
Abstract
Background:
Prognostic factors are essential for risk stratification in patients with differentiated thyroid carcinoma (DTC). The role of stimulated postoperative thyroglobulin (sPOTg) has been well established in adult DTC population, but it remains unclear in children and adolescents. This study aimed to evaluate potential prognostic factors in children and adolescents with DTC, with special emphasis on sPOTg analysis.
Methods:
Individuals aged ≤18 years at diagnosis were selected from a cohort of DTC patients attending the thyroid clinic of a tertiary university-based hospital. Baseline clinical and oncological characteristics, interventions, disease status, and outcomes were obtained from medical records. Clinical variables included in the univariate analysis were sex, age at diagnosis, tumor size, the presence of lymph node and distant metastasis, and sPOTg. Additionally, sPOTg was evaluated using the area under the receiver operating characteristic curve analysis.
Results:
Thirty-two children and adolescents with DTC (28 girls, 87.5%; the mean age at diagnosis = 14.7 ± 3.2 years) were included in this study. Thirty-one (96.9%) patients had papillary thyroid carcinoma. The median tumor size was 2.0 cm (P25–75 = 1.6–3.5), 22 patients (68.8%) had lymph node disease, and 5 (15.6%) had distant metastasis at diagnosis. All patients underwent total thyroidectomy, and 29 (90.6%) received radioactive iodine therapy. After a median follow-up of 5.0 years (P25–75 = 2.0–10.0), disease status was available for 27 patients: 15 (55.6%) patients were disease free, six (22.5%) had biochemical disease, and six (22.2%) had persistent structural disease (two cervical and four distant metastasis). Prognostic factors associated with persistent disease in the univariate analysis were lymph node and distant metastasis at diagnosis and sPOTg. According to the receiver operating curve analysis (n = 17 patients), the best sPOTg cutoff to predict disease-free status was 31.5 ng/mL, with a sensitivity and specificity of 100%.
Conclusion:
The data demonstrate that
Introduction
T
DTC in children is, in many ways, a distinct disease from DTC in adults (4 –8). Although children most often present with extensive and aggressive disease and have a higher frequency of recurrence, their prognosis is excellent, with a low mortality rate, even if advanced disease is present (4 –9). Recently, the American Thyroid Association (ATA), recognizing these differences, released two separate guidelines for thyroid nodules and DTC specific to children and adults (10,11). The current recommendation for the initial management of these young patients is total thyroidectomy followed by radioiodine therapy as indicated and levothyroxine suppressive therapy (4,5,10).
Currently, one of the most important steps in the evaluation of patients with DTC is risk stratification for recurrence (12). For that reason, the knowledge of possible prognostic factors is essential. Several prognostic factors have been well established and cited in the ATA Adult DTC Guidelines: extremes of age, larger tumors, multicentricity, extrathyroidal extension, lymph node metastasis, vascular invasion, and postoperative thyroglobulin (POTg) (11). In contrast, there are conflicting results related to these prognostic factors in children and adolescents (13 –15).
One study published in 2011 by Mihailovic et al. (13) evaluated potential prognostic factors in children and concluded that younger age at diagnosis, less aggressive initial treatment, and tumor multifocality were associated with disease recurrence. These authors identified no association between DTC recurrence and sex or lymph node metastasis or distant metastasis (13). Conversely, Vaisman et al. (14) found that the only two factors associated with persistent disease were lymph node metastasis and distant metastasis. In this cohort, age, sex, tumor size, and multicentricity were not predictors of the success of initial therapy (14). Of interest, the POTg—a well-stablished risk predictor for adults with DTC (16)—has not been evaluated in young patients.
The objective of the present study was to evaluate factors associated with persistent disease, with a particular focus on stimulated postoperative thyroglobulin (sPOTg) analysis, in a contemporary DTC cohort of children and adolescents attending a referral center hospital in southern Brazil.
Materials and Methods
Patients and study design
Patients with a histological diagnosis of DTC before the age of 18 years, from a cohort of DTC patients attending the Thyroid Outpatient Clinic of the Endocrine Division of Hospital de Clínicas de Porto Alegre from 2000 to 2015, were included in this report. The institution is a tertiary-care university teaching hospital in southern Brazil and is a referral center for DTC treatment.
Treatment protocol and follow-up
The DTC treatment protocol at the institution consists of performing total thyroidectomy, administering an ablative or therapeutic dose of radioactive iodine (RAI) as indicated, and levothyroxine suppression therapy (17 –19). Decisions regarding cervical lymph node dissection were made at the discretion of the surgical team at the center where the patients underwent surgery. Follow-up duration was defined as the time between the thyroidectomy and the last medical visit to the clinic. During the first evaluation, the following data were recorded for each patient: patient demographics; tumor characteristics (date of diagnosis; histological features; extrathyroidal extension, and lymph node involvement); and treatment (surgery, RAI, and other interventions). Each patient was classified using the 7th edition of the TNM/AJCC staging system (I or II). N0 status was determined by clinical examination of the neck, preoperative and postoperative neck ultrasound (US) imaging, macroscopic examination during surgery, and pathological examination of patients with lymph node resection.
The follow-up protocol called for an initial assessment at three to six months post surgery, which included a physical examination of the neck and measurements of serum thyroglobulin (Tg) levels under thyrotropin (TSH) suppression (Tg-T4), and antithyroglobulin antibody (TgAb). In a second evaluation 6–12 months after the initial treatment, serum Tg was measured under conditions of a stimulated TSH (sTg) with endogenous hypothyroidism (TSH >30 mIU/L). Neck US was also performed during the first year of follow-up. Patients classified as disease free (see below) were scheduled for annual visits that included a physical examination of the neck and measurements of Tg-T4 and TgAb. Patients with persistent disease were scheduled for medical visits twice a year. Additional imaging studies (e.g., neck US, diagnostic 131I whole-body scan [WBS], and computed tomography [CT]) were undertaken as indicated when clinical or laboratory findings raised suspicion of persistent or recurrent disease.
sPOTg
sPOTg was measured post thyroidectomy and before administration of RAI. In patients not selected to receive RAI, the sPOTg was measured in the first year after thyroidectomy. In both groups, sPOTg measurement was made under stimulated conditions and was considered appropriate if TSH was >30 mIU/L (endogenous hypothyroidism). Serum levels of TgAb were accessed in the same blood sample from which sPOTg was measured, and patients with positive results were excluded from this analysis.
Outcomes
Disease status was defined based on clinical examination, Tg-T4 and sTg levels, neck US, post-RAI WBS (when available), and additional imaging exams when indicated.
“Disease free” was defined as no clinical or imaging evidence of tumor (i.e., no uptake outside the thyroid bed on the post-treatment WBS, and no imaging evidence of tumor on neck US), undetectable (<1 ng/mL) Tg-T4 levels, and sTg levels <2 ng/mL.
Persistent disease was subdivided into biochemical or structural disease. Biochemical disease was defined as Tg-T4 values ≥1 ng/mL or sTg levels ≥2 ng/mL without structural evidence of disease. Structural disease of the cervical lymph node was determined by imaging studies and biopsy-proven disease (cytology or histology) with or without abnormal Tg values. Patients diagnosed with persistent disease were evaluated for additional treatment (e.g., surgery or radioiodine), depending on the site involved.
Recurrence was defined as new biochemical or structural evidence of disease detected in a patient who had previously been determined to be disease free.
Laboratory analysis
Serum Tg measurements were performed using immunoradiometric assays (from 2000 to 2002, radioimmunoassay; 2002 to 2010, electrochemiluminescence; and 2010 until the present, chemiluminescence—ECLIA, Modular E-170; Roche) with functional sensitivities of at least 1 ng/mL. TgAb were measured using the passive agglutination method from 2000 to 2010 and chemiluminescence (Siemens Healthcare) from 2010 until the present. After each new technique had been implemented, necessary standardization and validation procedures were performed. TSH levels were measured by electrochemiluminescent immunoassay (ADVIA Centaur XP; Siemens Healthcare). All tests were conducted in the central laboratory of the Hospital de Clínicas de Porto Alegre.
Statistical analysis
Clinical and laboratory data are reported as the mean ± standard deviation or median and percentiles 25 and 75 (P25–75) for continuous variables and absolute numbers and percentages for categorical variables. Comparative analyses were performed using an unpaired Student's t-test, Mann–Whitney U-test, Fisher's test, or chi-square test, as appropriate.
Clinical variables, such as sex, age at diagnosis, tumor size, lymph nodal and distant metastases, and sPOTg were evaluated as potential prognostic factors for DTC by univariate analysis. sPOTg was also assessed using the area under the receiver operating characteristic (ROC) curve with sPOTg as a continuous prognostic variable and disease status at follow-up as the outcome variable.
All tests were two-tailed, and all analyses were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). A two-tailed p-value <0.05 was considered statistically significant.
Results
Clinical characteristics
A group of 32 children and adolescents with DTC (28 girls, 87.5%; M age at diagnosis = 14.7 ± 3.2 years) were included in this study. Thirty-one (96.9%) patients had PTC, and one (3.1%) had FTC. The median tumor size was 2.0 cm (P25–75 = 1.6–3.5). Cervical metastasis was identified in 22 (68.8%) patients, and distant metastasis in five (15.6%) patients. Regarding TNM staging, 27 (84.4%) were classified as stage I, and five (15.6%) as stage II. Clinical and oncological characteristics of the 32 patients are described in Table 1.
Data are expressed as the mean ± standard deviation, median (percentiles 25–75), or frequencies. RAI, radioactive iodine.
All patients underwent total thyroidectomy, and 29 (90.6%) received RAI therapy with a median activity of 100 mCi (P25–75 = 100–150). Post-therapy WBS were performed in 28 patients; 23 (82.1%) patients presented only cervical uptake, and 5 (17.9%) had distant metastases (all in the lung).
Disease status
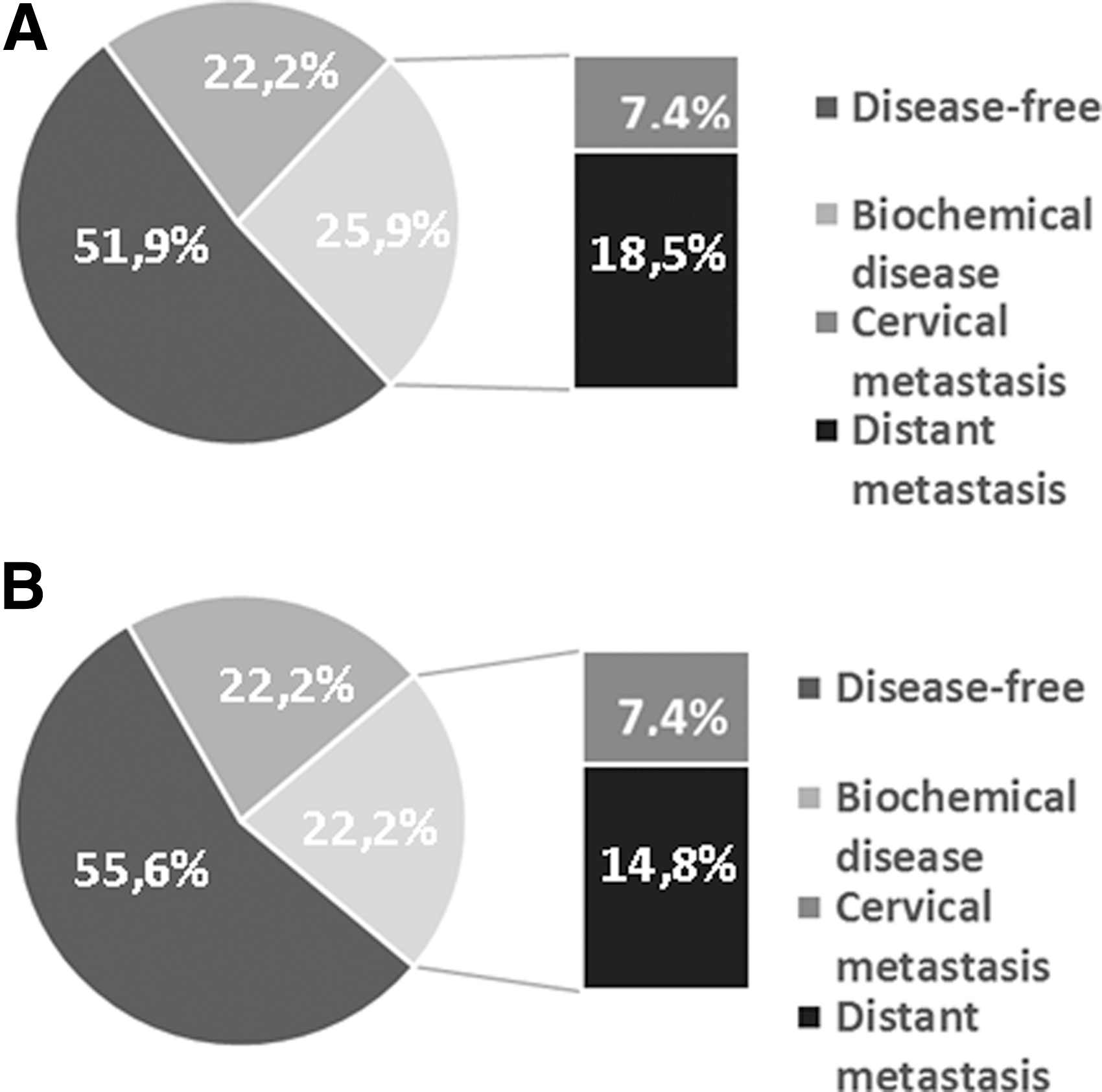
During the first year of follow-up, disease status was available for 27 patients (Fig. 1A): 14 (51.9%) patients were considered disease free, six (22.2%) had biochemical persistent disease, and seven (25.9%) had persistent structural disease (two cervical and five distant metastasis).
Disease status after a one-year follow-up (
After a median follow-up of 5.0 years (P25–75 = 2.0–10.0), disease status was available for the 27 patients (Fig. 1B): 15 (55.6%) patients were considered disease free, six (22.2%) had persistent biochemical disease, and six (22.2%) had persistent structural disease (two cervical and four distant metastasis). No recurrence or deaths were registered.
Prognostic factors
To investigate factors associated with disease-free status at follow-up, patients were grouped into disease-free or persistent-disease categories. Univariate analysis indicated that patients with persistent disease had a higher proportion of lymph node metastasis (100.0 vs. 46.7%; p = 0.003) and distant metastasis (41.6 vs. 0.0%; p = 0.01). The sPOTg was significantly higher in the group of patients with persistent disease (638.0 vs. 8.5 ng/mL; p < 0.001). Male sex, age at diagnosis, and tumor size were not associated with persistent disease (p = 0.075, p = 0.359, and p = 0.338, respectively; Table 2).
Data are expressed as the mean ± SD, median (percentiles 25–75) or frequencies.
Tg, thyroglobulin.
sPOTg as a prognostic factor for DTC
Data for sPOTg and disease status at follow-up were available for 19/32 patients included in this study. Of these, two were ex
Thus, 17 patients were evaluated. The time interval between surgery and sPOTg was a median of 3.0 months (P25–75 = 1.5–8.0). All patients but one received RAI: a female, aged 15 years old at diagnosis, with a 2.0 cm PTC, without lymph node metastasis or distant metastasis (low-risk, T1bN0M0). Her sPOTg was already undetectable one month after surgery and continued to be undetectable without evidence of disease after four years of follow-up.
The median value of sPOTg was 11.2 ng/mL (P25–75 = 7.5–418.5), with a median of 8.5 ng/mL (P25–75 = 5.2–11.1) for patients classified as disease free, and 638.0 ng/mL (P25–75 = 125.0–2297.0) for patients with persistent disease (p < 0.001). The maximum value of sPOTg among patients considered disease free (n = 10) was 13.5 ng/mL, whereas patients with persistent disease (biochemical or distant; n = 7) had a minimum sPOTg value of 49.5 ng/mL. Table 3 shows the individual sPOTg levels, the time between surgery and its measurement, current disease status, and follow-up data for these patients.
To evaluate the performance of sPOTg in predicting persistent disease, a ROC curve was used, which resulted in an area under the curve of 1.0 [confidence interval (CI) 1.0–1.0]. A sPOTg level of 31.5 ng/mL was determined as the optimal cutoff point to predict disease-free status, with a sensitivity and specificity of 100%.
No significant changes in the sPOTg values or ROC curve were observed when the patient who did not receive RAI was excluded from the analysis.
Discussion
Identification of patients who are at greater risk of adverse outcomes is a critical step in the management and follow-up of DTC patients. This study shows that sPOTg is a powerful prognostic tool to predict disease status at follow-up in children and adolescents with DTC.
POTg has been suggested as a prognostic factor in adult patients with DTC (16,20 –25). A recent meta-analysis demonstrated that POTg has a high negative predictive value (94.2% [CI 92.8–95.3]) for persistent disease, with the best cutoff value of 10 ng/mL for the prediction of the absence of biochemical or structural evidence of disease (16). However, the studies included in this meta-analysis involved mostly adult patients (average age ranging from 40.6 to 49.2 years). In fact, these data may not be applicable to pediatric patients, since this type of tumor in children differs from that identified in adult populations, not only in pathophysiology and clinical presentation but also in long-term outcomes (10). Additionally, the data suggest that serum Tg levels might be higher in children compared with adults with a similar extent of disease (10,26,27). Thus, differences can be expected in the analysis of POTg between children and adults, particularly regarding optimal cutoff value for these populations. Nevertheless, no previous studies have evaluated the use of POTg as a prognostic marker specifically in a pediatric population.
The present results show a significant difference in sPOTg values in patients with disease-free status when compared with those with persistent disease at follow-up (8.5 vs. 638.0 ng/mL, respectively). Interestingly, the sPOTg cutoff value of 31.5 ng/mL is higher than those previously reported in adult population studies, which ranged from 5.0 to 30.0 ng/mL (16). A potential explanation for the differences between adults and children/adolescents sPOTg cutoff values is the more aggressive presentation of DTC in young patients, with larger tumors, lymph node metastasis, and distant metastasis.
In the present cohort, the presence of lymph node metastasis and distant metastasis were associated with persistent disease in short- and long-term outcomes. These findings are similar to those found in a previous study (14) that identified lymph node metastasis and distant metastasis as the two most important prognostic factors in young patients with DTC. Furthermore, in agreement with the present results, these authors found no statistical significance between sex, tumor size, or age at diagnosis and persistent disease. In contrast, a recent study that included 118 children and adolescents (15) showed that sex and metastatic disease (lymph node and distant) are important prognostic factors in children with DTC. Moreover, they found ATA risk stratification useful in predicting early and long-term outcomes in the pediatric population.
Based on the present data, sPOTg results can help to guide the follow-up of young patients with DTC. Those with POTg values <31.5 ng/mL had a better prognosis, requiring less intensive treatment and monitoring. Conversely, patients with sPOTg >31.5 ng/mL were at high risk of persistent disease, a condition that warrants more aggressive treatment and follow-up.
This study has some strengths. First, the fact that all patients included in this analysis were followed at the same institution ensures similar therapeutic and follow-up approaches. The exclusion of patients with TgAb-positive minimizes the possibility of false-negative sPOTg values. However, the relatively small number of patients and the fact that the analysis is restricted to only one center experience are limitations for the interpretation of the ROC curve analysis and the external validity of the findings, a fact that should be acknowledged. Another aspect to be considered is that although a median of five years is a reasonable time of follow-up for assessing clinical outcomes, a more extensive period should be observed for definitive conclusions. Notwithstanding, considering the rarity of DTC in this population and the lack of effective risk stratification strategies, the role of sPOTg as a prognostic risk stratification tool in the pediatric population is of considerable interest.
In conclusion, this study demonstrates that lymph node metastasis, distant metastasis, and sPOTg are useful prognostic factors in young patients with DTC. Of particular interest, sPOTg seems to have a promising role as a tool for identifying children and adolescents with DTC at high risk of persistent disease.
Footnotes
Acknowledgments
This work has been made possible by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundo de Incentivo a Pesquisa (FIPE), and Programa de Apoio a Núcleos de Excelência (PRONEX)/Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS). We wish to thank Dr. Alceu Migliavacca, Dr. José Ricardo Guimarães, and Dr. Diego Mossmann, surgeons at our hospital, for the surgical management of our patients.
Author Disclosure Statement
The authors have nothing to declare.