
Abstract

I read with interest the report by Suzuki et al. (1) on thyroid ultrasound examinations in Fukushima, which concludes that the “prevalence of childhood thyroid cancer in Fukushima was determined to be 37.3 per 100,000 with no significant differences between evacuated and non-evacuated areas.” However, I identified three major limitations of their study.
First, grouping 59 municipalities into four areas is inappropriate. Although the average effective dose of municipalities in the same area should be homogeneous, as summarized in Figure 1, in which municipalities are ranked in the order of the average effective dose, it is quite variable. To confirm this, a chi-square test was conducted for municipality by 16 dose categories, ranging from <1 mSv to >15 mSv. To avoid violation of an assumption of large sample distribution, 10 dose categories of >6 mSv were collapsed into a single category. Thus, the degree of freedom of the cross table is (# of municipalities in an area – 1) × (6 dose categories – 1). The distribution of estimated external dose is significantly different among municipalities in the evacuated zone (χ2 (df=60) = 60,000, p < 1e-16), Nakadori (χ2 (df=100) = 90,000, p < 1e-16), and Iwaki and Soma (χ2 (df=10) = 1000, p < 1e-16).
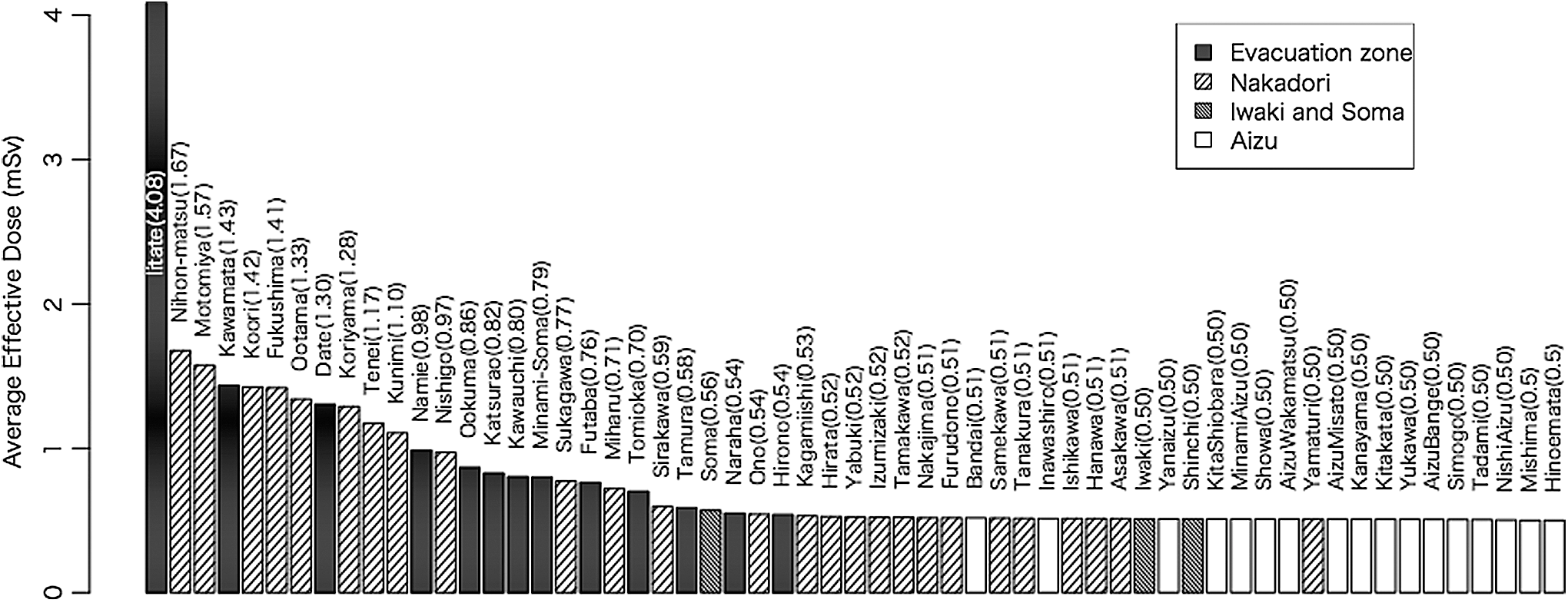
Average effective dose for 59 municipalities and classification by Suzuki et al. (1). Note: Pattern corresponds to four areas by Suzuki et al. Average dose in parentheses. Calculated based on “Appendix 4: Estimated external radiation doses by region in the first four months (from 11 March through 11 July) excluding radiation workers (as of 31 March 2016)” (
Second, the research lacks statistical power. UNSCEAR (2), which estimated the health risk of radiation in Fukushima, reported that the statistical power of their analysis is 11%. Assuming a linear dose–response relationship, the difference between the average lifetime thyroid dose for the two areas is 10 mSv and 20 years of observation. The statistical power in the study by Suzuki et al., which was based on three years of observation without using dose information, is expected to be weaker than the one established by UNSCEAR. The insignificant odds ratio appears to be due to the lack of statistical power. Actually, the study by Suzuki et al. (1) and the corresponding research plan (3) do not include information on statistical methods, assumed risk model and dose differences, and statistical power.
Third, the conclusions drawn from comparisons with unaffected areas cannot be sustained for the following reason. Screening results from children in Fukushima are compared to those for 4365 children in uncontaminated areas: Aomori, Yamanashi, and Nagasaki (4). Suzuki et al. concluded that “such proportions were not statistically different from those in Fukushima” without test statistics. According to my re-analysis, the distribution is significantly different (χ2 (df=3) = 149.5, p < 0.01). Moreover, as reported in the original studies on the screening of three prefectures, “age composition (0- to 2-year-olds are not included), inter-observer differences, iodine intake, socio-ecological status, and family history or past history” are different (4). Hence, a direct comparison seems inappropriate.
Although I acknowledge the authors' effort in investigating thyroid screening, proper research design and statistical analysis are necessary to reach a firm conclusion.
Footnotes
Author Disclosure Statement
The author declares that there are no conflicts of interest.