
Abstract
Background:
In preparation for 131I ablation, temporary withdrawal of thyroid hormone is commonly used in patients with thyroid cancer after total thyroidectomy. The current study aimed to investigate brain glucose metabolism and its relationships with mood or cognitive function in these patients using 18F-fluoro-2-deoxyglucose positron emission tomography (18F-FDG-PET).
Method:
A total of 40 consecutive adult patients with thyroid carcinoma who had undergone total thyroidectomy were recruited for this cross-sectional study. At the time of assessment, 20 patients were hypothyroid after two weeks of thyroid hormone withdrawal, while 20 received thyroid hormone replacement therapy and were euthyroid. All participants underwent brain 18F-FDG-PET scans and completed mood questionnaires and cognitive tests. Multivariate spatial covariance analysis and univariate voxel-wise analysis were applied for the image data.
Results:
The hypothyroid patients were more anxious and depressed than the euthyroid participants. The multivariate covariance analysis showed increases in glucose metabolism primarily in the bilateral insula and surrounding areas and concomitant decreases in the parieto-occipital regions in the hypothyroid group. The level of thyrotropin was positively associated with the individual expression of the covariance pattern. The decreased 18F-FDG uptake in the right cuneus cluster from the univariate analysis was correlated with the increased thyrotropin level and greater depressive symptoms in the hypothyroid group.
Conclusions:
These results suggest that temporary hypothyroidism, even for a short period, may induce impairment in glucose metabolism and related affective symptoms.
Introduction
I
As a treatment strategy for thyroid cancer, 131I ablation following total or near-total thyroidectomy is recommended for most patients (3). For successful 131I ablation, patients are required to stop levothyroxine therapy for at least three weeks prior to 131I ablation in order to elevate thyrotropin (TSH) levels. Recombinant human TSH provides an alternative for the preparation of 131I therapy and allows patients to maintain levothyroxine therapy, thereby avoiding hypothyroidism (4). However, its use for remnant ablation and therapy ablation is limited based on the activity of radioactive iodine in South Korea. The cost for recombinant human thyrotropin is reimbursed by national health insurance only when using 131I ≤ 100 mCi. Consequently, a substantial number of thyroid cancer patients undergo thyroid hormone withdrawal after total thyroidectomy and often suffer from various hypothyroid-related symptoms that can impair quality of life, such as depression, anxiety, and cognitive impairment (5 –8).
Thyroid hormones are of high importance for normal brain function. Multiple neurotransmitter systems, including catecholaminergic and serotonergic systems, are affected by the excess or deficit of thyroid hormones (9). Nevertheless, only a few in vivo neuroimaging studies have examined hypothyroid patients following total thyroidectomy. Previous single photon emission computed tomography (SPECT) studies found decreased regional cerebral blood flow (rCBF) primarily in the occipital lobe (6,7,10). In a study using 18F-fluoro-2-deoxyglucose positron emission tomography (18F-FDG-PET), only a global reduction in regional cerebral metabolic rate of glucose (rCMRglu) was found without regional effects (6). Furthermore, associations between altered rCBF or rCMRglu and clinical symptoms have not yet been demonstrated (6,7,10).
The current study aimed to investigate brain glucose metabolism and its relationships with cognitive or psychiatric symptoms in hypothyroid patients after total thyroidectomy for thyroid cancer. Two complementary approaches were combined for analyses of 18F-FDG-PET images: multivariate spatial covariance analysis and univariate voxel-wise analysis. The former is based on the scaled subprofile model, an extension of principal component analysis, and has the advantage of identifying neural networks with greater statistical power by simultaneously taking into account signals from multiple areas (11). On the other hand, the latter allows better localization and interpretation of significant areas of difference. In addition, euthyroid patients who were on levothyroxine therapy after total thyroidectomy were chosen as a comparison group rather than healthy volunteers in order to exclude effects of potential confounding factors such as low-iodine diet and cancer-related stress.
Materials and Methods
Participants
Adult patients with thyroid carcinoma who underwent total thyroidectomy were prospectively recruited at Incheon St. Mary's Hospital (Incheon, South Korea) from June 2014 to December 2014. Participants were excluded if they had any other neurological or psychiatric disorders, or if they were taking any psychotropic medication. Based on the clinical risk stratification for thyroid cancer, the clinician and nuclear medicine physician determined the treatment strategy. All patients received levothyroxine for approximately four to five months following total thyroidectomy. After discontinuing levothyroxine therapy, the high-risk patients were given triiodothyronine (T3) for two weeks followed by complete withdrawal of thyroid hormones for three weeks before ablation with 150 mCi of 131I (withdrawal group). Meanwhile, the low-risk patients continued to take levothyroxine until ablation. They received two intramuscular injections of recombinant human thyrotropin two days and one day before ablation with 100 mCi of 131I (replacement group). Considering the higher iodine intake in South Korea compared with other countries (12), both groups were kept on a low-iodine diet for three weeks prior to 131I ablation. All clinical assessments and 18F-FDG-PET scans were performed one week before 131I ablation. Therefore, the patients in the withdrawal group were hypothyroid for two weeks at the time of evaluation. The timeline of the study is outlined in Figure 1. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board at Incheon St. Mary's Hospital. Written informed consent was obtained from all participants.
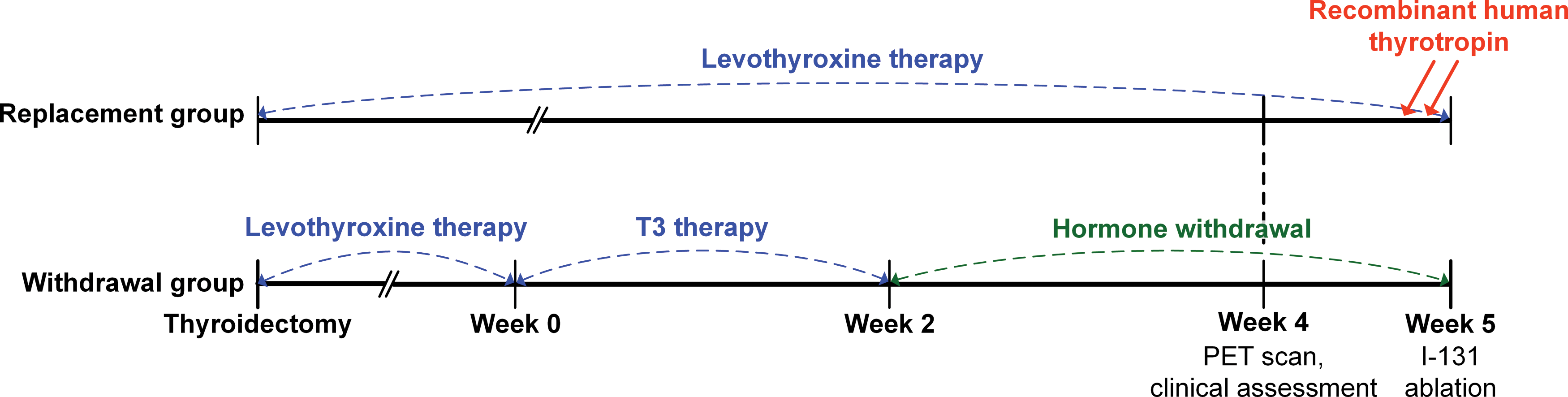
Study timeline. All patients received levothyroxine following total thyroidectomy. After discontinuing the levothyroxine therapy, the high-risk patients were given triiodothyronine for two weeks followed by complete withdrawal of thyroid hormones for three weeks before 131I ablation (withdrawal group). Meanwhile, the low-risk patients continued to take levothyroxine until ablation (replacement group). All assessments were performed at one week before 131I ablation. Color images available online at
Clinical assessment
Serum levels of T3, free thyroxine (fT4), and TSH were measured in blood samples. Global cognitive status was evaluated with the Montreal Cognitive Assessment (MoCA) test (13,14) by a licensed neuropsychologist who was blinded to the study protocol. The total score ranges from 0 to 30, with a higher score reflecting better performance. The Center for Epidemiological Studies Depression Scale (CES-D) (15,16) and Beck Anxiety Inventory (BAI) (17,18) were administered to assess depressive and anxiety symptoms, respectively. The total scores of the CES-D and BAI ranged from 0 to 60 and 0 to 63, respectively, with higher scores indicating more symptoms.
Image acquisition and processing
All participants fasted for 6 h, and blood glucose level was measured to ensure that it did not exceed 130 mg/dL. Approximately 45 min after intravenous injection of 18F-FDG (185–222 MBq), PET images were acquired under standard resting conditions using a Discovery STE PET/CT scanner (GE Healthcare, Milwaukee, WI). The scanner allows simultaneous imaging of 47 transaxial slices in three-dimensional mode (pixel size = 1.95 mm × 1.95 mm, with a slice thickness of 3.27 mm). Sixteen-slice CT scans were also performed for attenuation correction.
Statistical Parametric Mapping 8 (SPM8; Wellcome Department of Cognitive Neurology, Institute of Neurology, London, United Kingdom) was used for image processing. The PET images were spatially normalized to the SPM PET template (Montreal Neurological Institute, McGill University, Montreal, Canada), resliced with a voxel size of 2 mm × 2 mm × 2 mm, and smoothed with an 8 mm full-width half-maximum isotropic Gaussian kernel.
Multivariate spatial covariance analysis
Multivariate spatial covariance analysis was conducted for all processed PET images using the Generalized Covariance Analysis program v1.2 (
A linear regression model with each individual's SSF as an independent variable and group as a dependent variable was used to identify a spatial covariance pattern that best discriminates the two groups. The set of eigenimages that yielded the lowest Akaike's information criterion value was selected (20) and linearly combined to produce the spatial covariance pattern and its SSF value. The SSF values in the withdrawal group were standardized (z-scored) with respect to those in the replacement group such that the mean for the replacement group was 0 and the standard deviation was 1. Nonparametric regression with 10,000 permutations was used to test the hypothesis of the significant relationship between the spatial covariance pattern and group membership. To identify areas that significantly contributed to the pattern, stability, and reliability of the voxel loadings from the pattern were assessed with a bootstrap resampling method using 1000 iterations. This procedure converted the voxel loadings into z-values. A threshold of |z| > 1.64 (one-tailed p < 0.05) was adopted for visualization.
Univariate voxel-wise analysis
A voxel-wise two-sample t-test for the PET data was performed in SPM8 after introducing age and sex as covariates. Global counts were normalized using proportional scaling to a mean value of 50 mL/dL/min. A relative threshold masking of 0.8 was applied. The statistical threshold was set at a family-wise error (FWE) corrected p < 0.05 at both voxel and cluster levels. The normalized mean rCMRglu value was extracted from the most significant cluster using MarsBaR toolbox v0.44 (
Statistical analysis
Differences in demographic and clinical variables between the two groups were examined with an independent t-test and a chi-square test.
Relationships between the TSH level and standardized SSF value from the spatial covariance pattern and between the TSH level and normalized mean rCMRglu from the most significant cluster were examined in both groups, since TSH is potentially considered as the best serum biomarker of thyroid hormone availability and severity of hypothyroidism. Multiple linear regressions were used with the SSF value or rCMRglu as a dependent variable and the TSH level as an independent variable, while adjusting for age and sex.
Correlations between the SSF value or rCMRglu and the cognitive or psychiatric variables that had shown significant group differences were further assessed. Multiple linear regressions were conducted with the scores of the MoCA, CES-D, or BAI as a dependent variable and the SSF value or rCMRglu as an independent variable, while adjusting for age and sex.
An alpha value of <0.05 (two-tailed) was considered significant. All statistical analyses were condected with Stata v13.1 (StataCorp, College Station, TX).
Results
A total of 40 patients with thyroid carcinoma participated in the study. Among them, 20 high-risk patients were assigned to the withdrawal group, while the rest were allocated to the replacement group. Demographic and clinical characteristics of the participants are presented in Table 1. There was a significant difference in the sex ratio between the two groups (χ2 = 4.80, p = 0.01), with more women in the replacement group. The two groups did not significantly differ in terms of age (p = 0.38) or the MoCA total score (p = 0.16). However, the CES-D scores (t = 2.63, p = 0.01) and BAI scores (t = 2.47, p = 0.02) were higher in the withdrawal group. All patients in the replacement group were clinically euthyroid, while those in the withdrawal group met the criteria for clinical hypothyroidism. T3 levels (t = –17.86, p < 0.001) and fT4 levels (t = –37.07, p < 0.001) were lower, whereas the TSH level was higher in the withdrawal group (t = 11.38, p < 0.001). No patients were excluded from the analyses due to brain metastases detected by brain 18F-FDG-PET/CT.
Independent t-test for continuous variables and chi-square test for sex.
MoCA, Montreal Cognitive Assessment; CES-D, Center for Epidemiological Studies Depression Scale; BAI, Beck Anxiety Inventory; T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin.
In the spatial covariance analysis, the linear combination of four principal components significantly distinguished the two groups (R 2 = 0.49, p = 0.009). The identified spatial covariance pattern is shown in Figure 2. Positive loadings were mainly observed in the bilateral insula and surrounding areas, including the frontal orbital cortex, putamen, parahippocampal gyrus, brainstem, and cerebellum. Negative loadings were found in bilateral parieto-occipital regions, including the superior/inferior parietal lobule, precuneus, cuneus, lingual gyrus, and middle/inferior occipital gyrus. The SSF score was significantly higher in the withdrawal group than it was in the replacement group (t = 6.01, p < 0.001). Additionally, a positive association between the TSH level and SSF value was found in the withdrawal group (β = 0.45, p = 0.015). However, the SSF score was related to neither CES-D nor BAI score in the withdrawal group (p > 0.05). In the replacement group, individual SSF value was not correlated with TSH, CES-D, or BAI (p > 0.05).
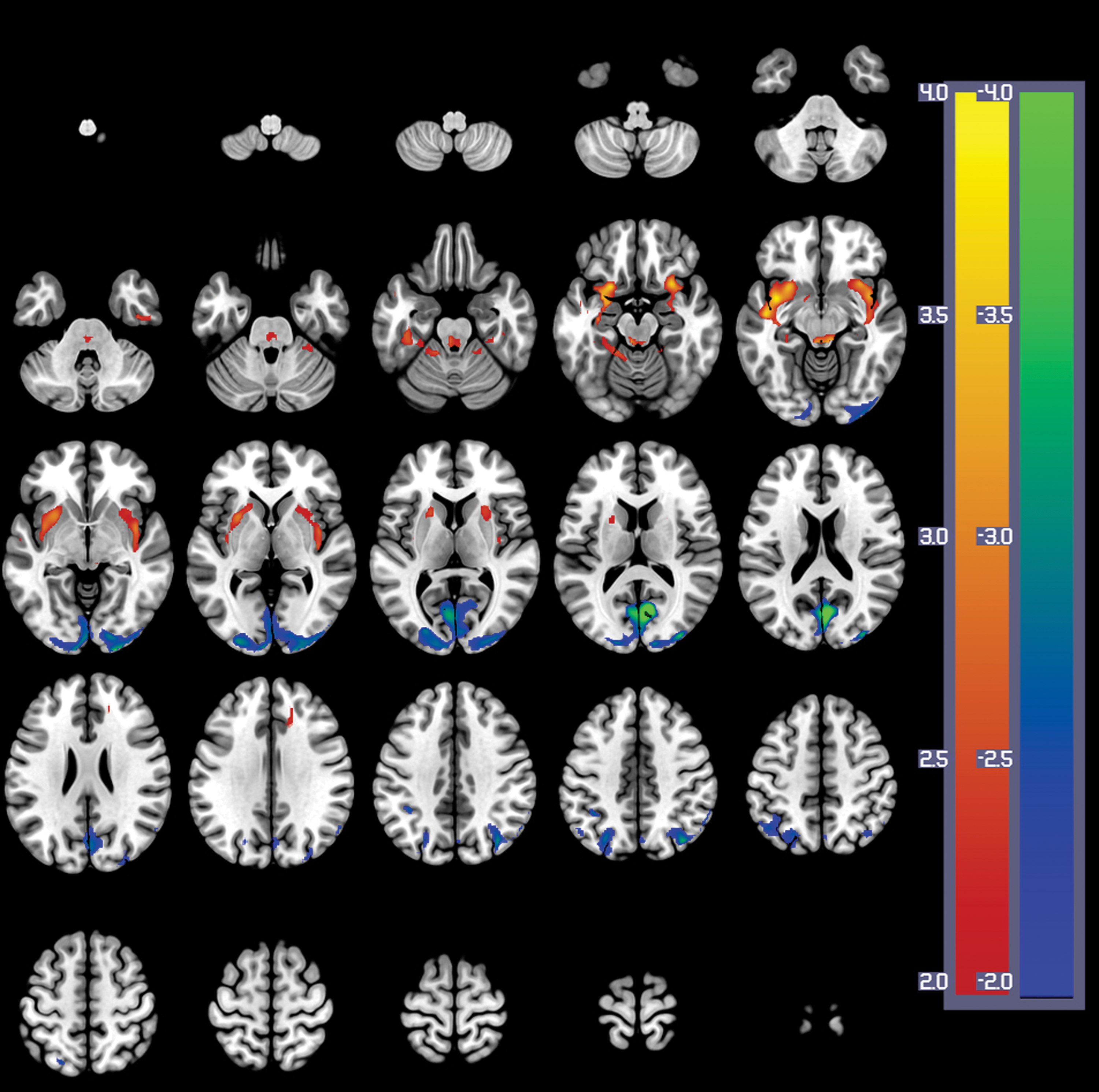
Spatial covariance pattern of regional cerebral metabolic rate of glucose, distinguishing the withdrawal group from the replacement group. At each voxel, positive and negative loadings appear in red-yellow and blue-green, respectively. Images are shown in neurological convention. The color bar represents a z-value for each voxel. A threshold of |z| > 1.64 (one-tailed p < 0.05) was adopted for visualization. Color images available online at
The results from univariate voxel-wise analysis are summarized in Table 2 and Figure 3. The withdrawal group demonstrated lower 18F-FDG uptake in the right cuneus (voxel level FWE-corrected p = 0.001, cluster size = 1600 mm3) and right inferior occipital gyrus (voxel level FWE-corrected p = 0.002, cluster size = 664 mm3) when compared with the replacement group. However, the withdrawal group did not show any hypermetabolic areas.
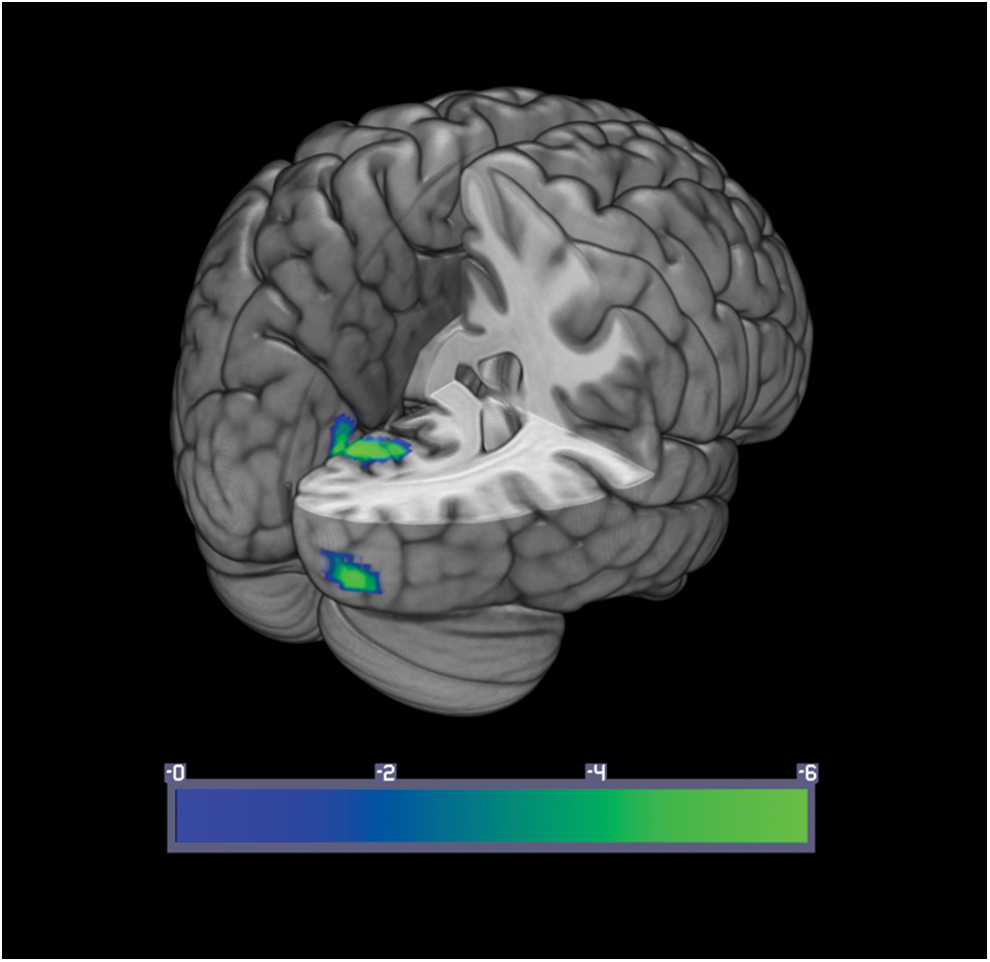
Hypometabolic areas in the withdrawal group compared with the replacement group. The statistical threshold was set at a family-wise error corrected p < 0.05 at both voxel and cluster levels. Images are shown in neurological convention. The color bar represents the t-value for each voxel. Color images available online at
Statistical threshold was set at a family-wise error (FWE) corrected p < 0.05 at both voxel and cluster levels.
The coordinates refer to the Montreal Neurological Institute coordinate system.
In the withdrawal group, the rCMRglu in the right cuneus cluster was inversely associated with the TSH level (β = –0.68, p < 0.001) and the CES-D score (β = –0.70, p = 0.005), but not with the BAI score (p = 0.94). Glucose metabolism in the right inferior occipital gyrus did not correlate with the TSH, CES-D, or BAI (p > 0.05). In the replacement group, the rCMRglu values in both clusters were not significantly related to the TSH, CES-D, or BAI (p > 0.05).
Discussion
In preparation for 131I ablation, temporary withdrawal of thyroid hormone is commonly used in patients with thyroid cancer after total thyroidectomy. However, effects of hypothyroid condition on brain glucose metabolism and their relationships with mood or cognition remain unclear.
The current study examined thyroid cancer patients after total thyroidectomy in order to investigate brain glucose metabolism and its relationships with mood or cognitive function using two complementary analyses of 18F-FDG-PET data. The hypothyroid patients were more anxious and depressed than the euthyroid patients were, although the difference in cognitive function was not significant. The spatial covariance analysis showed increases in rCMRglu in the bilateral insula and surrounding areas, and concomitant decreases in the parieto-occipital regions in the hypothyroid group. The TSH level was positively associated with expression of the covariance pattern. The decreased 18F-FDG uptake in the right cuneus cluster from the univariate analysis was correlated with increased TSH levels and greater depressive symptoms in the hypothyroid group.
It has been well documented that not only permanent thyroid dysfunction, but also transient hypothyroidism of short duration before 131I ablation therapy can cause anxiety and depressive symptoms and cognitive decline (5 –7,21). In line with previous evidence, the scores of both the CES-D and the BAI were higher in the withdrawal group after two weeks of T3 withdrawal. However, the MoCA total score was not statistically different between the two groups. This inconsistency may be due to the short duration of thyroid hormone withdrawal compared with three to five weeks in previous studies (5 –7). Additionally, the MoCA was originally developed as a brief screening instrument for mild cognitive impairment (13), and therefore it might be less sensitive to detect subtle cognitive decline in short-term hypothyroid patients. More comprehensive neuropsychological test batteries would be desirable in future studies.
The spatial covariance analysis demonstrated that the 18F-FDG uptake increased most significantly in the bilateral insula. This result is supported by the SPECT study that showed augmented rCBF in the insula during transient hypothyroidism after 131I treatment (7). The insula is one of the key areas of autonomic regulation, including control of the cardiovascular system (22). Moreover, a previous animal study reported the influences of hypothyroidism on arterial baroreflex function and autonomic contributions to heart rate and resting blood pressure (23). Further human studies are warranted to evaluate hypothyroidism-related alterations in the cardiovascular autonomic function and their relationships with the insula. On the other hand, the decreased pattern of glucose metabolism in parieto-occipital areas was consistent with most previous neuroimaging studies performed on hypothyroid patients, which reported reductions of rCMRglu (6) and rCBF (7,10,24) in these regions. It is noteworthy that both the multivariate and univariate analysis identified the cuneus as the area with the most remarkable decrease in rCMRglu.
In the regression analyses in the withdrawal group, the TSH level was positively correlated with the individual expression of the covariance pattern and negatively associated with rCMRglu in the cuneus cluster. These results suggest the direct relationships between the severity of hypothyroidism and changes in brain glucose metabolism. Furthermore, although the individual SSF scores, which captured the global pattern of glucose metabolism, were not related to specific symptoms, the larger reduction of 18F-FDG uptake in the cuneus cluster were associated with greater depressive symptoms in the withdrawal group. Interestingly, rCBF in the parieto-occipital area including the cuneus was lower in hypothyroid patients compared with patients with major depression (25). Additionally, a previous study on euthyroid patients with mood disorders demonstrated that the level of TSH is inversely related to the rCMRglu in the cuneus (26). These results may also suggest different neural circuitries mediating affective symptoms in hypothyroidism and major depression. It would be of clinical and scientific significance to investigate the exact roles of the cuneus and surrounding areas in hypothyroidism-related depression.
Some potential limitations should be addressed. First, the different sex ratio between the two groups might introduce some bias into the results, although sex was included as a covariate of no interest in all analyses. Caution is needed in interpretation of these findings. Second, the cross-sectional nature of the study design precluded inferences about causal relationships among variables, despite the results of the regression analyses.
In summary, the present study indicates that the brain metabolic covariance pattern can be altered in hypothyroid patients after thyroidectomy for thyroid cancer. Moreover, reduction of glucose metabolism in the cuneus may be specifically related to depressive symptoms in these patients. These results suggest that temporary hypothyroidism, even of short duration, may induce impairment in glucose metabolism and related affective symptoms. Further prospective studies are needed to examine the effects of duration of hypothyroidism and thyroid hormone therapy on brain structure, function, and metabolism.
Footnotes
Acknowledgments
The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2014. This study was also supported by the Global Frontier R&D Program on “Human-centered Interaction for Coexistence” of the National Research Foundation of Korea funded by the Korean Government (MSIP; 2012M3A6A3055707). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
The authors declare that there is no conflict of interest.