
Abstract
Background:
Atypia/follicular lesion of unknown significance (AUS/FLUS) has variable rates of malignancy. The recommended management includes active surveillance (AS), repeated fine-needle aspiration (RFNA), diagnostic surgery, or genetic testing for malignancy. The objective of this study was to assess the management of AUS/FLUS patients in a dedicated thyroid clinic without implementing genetic testing.
Methods:
This was a single institute cohort study of all patients aged ≥18 years who underwent ultrasound-guided FNA thyroid biopsies between January 2009 and January 2013 and were followed until January 2016. The median follow-up time was 4.6 years (range 3.2–6.8 years). Forty-eight (57%) patients were referred to AS, and 36 (43%) patients were referred for diagnostic surgery. Thirty-six (75%) patients from the AS group underwent RFNA. An additional eight patients from the AS group subsequently underwent diagnostic surgery.
Results:
Malignancies were found in 15/44 (34%) diagnostic surgical samples, and benign cytologies were found in 61.1% of the RFNAs. Analysis of adherence to follow-up in the 36 AS patients showed an adherence rate of only 53%, with males tending to comply better than females did (31.6% vs. 5.8%, respectively; p = 0.052), especially males in their sixth decade of life.
Conclusions:
Genetic tests for AUS/FLUS patients are accepted today as complementary evaluations in many well-developed health systems. Yet, when these tests are not feasible due to financial or availability issues, careful management of AUS/FLUS patients may still offer good results in the selection of patients for surgery or AS. The present results also indicate that compliance to follow-up schedules is a major consideration when selecting patients for AS.
Introduction
S
The malignancy rate of the AUS/FLUS category was estimated to be 5–15% overall according to the BSRTC consensus study (1). A recent meta-analysis reported an actual malignancy rate of 14%, ranging widely between reports (i.e., 6–48%) (4). This low albeit substantial malignancy rate poses considerable challenges in selecting the appropriate therapeutic management of AUS/FLUS patients.
Several factors have been extensively researched in an attempt to reduce diagnostic surgical procedures. Along with patient preferences, the factors that are used to stratify the malignancy risk in AUS/FLUS are outlined below.
Ultrasound features
Solid component, hypoechogenicity, microlobulated or irregular margins, microcalcifications, and taller-than-wide shapes are considered features associated with malignancy (2,5).
RFNA
Some reports have shown that RFNA reduces initial diagnosis of AUS/FLUS cytology in up to 60% of cases (6), while others have concluded that its clinical utility is limited (7).
Genetic testing
In many institutions, molecular analyses have become the preferred method to evaluate such lesions, given that several studies have shown relatively good predictive values (8 –11). However, genetic tests are expensive (12), and, more importantly, their predictive value depends upon the specific malignancy rate of indeterminate nodules within each institution. There are currently a number of genetic tests available for AUS/FLUS nodules based on different methodologies (13). In 2012, Alexander et al. published the results of the Afirma gene expression classifier (GEC; Veracyte, Inc., South San Francisco, CA). The test is based on microarray technology and analyzes the mRNA expression of 167 different genes. The authors found that the negative predictive value (NPV) for the AUS/FLUS category (n = 129) was 95%, meaning that a benign result carries a 5% risk for being malignant (8). In contrast, the positive predictive value (PPV) for the AUS/FLUS category was low (38%). In 2015, Labourier et al. (9) published their results of a combination of the miRInform Thyroid test (for known point mutations and fusion transcripts) and a 10-microRNA GEC. The NPV and PPV for AUS/FLUS nodules were 97% and 68%, respectively. Based on that publication, a modification of these tests combined together is now commercially available as the ThyGenX thyroid test and the ThyraMIR test (both by Interpace Diagnostics, Parsippany, NJ) (13). Nikiforov et al. (10) reported that the ThyroSeq v2.1 panel showed a NPV of 97.2% (range 92–99%) and a PPV of 77% (range 42–91%) for AUS/FLUS nodules. The strength of this study is that it demonstrates a high NPV for a wide range (5–45%) of pretest malignancy probabilities from different institutions and populations. The RosettaGX Reveal test (Rosetta Genomics Ltd., Rehovot, Israel), a new genetic test based on 24 selected microRNAs, has shown a 100% NPV for indeterminate nodules (AUS/FLUS and follicular neoplasm) whose final pathologies were validated by three pathologists (11). When interpreting statistical results of cytologic genetic studies, it is important to understand the influence of the pretest probability, which is based on the real malignancy incidence in a specific population and differs between health centers (e.g., academic, private, or tertiary care institutions).
Specific cytologic features
Major cytologic features associated with malignancy accepted by the Synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference (14) include: (i) an enlarged, oval, and irregular nucleus; (ii) eccentric and often multiple micronucleoli; (iii) fine, pale chromatin; (iv) longitudinal nuclear grooves; and (v) intranuclear pseudo-inclusions. The presence of such features has been shown to be associated with malignancy. Several reports stressed the importance of each specific feature (15 –18). Mathur et al. suggested that AUS/FLUS with nuclear atypia should be regarded as suspicious for PTC (SPTC) (16). Wu et al. proposed that AUS/FLUS should be subdivided into high and low risk: AUS/FLUS aspirates in which PTC or follicular neoplasm could not be excluded should be categorized as high-risk, and they may warrant a thyroidectomy or lobectomy, while conservative follow-up with RFNA or molecular testing is an adequate management option for patients with low-risk lesions (e.g., artifacts or scant material) (17).
The aim of this study is to present a management algorithm and outcomes of AUS/FLUS patients at the authors' institution for over a six-year period. To the best of the authors' knowledge, no study has investigated the role and efficacy of AS in this group of patients, including the importance of adherence to follow-up.
Patients and Methods
After obtaining Institutional Review Board approval, a prospective study was performed of all patients aged ≥18 years who underwent ultrasound-guided FNA (USGFNA) thyroid biopsies between January 2009 and January 2013 and who were followed until January 2016. All thyroid biopsies and US were performed by the same high-volume head and neck surgeon (M.Y.) and in accordance with the ATA guidelines for USGFNAs of the thyroid (19). Exclusion criteria were the absence of pertinent data and patients whose thyroid assessment failed to reveal sonographic or clinical features that warranted FNA of the thyroid according to the ATA guidelines (19). All the study patients had AUS/FLUS upon cytology. Patients who underwent an USGFNA of the thyroid along with a concurrent cytopathologic evaluation of more than one nodule were categorized according to the nodule with the highest BSRTC class, and were excluded from the study if the result was suspicious for follicular neoplasm (SFN), SPTC, or PTC. The cytologic diagnostic criteria were based on The Bethesda System for Reporting Thyroid Cytopathology (BSRTC) (1). Cytologic features were defined based upon the Synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference (14). All medical records were reviewed, and data were extracted on selected demographics, including age, sex, history of any other malignancy, and risk factors for thyroid cancer (e.g., history of external beam radiation during childhood, previous exposure to ionizing radiation during childhood or adolescence, a history of any thyroid cancer syndrome, or a history of thyroid cancer in one or more first-degree relatives). In addition, data were retrieved on the size of the thyroid nodules, results of initial and RFNAs, descriptions of FNA cytologic features, initial and last outpatient clinic visit findings, total number of outpatient visits, and final histopathological diagnosis when relevant. The retrieved data also included information on the sonographic features of each lesion, including size, echogenicity, margins, microcalcifications, and shape. Malignant US features were defined as marked hypoechogenicity (decreased echogenicity compared to the surrounding strap muscle), microlobulated or irregular margins, microcalcifications (≤2 mm in diameter, tiny, punctuated hyperechoic foci), and lesions that were taller than wide in shape (being greater in the anteroposterior dimension than in the transverse dimension). The US exam was done with a high-resolution portable 8–12 MHz system (Sonosite, M-Turbo, with a 35 mm linear array transducer). All USGFNA biopsies were performed with an on-site evaluation of adequacy by a cytopathologist.
All study participants were either referred for diagnostic surgery or for active surveillance (AS group) that included periodic (three- to six-month intervals) clinical and cytologic surveillance. Adherence to follow-up was considered positive if the patient attended all scheduled visits as recommended in the preceding clinic visit. Patients were defined as lost to follow-up if the last data collection exceeded six months prior to the end of the study period (January 2016).
For subgroup analysis, a “combined benign” group was defined, which comprised of patients with benign RFNA cytology and patients grouped together with benign histology.
Statistical analyses were performed using IBM SPSS Statistics for Windows v21 (IBM Corp., Armonk, NY). Categorical variables were described using frequencies and percentages. Variables that were normally distributed were described by means and standard deviation (SD), and abnormally distributed variables by median and interquartile ranges. The association between non-categorical (continuous) variables, categorical variables, and non-parametric variables was calculated with Student's t-test, the chi-square test, and the Mann–Whitney test, respectively. A two-tailed p-value of <0.05 was considered significant.
Results
During the study period, 498 patients underwent USGFNA thyroid biopsies. The procedures were well tolerated by all patients, and there were no complications. Overall, 84 (16.8%) patients were found to have AUS/FLUS and comprised the study group. There were 27 (32%) males and 57 (68%) females, whose median age at the time of the FNA was 55.8 years (SD = 17.8 years; range 23–90 years). The malignancy rate of the whole study group was 17.8% (15/84), as shown in Table 1.
PTC, papillary thyroid carcinoma; FVPC, follicular variant papillary carcinoma; NOS, not otherwise specified.
Figure 1 presents a summary of management methods and outcomes of the study group. Forty-eight (57%) patients were referred to AS, and 36 (43%) patients were referred to diagnostic surgery, of whom 12 (33%) were found to have malignancies on final pathology. Thirty-six (75%) AS patients underwent RFNA, seven (14.5%) were lost to follow-up, one died of other causes, and four were followed in the outpatient clinic. An additional eight patients from the AS group eventually underwent diagnostic surgery. Malignancy was found in 15 (34%) of the 44 patients who underwent diagnostic operations.
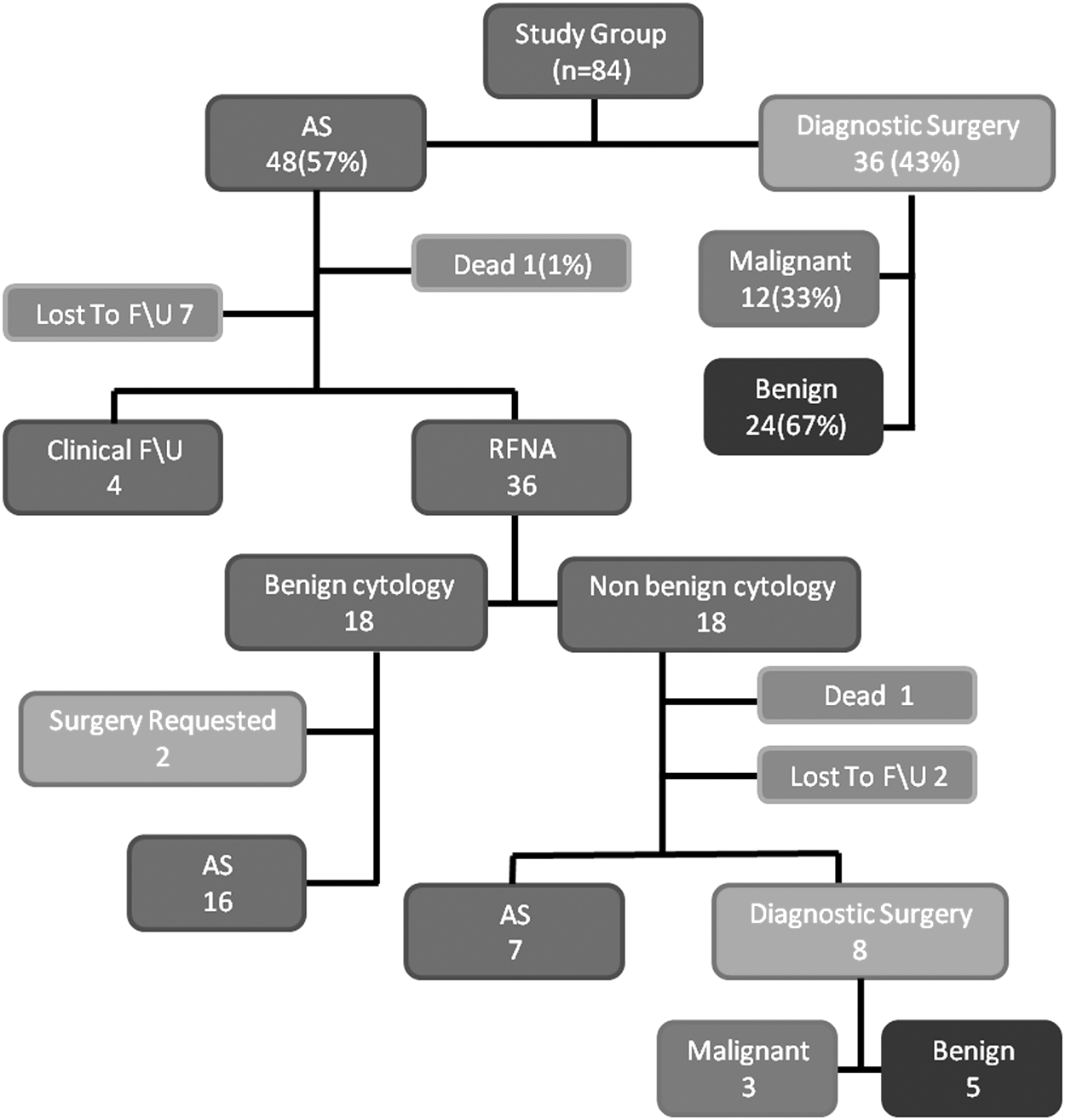
Outcome summary of the study group. In total, surgery was performed in 46 (54%) patients, 44 of them with diagnostic intent, of which 15 (15%) lesions were found to be malignant. Active surveillance (AS) was used in 27 (32%) patients. Eleven (13%) patients were lost to follow-up or deceased. F/U, follow-up; RFNA, repeated fine-needle aspiration.
Figure 2 summarizes the cytologic results of the 36 USGRFNAs. Eighteen of them were benign. Of the remaining 18 patients with RFNA, eight (44%) underwent diagnostic surgery, seven were clinically and sonographically followed, despite having non-benign cytology results (five of them underwent a third RFNA), two were lost to follow-up, and one patient died of other causes during the follow-up period. Overall, 22 patients had benign cytologies after RFNAs (18 after the first one and four after the second one; 61.1%).

Distribution of the RFNA cytology classification. BSRTC, Bethesda System for Reporting Thyroid Cytopathology; AUS/FLUS, atypia/follicular lesion of unknown significance; SFN, suspicious follicular neoplasm; SPTC, suspicious papillary carcinoma (1).
Next, the role of sonographic and cytologic features was examined in predicting malignancy in comparison to the combined benign subgroup (Table 2). Based on this analysis, the highest PPV and the highest NPV for malignancy were found for lesions with irregular margins (75% and 80%, respectively). The PPV and NPV for all other tested sonographic variables ranged between 5–30% and 76–80%, respectively. The PPV and NPV for the presence of major cytologic features associated with malignancy were 28% and 16%, respectively. None of these variables was found on univariate analysis to be a significant predictor for malignancy except for nodule size (Table 3; p < 0.05). Next, correlations of combinations between sonographic features and the presence of major cytologic features associated with malignancy were examined. Nodules with at least one major cytologic feature associated with malignancy and irregular margins or the presence of any three sonographic features associated with malignancy were significantly associated with malignancy (p = 0.01 and p = 0.009, respectively).
NPV, negative predictive value; PPV, positive predictive value.
Statistically significant values are shown in bold.
Combined benign: benign cytology + benign pathology grouped together.
AUS/FLUS, atypia/follicular lesion of unknown significance.
The median follow-up time of the patients was 4.6 years (range 3.2–6.8 years). The adherence to follow-up was analyzed in 36 patients from the AS group (as defined in the Methods section). The mean age of those patients was 56 years (range 23–90 years), and the median number of clinic visits was four (range 2–9). Only 53% (19/36) of the patients adhered to follow-up. Age was not significantly different between the groups. Males tended to be more compliant with follow-up compared to females (31.6% vs. 5.8%, respectively; p = 0.052). The highest rate of patient compliance with follow-up was in the sixth decade of life (7/9; 77%) followed by the third decade (2/3; 66%; Fig. 3). The rate of patients lost to follow-up was ≥50% among all the other age groups.
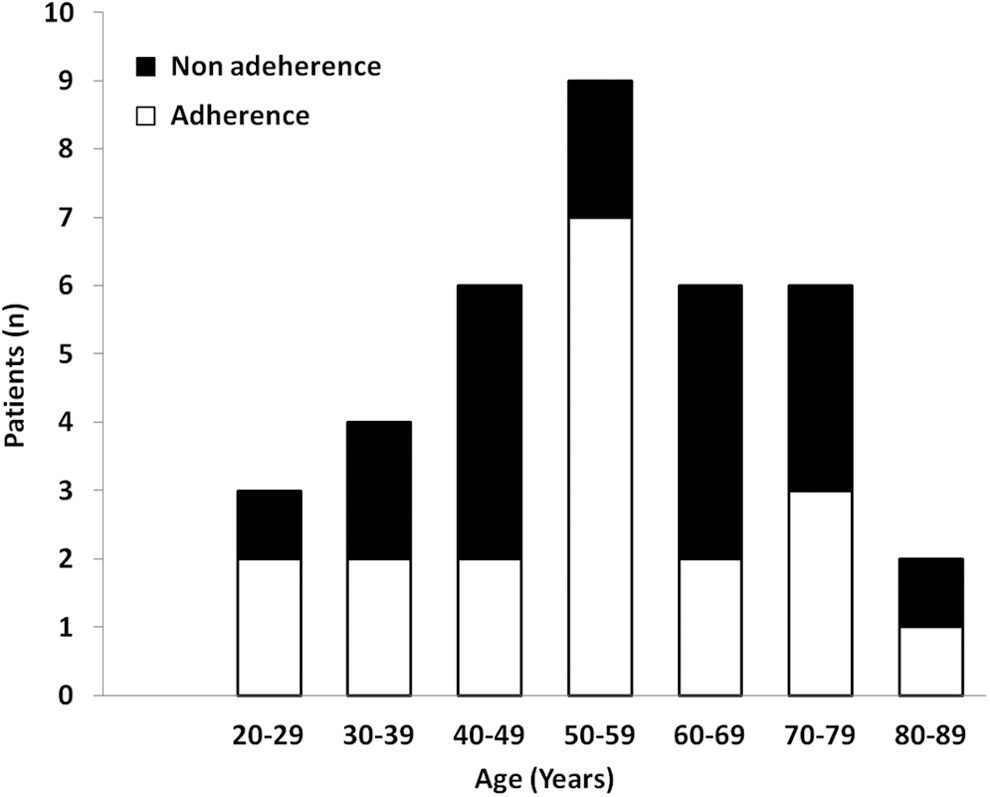
Adherence to follow-up according to age group.
Discussion
It is for good reason that the Bethesda category III—AUS/FLUS was defined as a last resort when presented in the Bethesda conference, given that it represents a broad spectrum of cytologic scenarios (1). Its heterogeneous character allows for multiple acceptable management approaches (i.e., conservative follow-up, RFNA, or surgery). The authors suggested that its use should be limited to no more than 7% of all FNAs performed. Yet, in practice, its prevalence ranges between 1% and 27% of all thyroid nodule cytologies (20,21).
This study reports the authors' experience with AUS/FLUS patients in their dedicated thyroid clinic. In addition to a “routine” physical examination, the visit includes a surgeon-performed US of the thyroid. When indicated, an USGFNA is also performed, together with an on-site cytopathology evaluation. The study results illustrate the authors' experience with patient selection for surgery, yield of RFNAs, and the correlation between each of them with final pathology. More importantly, to the best of the authors' knowledge, this is the first study to focus on the yield of conservative clinical follow-up in patients with AUS/FLUS cytology. The compliance of patients to maintain a scheduled follow-up, which includes repeat US and clinic visits every three to six months, was evaluated (2,19).
Multiple reports have measured the prevalence of malignancy in AUS/FLUS cytology, and there are significant differences between them. A 20–25% malignancy rate had originally been attributed to patient selection (22,23), which was supported by later reports (8). In 2013, Ho et al. reported their experience with 541 patients, among whom the malignancy rate was 26.6% (144/541) for all AUS/FLUS patients and 37.8% (144/381) for AUS/FLUS patients who were referred for surgery (24). Those rates were considered considerably higher than previously reported values. The authors suggested that a larger sample size and a selection bias by a referral center may account for the difference. They concluded that current guidelines of AUS/FLUS nodules should be reconsidered, since the malignancy rate is higher than previously thought. The present results show a similar malignancy rate among operated patients (15/44; 34%). Yet, the overall malignancy rate was 17.8% (15/84), similar to the findings initially reported at the Bethesda conference (1). The rate of malignancy was 23.4% (15/64) when the cytology result on RFNA was considered as being benign (25,26). Accounting for false-positive benign RFNAs (7), it is assumed that the true malignancy rate of AUS/FLUS in the authors' institution ranges from 23.4% to 34%. The present results suggest that careful patient selection can result in fewer diagnostic surgeries and an increase in the malignancy rate in the operated group.
This study demonstrates both a high rate of benign cytology on repeat FNA (61.1%) and a high rate of malignancy within the operated group (34%). These two trends may appear to be conflicting with regard to the appropriate management of AUS/FLUS patients. The high rate of benign RFNA advocates a more conservative approach, as suggested by previous studies (6,27 –29), while the high rate of malignancy calls for a higher index of suspicion, which would favor surgery, as suggested by Ho et al. (24).
Faquin et al. (6) conducted RFNAs in 40% of their AUS/FLUS patients (203/509), and the RFNA results were benign in 60% of those patients. Other reports found a range of 42–63.5% for benign results on RFNA for AUS/FLUS patients (27 –29), consistent with the present findings. These studies concluded that RFNA is a reliable tool for better patient selection for surgery. In contrast, VanderLaan et al. (7) found that malignancy following a benign RFNA can reach 28% (2/7 patients). They suggested that RFNA for AUS/FLUS should be limited to cases not suggestive of papillary carcinoma, such as artifacts or sparse cellularity, and that surgery rather than RFNA may be a more appropriate course for many patients. Nevertheless, considering its yield and availability, it is recommended that most patients be referred for RFNA.
Suspicious sonographic features have been shown to predict malignancy in 60–100% of nodules with AUS/FLUS cytology, while Khoncarly et al. (30) and Ho et al. (24) reported lower values. The existence of even only one suspicious US feature significantly increased the risk of malignancy in AUS/FLUS nodules (2,7).
The present results show that the combination of one major cytologic feature together with irregular margins or in the presence of three malignancy-associated sonographic features correlates with malignant histological results. These results are consistent with the TIRADS grading of nodules by US features suggested by Kwak et al. (5) and other reports (31). Since the inter-observer variability for all malignancy-associated features was found to be considerable for most sonographic features (32), the use of a single operator when feasible is encouraged (M.Y. in this study). This is especially relevant, since US features were shown to contribute to patient selection for surgery. Therefore, a consistent and reliable characterization of the nodule is critical.
In recent years, several publications suggested that AUS/FLUS should be subdivided based on the cytologic description. Smears showing major cytologic features suggestive of malignancy may have a higher incidence of malignancy, reaching 75% (15 –18), while smears devoid of such features have a greatly reduced risk (18%) of malignancy (16). Mathour et al. suggested that AUS with rare PTC features should just be called suspicious for PTC (16). These suggestions were not directly addressed in the recently revised ATA guidelines (2). The present study does not have sufficient power to discern significant differences between patients with benign versus malignant histologies based on the presence of atypical cytologic features. Moreover, the high inter-observer variability, which has been reported in this category (33), results in different prevalence rates of AUS/FLUS specimens in different institutions. Mathur et al. (16) sent 806 AUS/FLUS to a different cytologist for a second cytologic evaluation and found an agreement rate of only 57%. Furthermore, when atypia was reported by both cytologists, the malignancy rate was 68%, suggesting that an independent review of all AUS cases may contribute to better patient selection.
Since each of the tools used for risk stratification has limitations (e.g., clinical, sonographic, and cytologic inter-observer variability), the importance of a dedicated team approach and communication with an experienced cytopathologist, as well as familiarity of the team with their own institution's data, cannot be overemphasized.
This study shows that a combination of suggestive findings in both modalities was significantly associated with malignancy. This, in turn, reflects the challenge of AUS/FLUS patient selection for surgery. When referring a patient for surgery, it is up to the attending physician to look at the nodule in a comprehensive manner and to integrate the patient's history, the US features, the cytologic description, and the patient's ability to maintain active follow-up. It is recommended that nodules with major cytologic features associated with malignancy and irregular borders or three other known malignancy-associated sonographic features should be referred for surgery.
In its consensus statement, the Bethesda task force suggested that certain AUS/FLUS patients could be managed by clinical follow-up alone, which includes yearly US and clinic visits (1). In its recommendation for management of AUS/FLUS cytology, the ATA considered surveillance to be an adequate option, considering informed patient preference and feasibility (2). To the best of the authors' knowledge, this study is the first to assess the applicability and feasibility of this option in the management of AUS/FLUS patients. A significant result of this study is the low rate of adherence to follow-up. Nearly half of the patients did not adhere to follow-up. In an attempt to characterize which patients are at risk of being lost to follow-up, it was found that males were more compliant than females were. The most concerning result was a median of only three visits among patients who did not comply with follow-up visit recommendations. Specifically, despite them being aware of the risk of malignancy, a large number of patients kept only one appointment beyond the one during which they were diagnosed with AUS/FLUS. Since the authors' database includes both hospital and community visits, it is reasonable to assume that these patients did not maintain any follow-up during the study period after being diagnosed with AUS/FLUS. It is possible that some of these patients chose to maintain follow-up by other healthcare providers that accept private insurance. However, this is unlikely, as there were no such visits documented in their attending family physician's follow-up notes (which would be expected if they underwent surgery elsewhere). Moreover, all of the non-compliant AS patients were contacted by the first author and asked to resume follow-up. Some of the patients refused to do so, while others did not maintain AS requirements following their visit (i.e., did not undergo US studies as requested or did not attend their next scheduled visit). Therefore, AS should be considered as a feasible management option only when both the patient and the caregiver are committed to its requirements. Adherence to follow-up may also be influenced by cultural, educational, and socioeconomic factors.
One possible explanation for the low rate of adherence is the relatively short interval between appointments (3–6 months). This interval was chosen by the authors, since it was unclear whether AS can be considered as a reasonable management option. The follow-up visits are currently scheduled every 6–12 months, depending upon different known risk factors. These longer time intervals should not affect the clinical outcomes and will hopefully enhance compliance. The optimal interval for clinical follow-up in AUS/FLUS patients that results in best compliance and clinical outcomes should be evaluated in future prospective studies.
The present results should be considered by all physicians caring for patients with indeterminate thyroid cytology. It is critical for the physician to keep track of these patients, and he/she should emphasize that other than surgery, all other management options rely on the ability of the treatment team to reassess the nodule's malignancy potential at each visit. That being said, recent advances in thyroid genetic testing may lead to alternative methods for selecting active surveillance or surgery in these patients.
Genetic tests currently complement other sources of information or clinical judgment (2). As stated in the ATA guidelines, the variability of the pretest probability (which, in turn, affects the predictive value of the tests) can negatively impact the value of genetic testing (2,34). Additionally, although genetic testing still lacks long-term follow-up data, recent reports on genetic tests have shown promising results, with excellent predictive values in patients with AUS/FLUS cytology. The clinician should be familiar with their applications with respect to both the patient's and the clinician's health system environment.
This study presents a six-year follow-up of patients with AUS/FLUS cytology. None of the patients selected for AS were diagnosed with thyroid cancer during the study period. This fact by itself supports the recommendation presented in the Bethesda conference, in which AS is an acceptable and safe possibility in selected patients. In addition, careful patient selection may reduce unnecessary diagnostic surgeries and significantly increase the rate of detecting malignancies in patients undergoing surgery for AUS/FLUS lesions. Patients should be meticulously selected for AS, with a concerted effort to assess their ability to maintain follow-up (patient factor), together with assessing the malignant potential of the nodule (nodule characteristics factor).
In conclusion, AUS/FLUS patients continue to pose a clinical challenge. While RFNA is a reliable and important tool in the management of these patients, active surveillance should be offered after careful assessment of the patient and the nodule's characteristics. When applicable, genetic testing should be considered in AUS/FLUS patients, particularly when the diagnosis is confirmed by RFNA or, alternatively, when compliance to follow-up is expected to be poor.
Footnotes
Acknowledgments
We thank Prof. Dan M. Fliss from the Department of Otolaryngology—Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Israel, for assistance with revising the final draft and for comments that greatly improved the manuscript. The paper was presented at the annual Israeli Society of Head and Neck Surgery conference Ramot, Israel, November 2015.
Author Disclosure Statement
No competing financial interests exist.