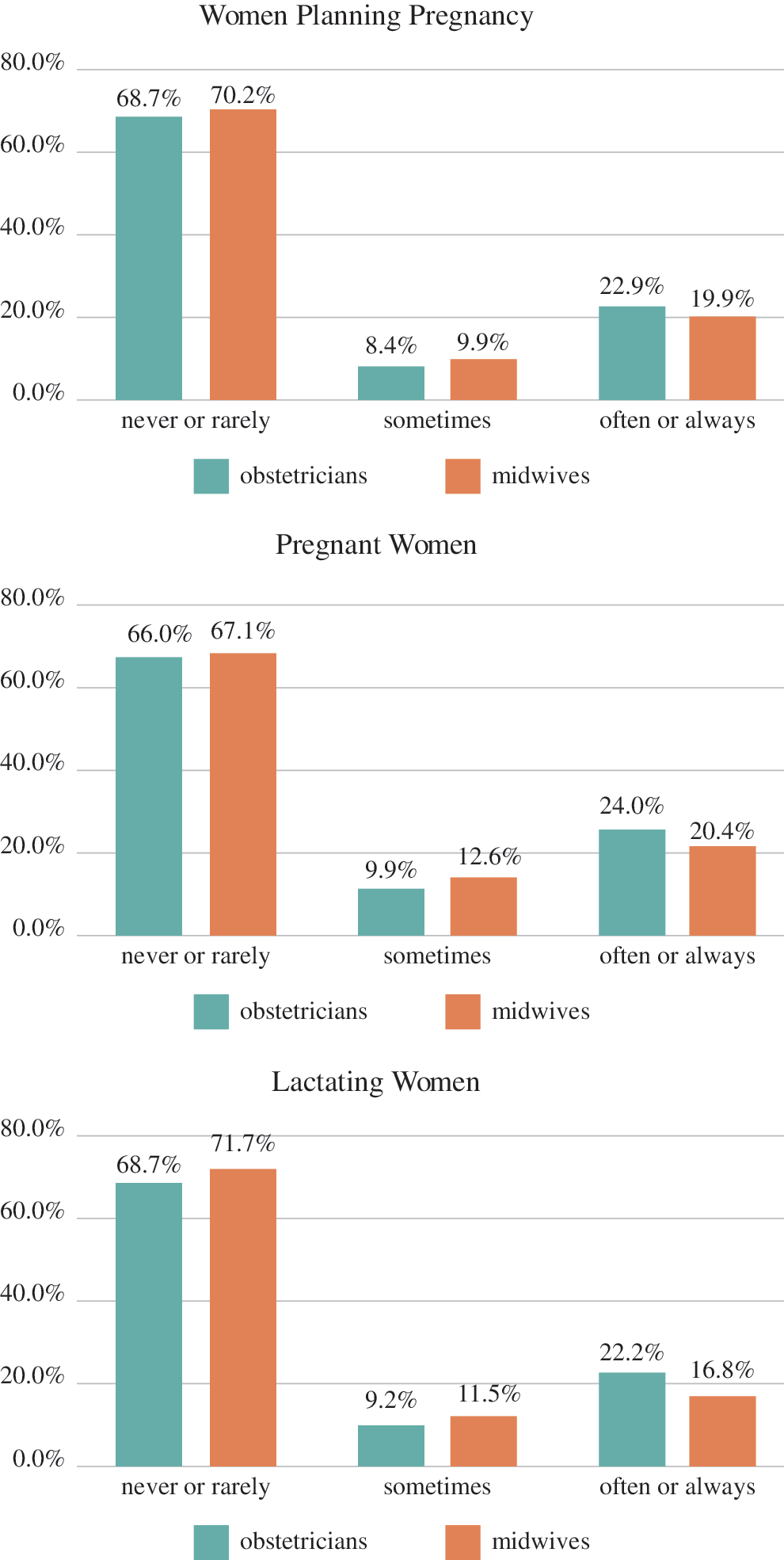
Frequency of recommendations by obstetricians and midwives to iodine-containing prenatal multivitamins in women planning pregnancy, pregnant women, and lactating women. Color images available online at
When iodine is recommended
Among respondents who recommended iodine-containing supplements, approximately 85% of both obstetricians and midwives would prescribe them during preconception and during the first trimester of pregnancy; 80% of obstetricians and 75% of midwives would recommend them during the second trimester; 77% of obstetricians and 75% of midwives during the third trimester; and 71% of obstetricians and 67% of midwives during lactation.
Amount of iodine
Of those who did recommend iodine supplementation, only 45% of respondents recommended 150 μg of iodine daily. In particular, 150 μg of iodine daily was recommended during preconception by 52.7% and 59.3% of obstetricians and midwives, respectively; during pregnancy by 44% and 43.5%; and during lactation by 42.5% and 34.5%. A total of 30% of obstetricians would recommend 250 μg of iodine daily during preconception, pregnancy, and lactation, while about 15% would recommend an inadequate dose of 50 μg of iodine daily during the three phases. Among midwives, 22% and 27% would recommend 50 μg and 250 μg of iodine daily, respectively, during the three phases (Fig. 3).
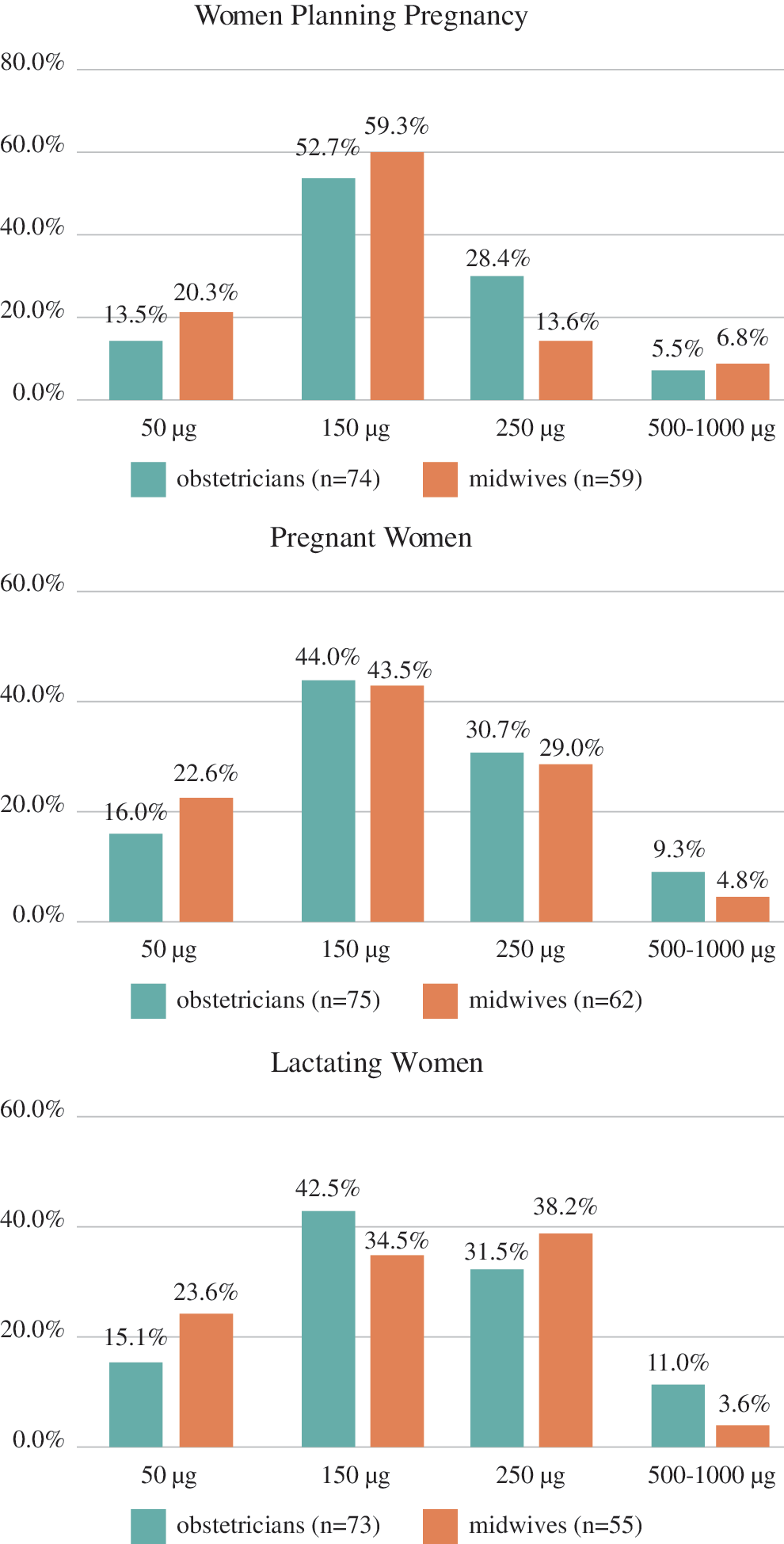
Daily iodine dose recommended after exclusion of respondents who would not recommend iodine-containing multivitamins. Color images available online at
Taking all respondents into account, 75% of both obstetricians and midwives would not recommend or would recommend an inadequate amount of iodine supplementation to U.S. women during preconception, pregnancy, and lactation. Thus, an adequate dose of 150 μg of iodine daily would be prescribed during preconception only by 15.1% and 18.5%, during pregnancy by 12.8% and 14.3%, and during lactation by 12% and 10.1% of obstetricians and midwives, respectively.
Discussion
The current study demonstrates that the majority of U.S. obstetricians and midwives who responded to this survey do not recommend or recommend an inadequate daily dose of iodine in women planning pregnancy, in pregnant women, and in breastfeeding women. Although almost all respondents would recommend prenatal multivitamins during preconception, pregnancy, and lactation, few would specifically recommend those containing iodine. Answers from obstetricians and midwives were similar. This failure to recommend iodine supplementation routinely may be due to the absence of specific guidelines of some obstetrical and midwifery societies, including the American Congress of Obstetricians and Gynecologists and the ACNM, and to a lack of knowledge about the iodine status of U.S. pregnant women. Indeed, almost a half of respondents wrongly believed that the iodine status of U.S. pregnant women is adequate, and one third did not know or thought iodine deficiency was not harmful for the fetus.
To the authors' knowledge, this is the first study aimed at ascertaining obstetrician and midwife knowledge about iodine supplementation in the United States. Other studies have been performed in Australia, Turkey, and the United Kingdom, with similar results. Australia is mildly iodine deficient, and the National Health and Medical Research Council there recommended that all women planning pregnancy, pregnant, or breastfeeding take iodine supplements containing 150 μg of iodine daily (15), which is similar to the U.S. guidelines. In Australia, both pregnant women and healthcare professionals (general practitioners and nurses) were surveyed. A total of 65% of healthcare providers reported that they did not prescribe iodine-containing supplements to pregnant women, although the majority of women reported that they were taking supplements containing iodine (16). This may be because most prenatal multivitamins in Australia contain iodine. Another study conducted in Australia, with a similar proportion of women taking iodine-containing supplements, reported that only half of the women surveyed were taking the correct amount of iodine (17). A recent review from Australia reported limited basic nutrition knowledge on the part of midwives (18). Turkey is a mildly iodine-deficient country. Among Turkish obstetricians who were surveyed, only 20% considered iodine supplementation necessary or knew the adequate daily iodine dose of supplementation in pregnant women (19). A recent study conducted in the United Kingdom surveyed women who were pregnant or who had had a recent pregnancy regarding their awareness of iodine supplementation in pregnancy. British pregnant women and those of childbearing age are currently considered mildly iodine deficient (20,21). Only 64% of the women surveyed had ever received information about iodine supplementation, and only 11% reported that they had been informed about iodine by healthcare professionals (22). These studies, together with the current findings, highlight a lack of knowledge by obstetricians, midwives, and pregnant women, underlining the need for more adequate nutrition education programs.
This study has some limitations. First, the survey response rate was quite low, so that only a small proportion of active members of the AMA and the ACNM participated in the survey, and respondents therefore may not have been representative. Nevertheless, demographic information shows that all ages, geographic areas of the United States, and type of practice setting were represented. Second, the survey did not include general questions about iodine nutrition and dietary iodine intake. Some might argue that respondents would recommend an adequate intake of iodine with foods instead of oral supplements, but this is unlikely. Indeed, only one third reported often or always recommending iodized salt, which is the easiest way to increase iodine intake in the diet.
In summary, in contrast to the strong recommendation of many medical societies, the majority of U.S. obstetricians and midwives who responded to this survey do not recommend iodine-containing vitamins in women planning pregnancy, during pregnancy, and during lactation. In spite of the poor response rate, the findings highlight a lack of knowledge about iodine supplementation by U.S. obstetricians and midwives. and suggest that nutrition education of both groups may be useful to protect at-risk women and their offspring.
Footnotes
Acknowledgments
The work was supported by National Italian American Foundation and Fondazione Bracco. This work was previously presented at the Endocrine Society Annual Meeting (April 1–4, 2016; Boston, MA) as a poster abstract and won the Presidential Poster Competition.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.