
Abstract
Background:
The aim of this study was to investigate the national prevalence of thyroid dysfunction in Spain and its association with various clinical, environmental, and demographic variables.
Methods:
The study included 4554 subjects (42.4% men) with a mean age of 50 years (range 18–93 years), who were participants in a national, cross-sectional, population-based survey conducted in 2009–2010. Data gathered included clinical and demographic characteristics, physical examination, and blood sampling. Thyrotropin, free thyroxine, free triiodothyronine, and thyroid peroxidase antibody (TPOAb) concentrations were analyzed by electrochemiluminescence. Urinary iodine (UI) levels were measured in an isolated urine sample.
Results:
The prevalence of treated hypothyroidism, untreated subclinical hypothyroidism, and untreated clinical hypothyroidism was 4.2% [confidence interval (CI) 3.6–4.9%], 4.6% [CI 4.0–5.2%], and 0.3% [CI 0.1–0.5%], respectively. The prevalence of total hypothyroidism (including all fractions) was 9.1% [CI 8.2–10.0%]. The prevalence of total hyperthyroidism was 0.8% [CI 0.6–1.1]. A total of 7.5% [CI 6.7–8.3%] of the population tested positive for TPOAbs (≥50 IU/mL). In multivariate logistic regression models, TPOAbs were strongly associated with both hypothyroidism (p < 0.001) and hyperthyroidism (p = 0.005), whereas high UI levels (>200 μg/g creatinine) were associated with hypothyroidism (p < 0.001). The positive association between UI and hypothyroidism remained for both treated (p < 0.001) and untreated (p < 0.05) hypothyroidism, whereas it was especially significant for non-autoimmune (TPOAbs negative) forms (p < 0.001). At UI levels ≥200 μg/g, there was a positive correlation between UI and thyrotropin levels (β = 0.152, p < 0.001) and a negative correlation between UI and free triiodothyronine levels (β = −0.134, p = 0.001).
Conclusion:
According to the data, a large proportion (10%) of the Spanish population has some evidence of thyroid dysfunction. High TPOAb concentrations were associated with both hypo- and hyperthyroidism, whereas high UI concentrations were associated with hypothyroidism.
Introduction
T
Numerous studies from many countries have reported the epidemiology of thyroid dysfunction, although with some variability in the results, probably influenced by different disease definitions, differences in reference ranges and in the laboratory techniques used to measure serum thyroid hormone levels, selection criteria of the studied population, and the influence of circumstances such as genetic background, race/ethnicity, age, sex, and environmental factors such as differences in the iodine nutrition status in the area of study.
All these aspects highlight the need for more information, and in particular, specific data from each country seems to be necessary to address the epidemiology of these highly prevalent disorders adequately.
Interestingly, although the national prevalence of thyroid dysfunction in the U.S. population has been extensively studied in the National Health and Nutrition Examination Survey (NHANES) study (10), such population-based national prevalence studies have hardly been conducted in other populations and, to the authors' knowledge, have not been previously performed in any European country where the available data remain limited to certain geographical areas or cities (11).
The present research aimed to study for the first time the national prevalence of thyroid dysfunction in Spain in a nationwide population-based sample representative of the Spanish adult population.
Materials and Methods
The
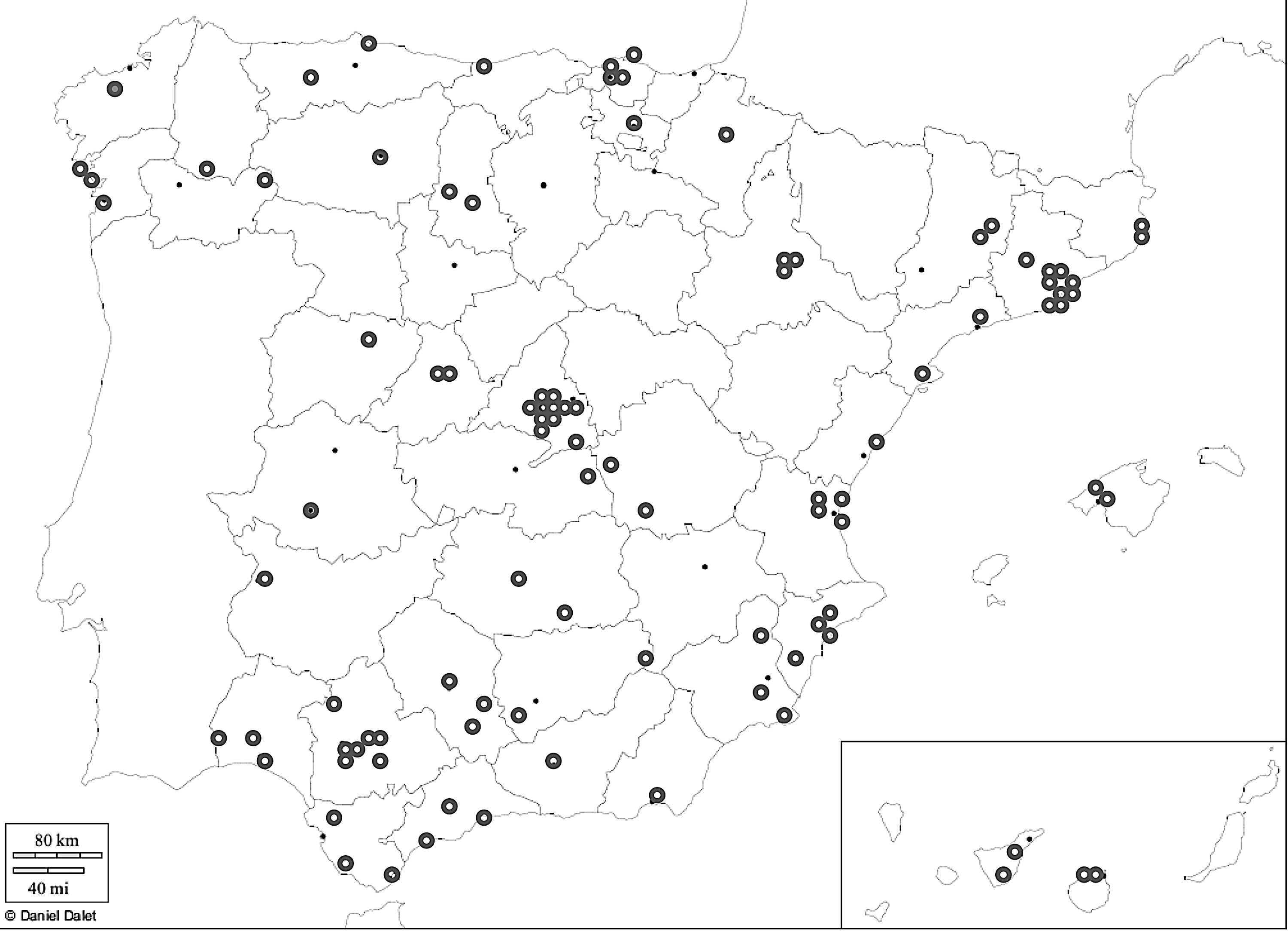
Map showing the 100 clusters included in the
The present study focuses on 4554 subjects (90% of the study sample) in whom thyroid function studies were performed. This sample was composed of 1932 (42.4%) men and 2622 (57.6%) women, with a mean age of 50 years (range 18–93 years). Ninety-one percent of the study participants were native Spanish people.
The study was approved by the ethics and clinical investigation committee of the Hospital Regional de Málaga (Málaga, Spain). Written informed consent was obtained from all participants.
Variables and procedures
The participants were invited to attend a single examination visit at their health center. Information was collected using an interviewer-administered structured questionnaire, followed by a physical examination and blood sampling.
Information on demographic characteristics and smoking status was obtained by questionnaire. Medical history and medications were also recorded. Weight, height, and body mass index (BMI) were measured by standardized methods. Blood samples were obtained in fasting conditions. A random urinary sample (in the morning and in the fasting state) was also collected. Serum and urinary samples were frozen until analyses. Samples were managed by the Hospital Regional Universitario de Málaga-IBIMA Biobank that also belongs to the Andalusian Public Health System Biobank, and the biorepository CIBERDEM (Instituto de Salud Carlos III, Madrid, Spain).
Thyroid function tests
Thyrotropin (TSH), free thyroxine (fT4), free triiodothyronine (fT3), and thyroid peroxidase antibody (TPOAb) concentrations were analyzed using an electrochemiluminescence immunoassay (Modular Analytics E170, cobas e 602; Roche Diagnostics, Basel, Switzerland). The functional sensitivity of the TSH assay was 0.014 mIU/L. The intra-assay coefficients of variation (CV) were: TSH 1.5–1.2%, fT4 1.8–1.6%, fT3 1.3–2.0%, and TPOAb 4.8–2.8%. The interassay CV for the low and high levels of serum TSH, fT4, fT3, and TPOAb quality control materials were 3.5% and 2.7%, 4.17% and 2.64%, 3.78% and 2.21%, and 8.5% and 5.2%, respectively. All samples were analyzed at the laboratory of Biochemistry of the Hospital Regional Universitario de Málaga, which attends a population of 487,857 people from the city of Málaga, Spain. Reference values with correction according to the authors' own studies (13) were as follows: TSH 0.20–5.00 μIU/mL, fT4 11.0–22.0 pmol/L, fT3 3.1–6.8 pmol/L, and TPOAbs <50 IU/L. These values are currently used to define thyroid dysfunction in the reference area of the hospital.
Urinary iodine (UI) was analyzed using the modified method of Benotti and Benotti (14). The intra- and inter-assay CV of the UI assay was 2.01% and 4.53%, respectively. The UI assay was subjected to a program of external quality assessment for the determination of iodine in urine of the Spanish Association of Neonatal Screening (AECNE). The reference material was Seronorm TM Trace Elements Urine, with a mean z-score of 0.3. All samples were analyzed in the Research Laboratory of the Hospital Regional Universitario de Málaga. UI levels were classified in categories according to current World Health Organization, UNICEF, and the Iodine Global Network (formerly International Council for the Control of Iodine Deficiency Disorders) recommendations (15). UI levels in this population (
Classification of thyroid dysfunction
Thyroid dysfunction was defined as follows: • Treated hypothyroidism: individuals treated with levothyroxine at the time of examination. • Untreated overt hypothyroidism: individuals not receiving levothyroxine/thionamides, with TSH levels >5 mIU/L combined with fT4 concentrations below the laboratory's reference range (11.0 pmol/L). • Untreated subclinical hypothyroidism: individuals not receiving levothyroxine/thionamides, with TSH concentrations >5 mIU/L combined with fT4 concentrations at the lower reference limit or higher (11.0 pmol/L). • Total hyperthyroidism: individuals with TSH <0.2 mIU/L and/or on treatment with thionamides. • TPOAbs positive: individuals with TPOAb levels above the reference range (≥50 IU/mL).
Statistical analysis
To study the distribution of TSH in the study sample, the median and the 2.5th and 97.5th percentile values in the total population and in the euthyroid population were calculated. Density histograms were also constructed with the distribution of TSH in the different subgroups after a previous logarithmic transformation.
The prevalence and confidence intervals of the different thyroid dysfunction subtypes were calculated in the global sample and separately for men and women. These prevalence data were adjusted for the age and sex structure of the Spanish population by the direct method. The prevalence of thyroid dysfunction subtypes was also studied separately for each sex in the different age groups. To test the association between thyroid dysfunction and various other factors, a multivariate logistic regression model was used, including age, sex, smoking status (current smokers vs. former/never smokers), TPOAbs (<20, 20–50, 50–100, >100 IU/mL), UI (<50, 50–100, 100–200, 200–300, >300 μg/g creatinine), BMI (<25, 25–30, >30 kg/m2), and the area of residence (center of Spain vs. peripheral areas). Linear regression analyses were also used to test the relation between UI and thyroid hormone levels at different UI levels. Reported p-values were based on two-sided tests, with statistical significance set at 0.05.
Results
TSH distribution in the study sample
The median serum TSH concentration (2.5th–97.5th percentiles) was 2.09 mIU/L (range 0.51–6.64 mIU/L) for the total population and 2.03 mIU/L (range 0.64–4.45 mIU/L) for the euthyroid population. The median TSH concentration (euthyroid population) was higher in women (2.08 mIU/L) than it was in men (1.97 mIU/L; p = 0.004). No significant trend was seen toward a rise in TSH concentrations with increasing age in either sex. Figure 2 represents the distribution on a logarithmic scale of the TSH values in the different subgroups. As can be observed, there was a displacement of the density curve toward lower values in the population with hyperthyroidism, an incomplete overlap in the groups with normal thyroid function and treated hypothyroidism, and a gradual shift to the right in TSH values in the groups with untreated subclinical hypothyroidism and untreated clinical hypothyroidism.
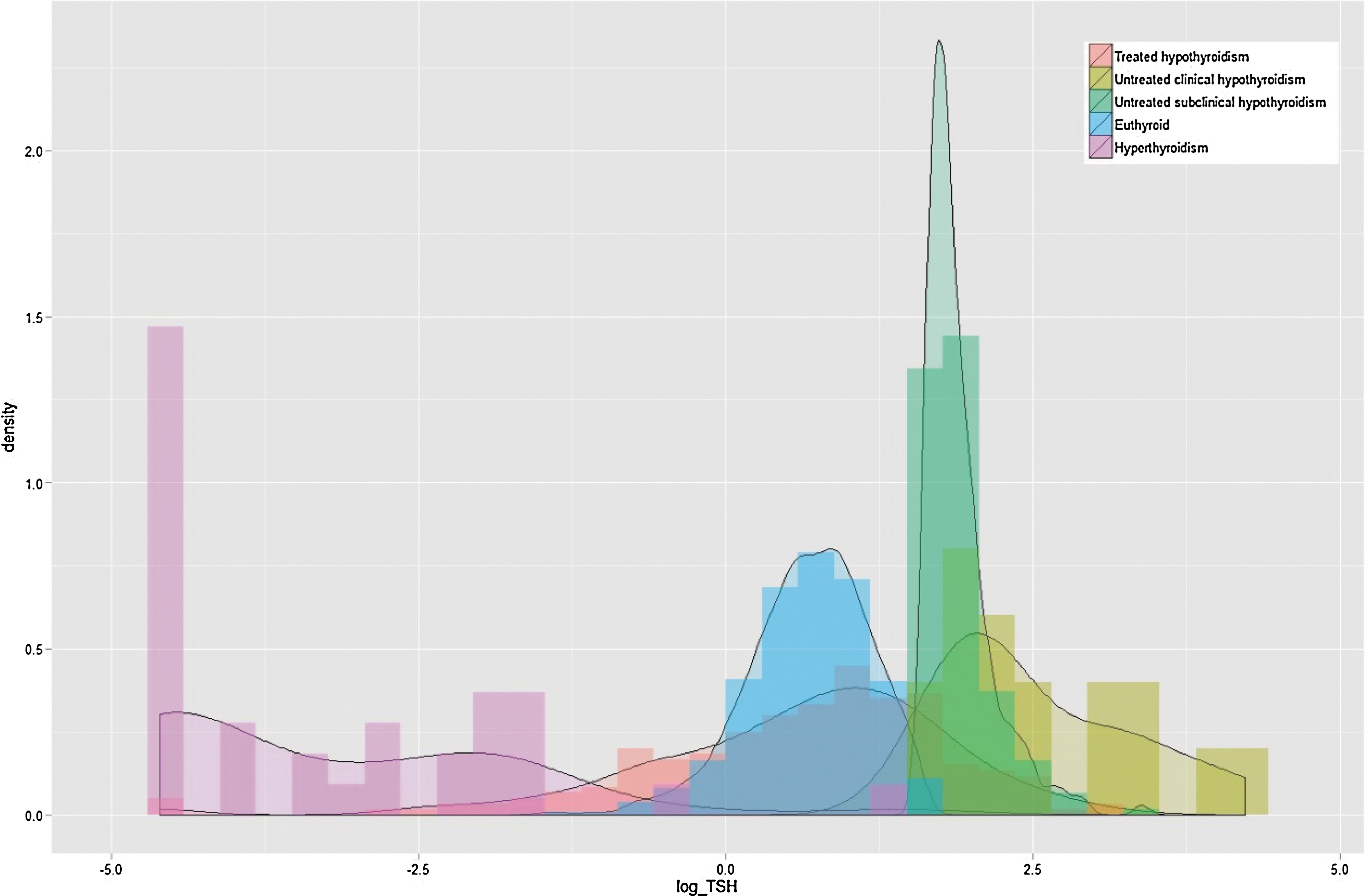
Distribution of the logarithmic values of thyrotropin in the study sample according to thyroid dysfunction subtypes.
Prevalence of thyroid dysfunction
Table 1 reports the prevalence of thyroid dysfunction in the study sample. After adjusting for age and sex structure of the Spanish population, the prevalence of treated hypothyroidism was 4.2% [confidence interval (CI) 3.6–4.9%], whereas the prevalence of untreated subclinical and untreated clinical hypothyroidism was 4.6% [CI 4.0–5.2%] and 0.3% [CI 0.1–0.5%], respectively. Therefore, the prevalence of total hypothyroidism (including all fractions) in the population was 9.1% [CI 8.2–10.0%]. The prevalence of total hyperthyroidism was 0.9% [CI 0.6–1.1%]. This corresponded to a 0.1% [CI 0.0–0.2%] fraction with treated hyperthyroidism, 0.4% [CI 0.2–0.6%] with untreated subclinical hyperthyroidism, and 0.4% [CI 0.2–0.6%] with untreated clinical hyperthyroidism.
All the prevalence estimates have been calculated from a total population of 4554 subjects, except for TPOAb prevalence data, which have been calculated from a total population of 4513 subjects with complete data on thyroid hormones and TPOAbs.
CI, confidence interval; TPOAbs, thyroid peroxidase antibodies.
All thyroid dysfunction phenotypes were more prevalent in women than they were in men. Total hypothyroidism was 13.3% [CI 12.0–14.6%] in women compared with 4.7% [CI 3.8–5.7%) in men (p < 0.001). The prevalence of the corresponding treated, untreated subclinical, and untreated clinical subtypes was 7.1% [CI 6.1–8.1%], 5.7% [CI 4.8–6.5%], and 0.5% [CI 0.2–0.8%] in women versus 1.2% [CI 0.7–1.8%], 3.5% [CI 2.7–4.3%], and 0.0% [CI 0.0–0.1%] in men. Thus, the proportion of treated hypothyroidism (from total) was higher in women (53.4% of the total) than it was in men (25.5% of the total; p < 0.001). Hyperthyroidism was also more prevalent in women, with 1.0% [CI 0.7–1.4%] compared with 0.6% ([CI 0.3–1.0%]; p = NS). Only 85% of women were free of any thyroid dysfunction compared with 95% of men. Additionally, 7.5% [CI 6.7–8.3%] of the population tested positive for TPOAbs (≥50 IU/mL). The corresponding figures by sex were 10.8% [CI 9.6–12.1%] in women compared with 4.1% [CI 3.2–5.0%] in men (p < 0.001). The proportions of individuals who tested positive for TPOAbs were 5.9% in the euthyroid group, 38.7% in the treated hypothyroidism group, 27.6% in the untreated subclinical hypothyroidism group, 58.8% in the untreated clinical hypothyroidism group, and 13.5% in the hyperthyroid group (p < 0.001; Table 2). Figure 3 shows the prevalence of the different thyroid abnormalities in both sexes according to age. The prevalence of treated hypothyroidism (Fig. 3A) increased progressively with age in women, reaching a maximum prevalence in the 50–70 years decades, with a slight decrease in older ages (>70 years), whereas the prevalence of treated hypothyroidism in men remained relatively low in all age groups. In contrast, the prevalence of untreated subclinical hypothyroidism (Fig. 3B) remained relatively stable across all age groups in both sexes (around 4–7% in women and around 3–4% in men). Untreated overt hypothyroidism was very infrequent in both sexes across all age groups (Fig. 3C). Hyperthyroidism (total) was also infrequent and reached a maximum prevalence of 2.3% in women >70 years (Fig. 3D). The population prevalence of TPOAb positive increased with age in women, reaching a prevalence of >14% in the 40–70 years age groups and a decrease in the >70 years age group, similar to the pattern described for the prevalence of treated hypothyroidism (Fig. 3E).
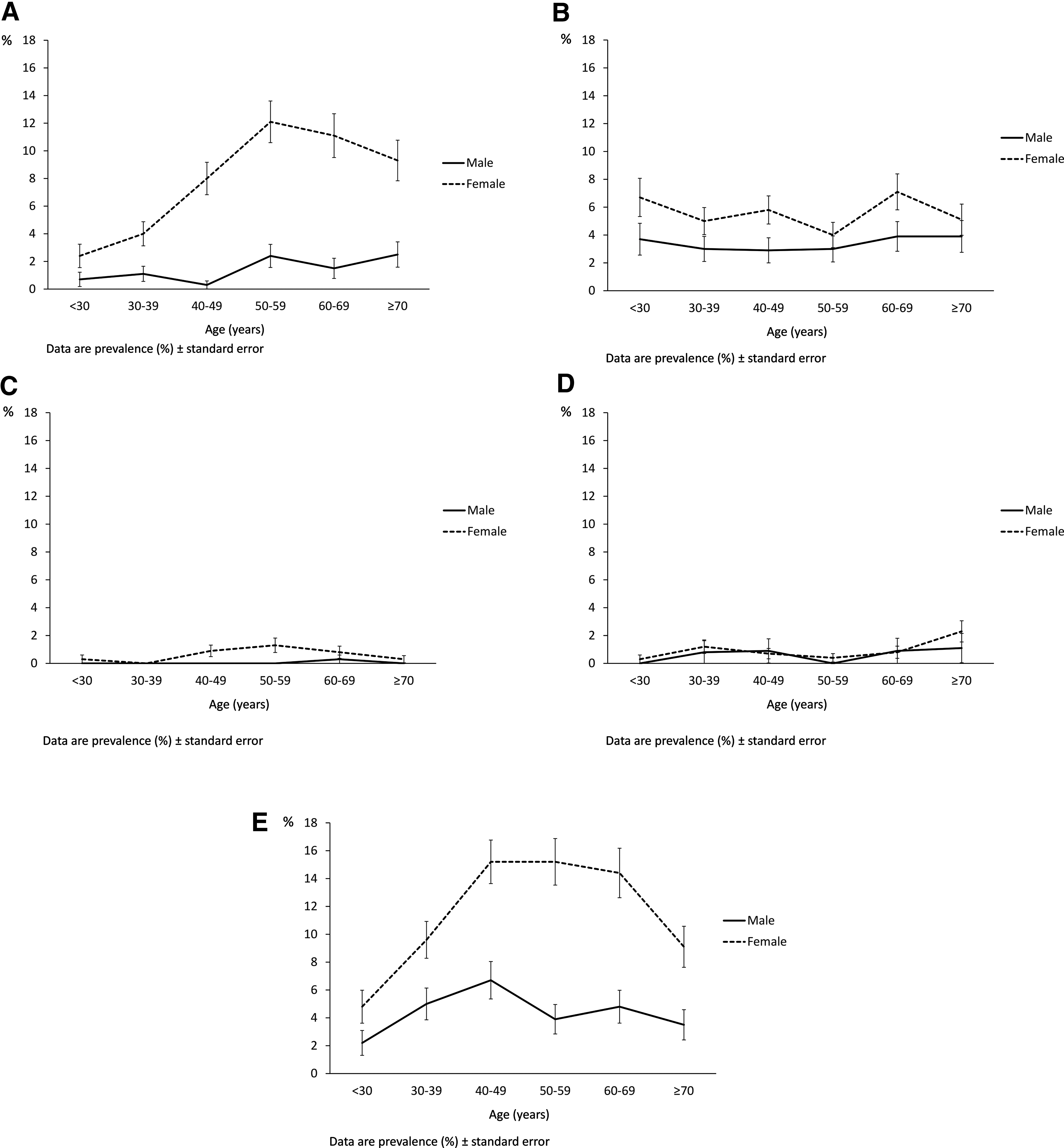
Prevalence of the different thyroid dysfunction phenotypes in both sexes according to age. (
Data are n (%).
Factors associated with thyroid dysfunction
Results of associations between various clinical and demographic variables and the presence of thyroid dysfunction (both hypo- and hyperthyroidism) studied in a multivariate logistic regression model are shown in Table 3. Correcting for these confounders, females were 2.5 times more likely to have hypothyroidism (all types) than men were (p < 0.001), whereas there was not a significant association of thyroid dysfunction with age (p = NS). TPOAbs were strongly associated with both hypothyroidism and hyperthyroidism. In the category with TPOAbs >150 IU/mL, the probability of having hypothyroidism was 10 times higher than it was in the reference category with TPOAbs <20 IU/mL (p < 0.001). In addition, there was around a five times higher probability of having hyperthyroidism in this category when compared with the reference (p < 0.005).
OR, odds ratio.
Additionally, there was a strong positive association between UI and thyroid dysfunction. Compared with the reference category composed of individuals with UI <50 μg/g, the likelihood of having hypothyroidism was more than twofold higher in the UI 200–300 μg/g category (p = 0.002) and more than threefold higher in the UI >300 μg/g category (p < 0.001). There was also an association between hypothyroidism and the area of residence, with a higher probability of hypothyroidism in the center of Spain compared with peripheral areas (p < 0.001). Medium UI levels between zones were similar (116.8 μg/g and 119.8 μg/g; p = NS). This association was mostly driven by treated (p < 0.001) versus untreated (p = 0.087) forms of hypothyroidism (data not shown). There was a trend for lower odds of hypothyroidism in smokers compared with former/never smokers (odds ratio [OR] = 0.82) and higher odds in obese versus normal weight (OR = 1.26), although these associations were not significant. Interestingly, all the associations found for hypothyroidism were virtually mimicked by those of hyperthyroidism, although none of the latter was statistically significant.
To explore the association between UI and hypothyroidism further, the results were disaggregated according to hypothyroidism subtypes (Fig. 4A and B). As shown in Figure 4A, increasing concentrations of UI were associated with an increased prevalence of both treated (p < 0.001) and untreated (p < 0.05) hypothyroidism. However, as seen in Figure 4B, high UI levels were associated exclusively with an increase in non-autoimmune (TPOAb negative) forms of hypothyroidism (p < 0.001), whereas autoimmune (TPOAb positive) hypothyroidism was not significantly increased. The study also tested for linear association between UI and thyroid hormone levels (TSH, fT4, fT3; Table 4). As shown in Table 4, at UI <200 μg/g, there was no significant association between UI and thyroid hormones, whereas at UI levels ≥200 μg/g, there was a weak but highly significant positive correlation between UI and TSH levels (β = 0.152, p < 0.001) and a negative correlation between UI and fT3 levels (β = −0.134, p = 0.001). Individuals with treated hypothyroidism and/or TPOAb positive were excluded from this last analysis.
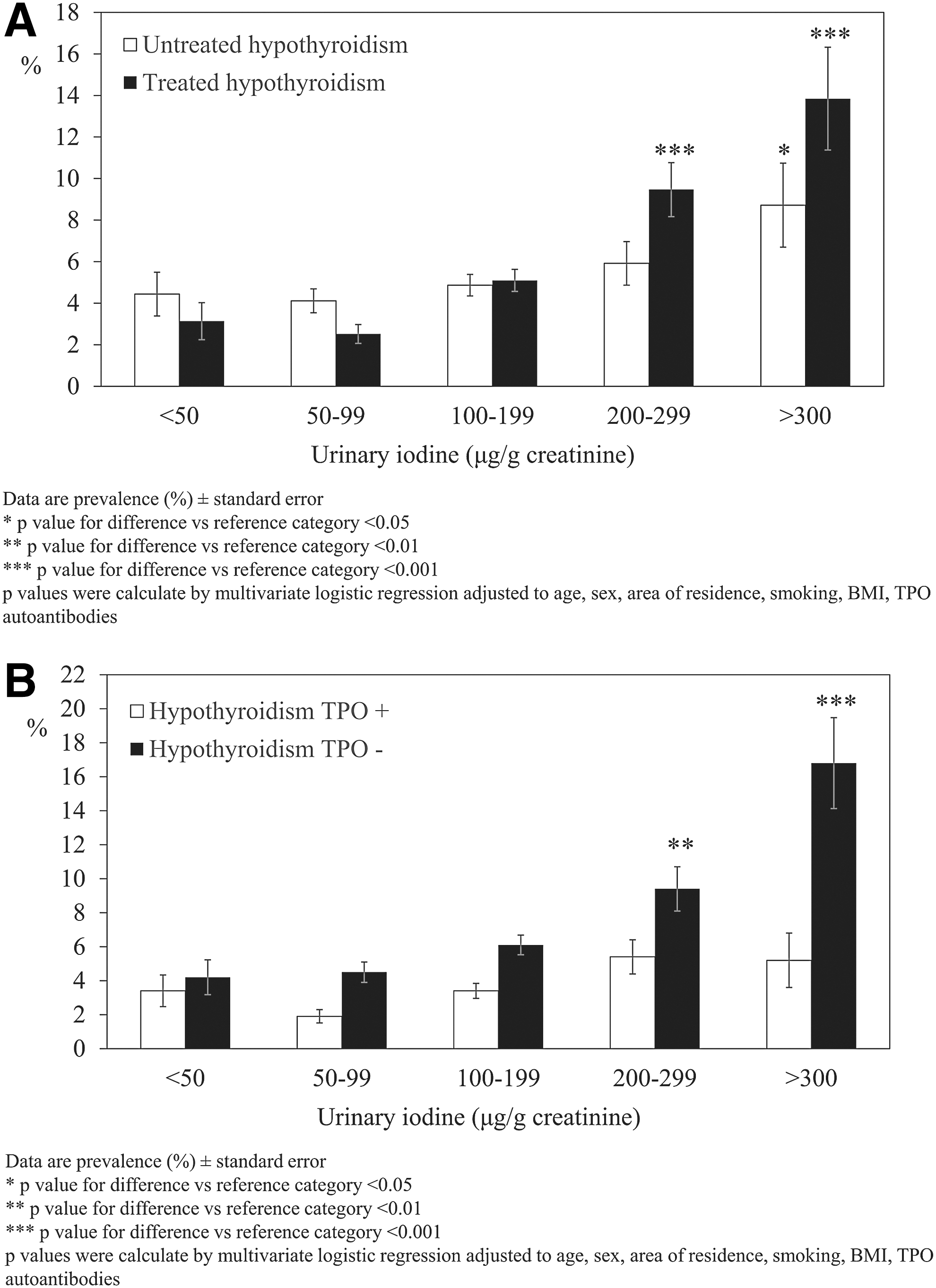
Prevalence of hypothyroidism according to urinary iodine levels disaggregated by hypothyroidism subtypes. (
β standardized coefficients and p-values were calculated by linear regression adjusted for age, sex, area of residence, smoking, and BMI.
Individuals with treated hypothyroidism and who were TPOAb positive were excluded from the analyses.
UI, urinary iodine; TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; BMI, body mass index.
Discussion
The results of this first national prevalence study in Spain show that a large proportion of the adult population of the country (approximately 10%) has thyroid dysfunction. These results were mainly driven by treated (4.2%) and subclinical forms (4.6%) of hypothyroidism, whereas clinical untreated hypothyroidism (0.3%) and hyperthyroidism (0.9%) were much more infrequent. There was a clear predominance of thyroid dysfunction in women compared with men, especially for hypothyroidism, and a higher proportion of women with hypothyroidism were treated. Treated hypothyroidism increased with age in women, whereas untreated forms of hypothyroidism remained relatively stable with age in both sexes. This pattern of thyroid dysfunction is within the range seen in other studies and is consistent with an area with sufficient iodine intake. In a recent meta-analysis of European studies, the prevalence of untreated subclinical and clinical hypothyroidism was estimated at 3.8% [CI 3.48–4.15%] and 0.37% [CI 0.27–0.48%], respectively, whereas hyperthyroidism was estimated at 0.75% [CI 0.73–0.77%] (11). Accordingly, in the NHANES study, the prevalence of untreated subclinical and overt hypothyroidism in the United States was estimated at 4.3% and 0.3%, respectively, and 1.3% of the population had hyperthyroidism (10). The present results are consistent with these previous reports. Also, the prevalence data are very similar to the findings of a previous study performed in Spain (Catalonia), which reported a prevalence of untreated subclinical hypothyroidism, untreated clinical hypothyroidism, and hyperthyroidism of 3.5%, 0.2%, and 1.5%, respectively (17). There is less information regarding the prevalence of treated hypothyroidism. In the HUNT study in Norway, the prevalence of treated hypothyroidism was 5.0% in women and 1.0% in men in 1995–1997, and this increased to 8.0% and 2.0%, respectively, in 2006–2008 (18). These last figures are again very similar to the 7.1% prevalence in females and 1.2% in men found in the present study.
If it is assumed that these prevalence data for thyroid dysfunction apply for the overall adult population of Spain aged >18 years (38,310,165 inhabitants according to the 2015 census) (19), this would result in the alarming figure of more than three million individuals with hypothyroidism and >300,000 with hyperthyroidism in Spain, many of whom remain undiagnosed.
Regarding TPOAb-positive prevalence data, the prevalence of subjects who tested positive for TPOAbs in the
Clinical categories associated with thyroid dysfunction were also studied, and as in other previous studies (22 –24), a strong association between TPOAb concentrations and both hypo- and hyperthyroidism was found, which further confirms its use as a sensitive marker of autoimmune thyroid disease. A higher probability of hypothyroidism was also found in the center of Spain versus peripheral areas. The association was mostly driven by treated (p < 0.001) versus untreated (p = 0.087) hypothyroidism, so it is possible that differences in clinical practice in different parts of Spain could partially explain the results. It is, however, noteworthy that this same geographical pattern in the prevalence of hypothyroidism has recently been reported in a study from India (25).
It is also noteworthy that after adjusting for the rest of confounders, age was not associated with a higher prevalence of thyroid dysfunction in this study, and a trend toward a rise in TSH concentrations with increasing age reported by Surks and Hollowell (26) was not observed either.
More strikingly, a strong positive association was found between UI and hypothyroidism, which has not previously been reported in the Spanish population. However, the results are concordant with other previous cross-sectional data, which have consistently found a higher prevalence of hypothyroidism associated with high levels of UI. Knudsen et al. reported an increased prevalence of TSH values >3 mIU/L in the population with high iodine excretion (>150 μ/g) (27). This was also true after correcting for the influence of age and sex in a logistic regression analysis (OR = 1.77 [CI 1.1–2.2]). In a recent study from China, the prevalence rates of subclinical hypothyroidism were 20.09%, 10.41%, and 2.25% for the iodine excess, sufficient, and deficient iodine groups, respectively (28). TSH was correlated with excess iodine intake (b = 1.764, p = 0.001) and with deficient iodine intake (b = −1.219, p = 0.028) (28). Similarly, in coastal regions of Japan, high UI was also significantly correlated with subclinical hypothyroidism (29). In another study from eastern Europe, the prevalence of subclinical hypothyroidism ranged from 4.2% in iodine-deficient areas (Northern Hungary: medium UI 72 μg/g creatinine) to 10.4% in an area with borderline iodine sufficiency (Slovakia: medium UI 100 μg/g creatinine) to 23.9% in an area of abundant iodine intake (Eastern Hungary: medium UI 513 μg/g creatinine) (30). Iodine-related hypothyroidism in the general population has also been reported in follow-up studies. In three communities with a medium UI of 88 μg/L, 214 μg/L, and 634 μg/L, respectively, the prevalence of overt and subclinical hypothyroidism was 3.2 times higher in a more than adequate iodine intake region and 6.8 times higher in excessive iodine intake regions. The incidence of subclinical hypothyroidism showed the same trend: 13 times higher in more than adequate iodine intake regions and 14.5 times higher in excessive iodine intake regions (31). Some other studies speak about a possible increase in the incidence of hypothyroidism after iodination. In Pescopagano, Italy, the prevalence of hypothyroidism was higher in 2010 compared with in 1995 (5.0% vs. 2.8%; p < 0.005) after iodine prophylaxis was started. Hypothyroidism increased in all age groups, with the exception of subjects >75 years (32). Longitudinal studies conducted in Denmark have also shown an increased incidence of overt hypothyroidism (33) and thyroid hormone prescriptions (34) after the beginning of an iodization program. Interestingly, although iodine has been associated with exacerbation of thyroid autoimmunity (35), the exclusive increment of TPOAb-negative forms of hypothyroidism associated with high UI that have been found in this study supports other non-autoimmune-mediated mechanisms. Such mechanisms could be mediated by a direct inhibitory effect of iodine on the thyroid (36). Animal experiments have also shown that prolonged high iodine intake can inhibit the activity of deiodinase-II in the hypothalamus and pituitary, resulting in increased TSH production (37), although the significance of these findings in humans is currently unknown. Interestingly, other previous epidemiological studies have shown this same pattern of association between UI and non-autoimmune forms of hypothyroidism (29,30). It is important to note that the present results are based on cross-sectional associations, so that no causal effect can be inferred. Moreover, the contribution of possible confounders, or even the possibility of a reverse causation (e.g., an increase of iodine intake and/or modifications of iodine metabolism in subjects with hypothyroidism leading to higher UI concentrations), cannot be discarded. In a previous longitudinal experiment from our group, oral supplementation with 100, 200, or 300 μg of iodine to healthy individuals for six months did not modify TSH or thyroid hormone levels (38). More research, especially prospective and experimental data, is needed in this field.
Strengths of this study include that the prevalence of both hyperthyroidism and hypothyroidism (treated and unrecognized) have been analyzed in a large sample of subjects representative of the general adult population of Spain with a national study perspective, and that the association between a number of clinical and demographic variables and the presence of thyroid dysfunction in this country have been explored.
However, the study also has a few limitations. First, the level of participation was relatively low (55%), and there was greater participation by women. To overcome this limitation, all the prevalence data in this study were adjusted for the age and sex structure of the Spanish population with little variation in the results, making selection bias unlikely. Second, thyroid examinations or sonograms for the evaluation of goiter or thyroid size were not included. Third, the study was cross-sectional and hence does not include individual changes over time. Further evaluations of the cohort will provide this information.
In conclusion, according to the present data, a large proportion (10%)of the Spanish population shows some evidence of thyroid dysfunction, mainly driven by treated and subclinical forms of hypothyroidism. High TPOAb concentrations were associated with both hypo- and hyperthyroidism, whereas high UI concentrations were associated with hypothyroidism.
Footnotes
Acknowledgments
We wish to acknowledge the kind collaboration of the following entities: The Spanish Diabetes Society, the Spanish Diabetes Federation, and the Ministry of Health Quality Agency. Our profound appreciation goes to the primary-care managers and personnel of the participating Health Centers, as well as to Drs. Luis Forga and. Felipe Casanueva for their inestimable help in the management of the northern zone. Thanks go to all the fieldworkers, nurses, and dietitians (I. Alonso, A. Arocas, R. Badia, C.M. Bixquert, N. Brito, D. Chaves, A. Cobo, L. Esquius, I Guillén, E. Mañas, A.M. Megido, N. Ojeda, R.M. Suarep, and M.D. Zomeño), without whose work it would not have been possible to carry out the study, and to all the people who voluntarily participated in the study. The authors also wish to thank Olga Perez Gonzalez (FIMABIS) for her statistical support.
The study was supported by CIBER in Diabetes and Associated Metabolic Disorders—CIBERDEM (ISCIII—Ministerio de Ciencia e Innovación), Ministerio de Sanidad y Consumo, Spanish Society of Diabetes—SED, Consejería de Salud Junta de Andalucía (0256/2007), Instituto de Salud Carlos III (PI11/02755) (PI14/00710), Sociedad Andaluza de Endocrinología, Diabetes y Nutrición (Beca SAEDYN).
The researchers of the
Author Disclosure Statement
The authors declare no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.