
Abstract
Background:
Measuring thyrotropin (TSH) eluted from a dried blood spot (DBS) is used to screen an estimated 30 million newborns annually for congenital hypothyroidism (CH). Newborn thyroid screening has eliminated cretinism from the industrialized world and decreased the adverse effects of unrecognized CH on neurocognitive development. Hematocrit, a pre-analytic variable that affects the measurement of TSH from a DBS, contributes to the imprecision of DBS TSH measurement and could account for false-negative and false-positive DBS newborn screening test results. To assess whether variations in hematocrit found in newborns have a clinical effect in DBS-based newborn thyroid screening, the effects of hematocrit variability on the measurement of DBS TSH were studied.
Methods:
U.S. Centers for Disease Control and Prevention procedures for manufacturing DBS performance testing standards were used to generate DBSs from blood samples, with hematocrits of 35%, 40%, 45%, 50%, 55%, 60%, and 65% and serum TSH concentrations of 6.3 ± 0.4 and 26.6 ± 8.0 mIU/L. TSH was measured in the eluates of four replicate DBS 3 mm punches at each hematocrit using the Thailand Ministry of Public Health Newborn Screening Operation Center enzyme-linked immunosorbent assay. Data were analyzed using a linear mixed-effects model.
Results:
Based on the mixed-effects model, hematocrit significantly affected DBS TSH measurement (p < 0.001). A 1% increase in hematocrit resulted in a 0.06 mIU/L decrease in eluate TSH when TSH was 6.3 + 0.4 mIU/L, and a 0.21 mIU/L decrease in eluate TSH when TSH was 26.6 + 8.0 mIU/L.
Conclusions:
DBS TSH is significantly affected by the blood sample hematocrit. The pre-analytic variability due to hematocrit is independent of TSH assay sensitivity, specificity, precision, repeatability, and reference intervals. The effect of hematocrit on DBS TSH measurement is clinically relevant, could account for geographic and ethnic variation in the incidence of CH, and may result in both false-positive and false-negative CH screening results. Individual newborn and population-specific hematocrit correction factors may improve the precision of DBS TSH measurement.
Introduction
S
Newborn screening procedures use a two-step process: a pre-analytic phase consisting of specimen collection, DBS preparation, and transport, and an analytic phase in which TSH and/or T4 is measured in a filter paper chad eluate. Arbitrary cutoff values for TSH and/or T4 are used to identify infants for whom additional biochemical testing is indicated. The pre-analytic phase of newborn screening represents a source of analytic variability. Inadequate sample collection occurs in 4–8% of infants tested (6). Additional sources of pre-analytic variability include hematocrit, specimen stability, ambient temperature and humidity, and time from collection to analysis.
Hematocrit (packed cell volume) is reported to have significant effects on the measurement of thyroid hormones from a DBS, and hematocrit bias is recognized as a source of pre-analytic variability in newborn screening (7 –11). Hematocrit alters the rheological properties of blood dried onto filter paper (12), and affects the distribution of TSH within a DBS (8), the quantitative recovery of a number of serum markers from a DBS (13,14), and the predictive value of diagnosing metabolic disease from a DBS (15). Hematocrit represents the percent of a blood sample volume that is occupied by cells. Variations in hematocrit result in reciprocal variations in the amount of liquid (e.g., serum) in a unit volume of blood. As hematocrit increases, serum volume decreases. Because TSH and T4 circulate in serum and the amount of serum per unit volume of blood varies as a function of hematocrit, TSH and T4 concentrations are expressed as the amount of TSH in a defined volume of serum (Fig. 1). Hematocrit values among healthy newborns range between 55% and 68% (16). There are ethnic and geographic variations in newborn hematocrit. In populations with a high prevalence of anemia, newborn hematocrits as low as 30% are frequent (17). Conversely, significantly higher hematocrits are found in newborns born at altitude (18).
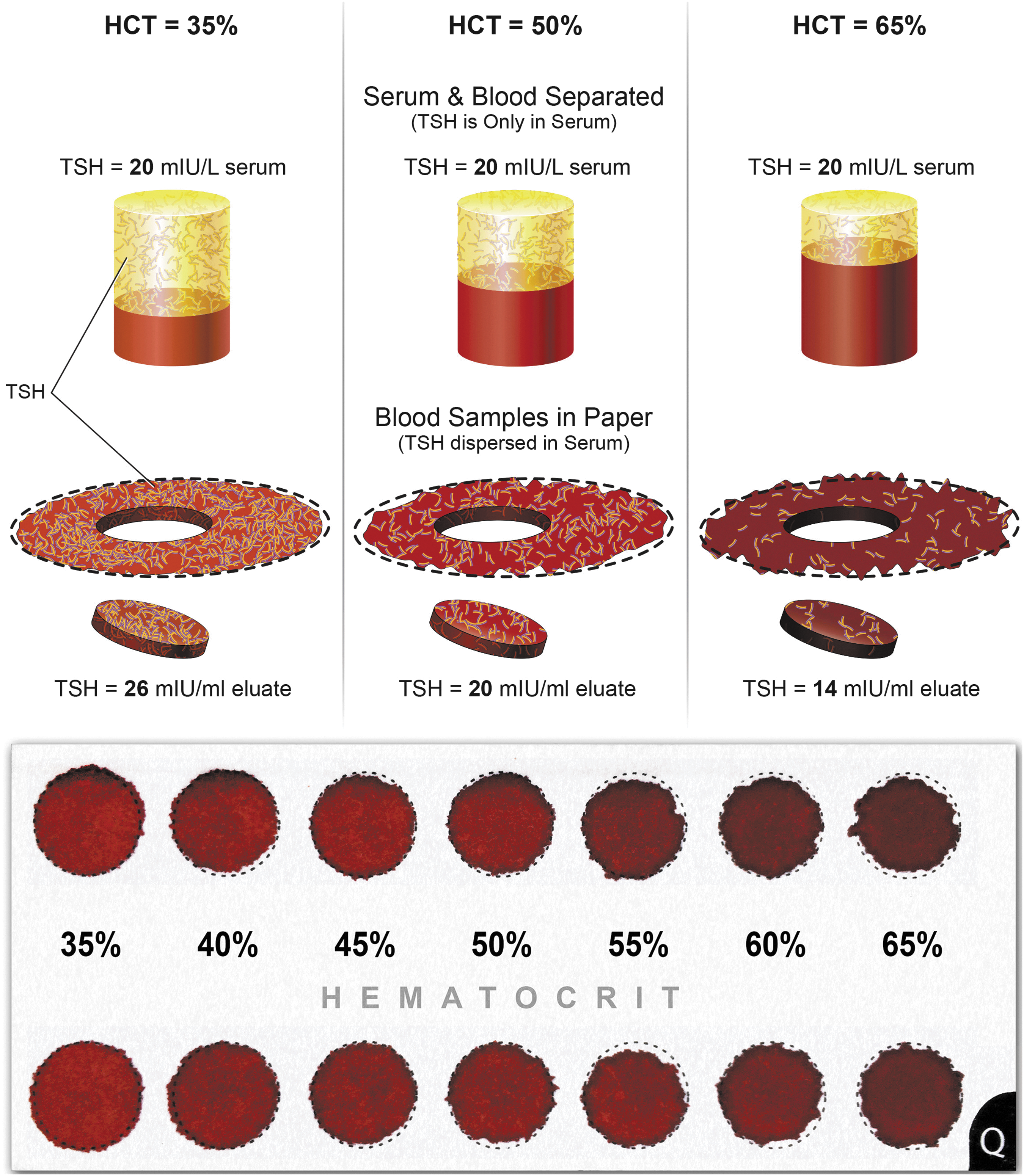
The top panel graphically represents the effect of hematocrit on the quantitative recovery of thyrotropin (TSH) from a dried blood spot (DBS). The bottom panel illustrates the effect of hematocrit on the rheological properties of blood. Two 100 μL aliquots of blood samples with hematocrits between 35% and 65% were spotted onto Guthrie cards. Hematocrit increases blood viscosity. Thus, the diameter of the DBS decreases as the hematocrit increases.
Although hematocrit bias has been described previously, the quantitative effects of this pre-analytic source of error have not been measured. As a result, it is not known whether hematocrit bias is clinically significant. In this study, experiments were conducted to quantify the effect of variations in hematocrit found in Thai newborns on DBS TSH measurement and to evaluate whether the hematocrit bias can alter clinical decision making.
Materials and Methods
Hematocrit effects experiments
Hematocrit was measured as part of routine care in 349 newborns aged >48 hours born in two regional Thailand hospitals. Venous blood was collected in capillary tubes, centrifuged, and the hematocrit expressed as percent packed cell volume. The mean hematocrit from both hospitals was compared to the U.S. Centers for Disease Control and Prevention (CDC) reference hematocrit of 50% using a t-test.
The U.S. CDC procedure for producing hematocrit-adjusted quality control performance samples was used to produce blood samples with hematocrits between 35% and 65% (19). Aliquots of ethylenediaminetetraacetic acid (EDTA) and heparin plasma or serum with TSH concentrations 6.3 ± 0.4 and 26.6 ± 8.0 mIU/L, measured by enzyme-linked immunosorbent assay (ELISA) (20), were added to washed packed red blood cells obtained from normal volunteers to obtain blood samples with hematocrits of 35%, 40%, 45%, 50%, 55%, 60%, and 65%. One hundred microliters from each hematocrit sample was spotted onto Whatman 903 filter paper, dried at room temperature overnight, and stored at 4°C for 24 hours. TSH was measured by The Thailand Ministry of Public Health Newborn Screening Operation Center ELISA (20) in the eluate of four replicate 3 mm DBS punches at each hematocrit. This resulted in a total of 325 DBS samples.
Statistical methods
A t-test was used to assess whether the assumption of 50% hematocrit is true for the subset of infants in Thailand. To quantify the effects of newborn hematocrit variability on TSH measurement, a simulation analysis was used to determine the effect of using 50% hematocrit versus using the actual hematocrit value. Using the range of hematocrits found in Thai newborns, 10,000 virtual DBS samples were modeled at a concentration of 20 mIU/L. Each virtual DBS sample was derived from a normal distribution centered at 20 mIU/L, with a standard deviation of 2 mIU/L. This simulation takes into account TSH assay variability, derived from a standard normal distribution, to estimate the deviation of TSH concentration from a cutoff TSH concentration of 20 ± 2 mIU/L. Using the simulated data and assuming that the incidence of primary CH is 1:3000, the positive predictive value (PPV), sensitivity, and specificity were estimated when using a standard 50% hematocrit to calculate TSH and when using an individual's actual hematocrit.
TSH measured on four to six chads from each DBS represents repeated measures that are not independent. Thus, a mixed-effects model was used to model DBS TSH. Hematocrit was included as a predictor variable. Overall, inter-matrix and intra-DBS variability were included as error terms. Specimen matrix type is incorporated through inter-matrix variability. p-Values were computed to measure the statistical significance of each variable included in the model. An alpha of 0.05 was used in both analyses.
Results
Hematocrit effects
Of the 349 Thai newborns sampled, 191 (54.7%) were male. Hematocrit values ranged from 33% to 68%, with a mean of 51.2% and standard deviation of 6%. A t-test was completed, assuming a population mean of 50% based on the CDC reference value for hematocrit. The mean hematocrit was 51.2% with a confidence interval of 50.6–51.9%, which is significantly different from 50% (p < 0.001). In this population, it is not correct to assume a hematocrit of 50% for all infants.
Using the simulated Thai newborn data, and assuming that the incidence of primary CH is 1:3000, the PPV is 0.1%, the sensitivity is 62%, and the specificity is 80% when using a standard 50% hematocrit to calculate TSH around the cutoff of 20 mIU/L. Using the true hematocrit, the PPV is 4.9%, the sensitivity is 99%, and the specificity is 99%. This simulation shows the importance for using an individual's actual hematocrit value when calculating DBS TSH rather than a standard assumption of 50% hematocrit.
Figure 2 displays the relationship between the hematocrit, specimen matrix of the blood from which the DBS was obtained, and the quantitative recovery of TSH from the blood spot. Using a mixed-effects model, DBS TSH was predicted with hematocrit (%) as a coefficient in the model and intra-DBS variability and inter-matrix variability as error terms. Both models found a significant negative relationship between hematocrit and DBS TSH (p < 0.001), meaning that as hematocrit increases, DBS TSH decreases (Table 1). At a TSH concentration of 6.3 ± 0.4 mIU/L serum, a 1% increase in hematocrit resulted in a 0.06 mIU/L decrease in elute TSH. At a TSH concentration of 26.6 ± 0.8 mIU/L serum, a 1% increase in hematocrit resulted in a 0.21 mIU/L decrease in elute TSH.
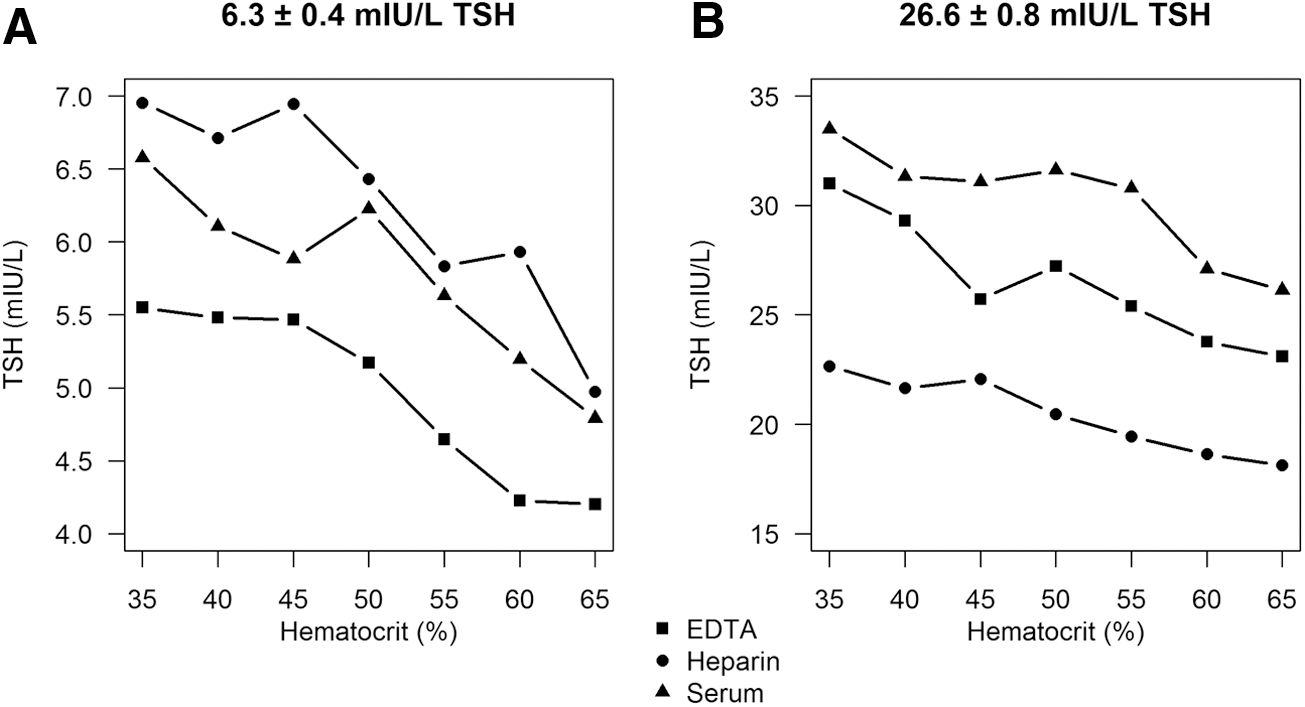
The effect of hematocrit on the quantitative recovery of TSH from DBS: (
DBS, dried blood spot; TSH, thyrotropin; CI, confidence interval.
Discussion
The present findings agree with and expand upon prior observations showing that hematocrit variations in the range found in Thai newborns represent a significant source of variability in DBS TSH measurement (7 –11,21,22). The effect of hematocrit on TSH measurement from a DBS is clinically significant, as TSH measured in a DBS from a hypothyroid newborn with a hematocrit of 65% will be 3.15 mIU/L lower than the TSH concentration measured in a DBS with a 50% hematocrit. Because screening programs use arbitrary cutoff values (e.g., a TSH ≥20 mIU/L) to identify infants who need evaluation for primary CH, the effect of hematocrit on TSH measurement can result in incorrectly identifying a hypothyroid infant as euthyroid when the infant's hematocrit is >50% (false negative) and incorrectly identifying a euthyroid infant as potentially hypothyroid when the infant's hematocrit is <50% (false positive).
False-negative newborn thyroid screening is not uncommon (23). French investigators in 1991 reported a 3% false-negative rate. “Laboratory error” accounted for 46% of missed diagnoses, and false-negative test results were responsible for 54% (24). Oregon investigators gave a figure of 8% false-negative rate (25). The New England Screening Program measured false-negative tests results at 9% in 1982 (26). Northern Ireland in 1986 reported a 9% false-negative rate (27). A 2010 study from Greece showed that 28% of newborns with CH were misdiagnosed (28). A 2015 review comparing CH screening results from states that conduct a single screening test to results from states that routinely collect a second specimen at 8–14 days of age found that states that use a single DBS screen did not detect 11.8% of CH cases (29). Explanations for false-negative test results include iodine excess, mutations in genes involved in thyroid hormone biosynthesis (e.g., DUOX2 mutations), inter-fetal transfusion in monozygotic twins, delayed maturation of the hypothalamic–pituitary–adrenal axis, preterm birth, hospitalization in a NICU, and intrauterine growth retardation (30 –32). Furthermore, false-positive newborn screening tests can result in increased psychosocial morbidity and parent–child dysfunction (33). Compared to infants with normal newborn screening test results, children with false-positive newborn screening tests are twice as likely to visit an emergency room or be hospitalized (34).
The procedures currently used to collect, process, and transport DBSs, the pre-analytic phase of clinical laboratory testing, are based on processes developed in the 1960s to mail specimens from a nursery to a newborn PKU screening laboratory (5). The infrastructure necessary for centralized DBS newborn screening limits the use of this extremely successful public-health tool to the industrialized world. Newborn thyroid screening in the developing world is an unmet need that represents a major public-health challenge. Among the 130 million babies born worldwide annually, only 25–30% are screened, and every year, approximately 1.4 million children with CH are not detected prior to the onset of permanent neurological damage (35,36).
Current newborn screening recommendations and guidelines do not include consideration of pre-analytic factors, such as inadequate specimen collection, hematocrit effects, specimen deterioration in transit, and rheological effects resulting in the heterogeneity of TSH distribution within a DBS, as sources of variability in newborn CH screening. Regional variations in newborn hematocrit values may contribute to ethnic and geographic differences in the incidence of CH (37 –42). The correlation between DBS TSH and serum TSH is not robust (r 2 = 0.391) (43,44). American Academy of Pediatrics Guidelines recommend reporting newborn TSH results as mIU/L serum (45). British newborn screening programs double the TSH concentration measured in a DBS eluate to report serum TSH concentrations (46). In Japanese newborn screening programs, the amount of TSH measured in a DBS eluate is multiplied by 1.6, and this value is reported as a serum TSH concentration (47). These correction factors assume a hematocrit of 50–60% and 100% quantitative recovery of TSH from a DBS. Because the TSH concentration in a DBS reflects the volume of serum present in the blood spot prior to drying, the hematocrit is integral to calculating TSH accurately (Fig. 1). As the mean hematocrit of Thai newborns is not 50%, using an assumed hematocrit of 50% to extrapolate serum TSH concentration from the TSH measured in an eluate represents a potential source of clinically significant analytic imprecision. Individual and population-specific hematocrit correction factors may improve the precision of DBS TSH measurement.
The effect of hematocrit on an assay's quantitative recovery is analyte specific. In contrast to the results obtained for TSH, DBS measurement of prostate-specific antigen (PSA), 25-OH vitamin D, and IGF-1 and IGF binding protein 3 have been reported to show <10% variation with hematocrit (48). The explanation given for these observations is that even though the amount of serum in a blood spot decreases as the hematocrit increases, increases in hematocrit increase blood viscosity. As a result, the spread of a blood spot on filter paper decreases as the hematocrit increases (Fig. 1). This, in turn, effectively increases the total amount of blood per filter paper surface area and counteracts the effects of decreased serum on the quantitative recovery of these analytes from a DBS. Studies on PSA (49), 25-OH vitamin D (50), IGF-1, and IGF binding protein 3 (51), however, used DBSs with hematocrits lower than those found in newborns.
Eliminating hematocrit as a source of bias in the measurement of DBS TSH can be accomplished by a number of methods. These include correcting for hematocrit by either measuring the sample's hematocrit or a surrogate hematocrit marker, such as DBS potassium, or using specially folded filter papers (52 –55). These approaches involve additional diagnostic tests and materials not widely available in nurseries where DBSs are prepared. A second approach for taking hematocrit bias into account would be to establish screening cutoff values that take into account hematocrit variability. This would result is a lowering of cutoff values. Many studies have shown that lowering cutoff values in newborn CH screening increases both the number of false-positive test results as well as the recall rate (46,56 –59).
This study focused on the effects of hematocrit on the newborn screening cutoff value that is used by the Thailand Ministry of Public Health's Newborn Screening Laboratory (20 mIU/L). It was not designed to evaluate the effect of hematocrit on the wide range of cutoff values used in DBS newborn thyroid screening programs around the world (37,59 –63). A newborn's TSH concentration is affected by many factors, including maternal iodine status, iodine antisepsis at delivery, mode of delivery, smoking behavior of the mother, and multiple pregnancies. The rationale for cutoff values in newborn CH screening is based on historical opinion, newborn care protocols, assay methods, screening strategies (i.e., repeat newborn screening for infants at risk for false-negative primary screening tests), resource availability, and missed cases of CH (39). Because of a lack of defined cutoffs, newborn screening programs traditionally start with a conservative cutoff and, over time, refine this value based upon data obtained to identify a cutoff value that results in absent false-negative tests (64). Invariably, this has resulted in a progressive decline in cutoff values in an attempt to improve rates of case identification and decrease the need for further testing (65). The results presented here show that hematocrit contributes to the imprecision of DBS-based newborn screening methods. Lowering the cutoffs used to identify infants who need additional evaluation represents one approach to minimizing false-negative newborn screening results. This approach will decrease the number of false negatives, but will also increase the number of false positives. Improving TSH assay precision by addressing hematocrit variability represents an alternative strategy. Additional studies are needed to determine whether correcting for hematocrit improves the sensitivity of DBS-based newborn thyroid screening without decreasing specificity.
There are a number of potential limitations to this study. They include the intra-chad TSH variability that results from both heterogeneous distribution of TSH within a single DBS and from variance in the TSH immunoassay. Additionally, use of TSH as a screening analyte is not able to detect central CH (66). Lastly, this study was performed on Thai newborns using the Thailand Ministry of Public Health TSH ELISA. The applicability of these results to newborn screening programs in other populations remains to be determined.
In summary, pre-analytic factors have clinically relevant effects on the quantitative recovery of TSH from a DBS. These effects can produce both false-positive and false-negative test results. A false-negative newborn screen can result in missed and delayed diagnoses of primary CH. A missed or delayed diagnosis of CH causes a permanent loss of as much as 0.5 IQ points per day during the first month of life and an increase in the severity of other neurocognitive deficits (67).
Footnotes
Author Disclosure Statement
R.P. provides consulting services to and J.E. owns equity in a company that makes newborn screening products. The remaining authors have no conflicts of interest to disclose.