
Abstract
Background:
Distant metastases (DM) are a rare occurrence in well-differentiated thyroid carcinoma. The aim of this study was to analyze the clinical, pathologic, and molecular features of primary thyroid carcinoma with low-risk histology that develop DM.
Methods:
A detailed clinicopathologic review and targeted next-generation sequencing were performed on a cohort of well-differentiated thyroid carcinoma lacking gross extrathyroidal extension, extensive vascular invasion, or significant lymph node metastases but exhibiting DM.
Results:
Primary well-differentiated thyroid carcinoma with low-risk histologic features and DM was a rare occurrence, accounting for only 3% of metastatic non-anaplastic thyroid carcinoma. All 15 cases meeting the inclusion criteria harbored DM at presentation. The majority (11/15) of these tumors were follicular variant of papillary thyroid carcinoma (PTC), especially the encapsulated form (n = 8). The remaining patients harbored encapsulated Hürthle cell carcinoma (n = 2), encapsulated follicular carcinoma (n = 1), and an encapsulated papillary carcinoma classical variant (n = 1). Of the 12 encapsulated carcinomas, 10 had capsular invasion only and no vascular invasion. Ninety-two percent of the tumors exhibited extensive intra-tumoral fibrosis. Among the eight tumors that were subjected to next-generation sequencing analysis, a RAS mutation was the main driver (5/8), and TERT promoter mutation was highly prevalent (6/8). In four cases, TERT promoter mutations were associated with RAS or BRAF mutations. BRAF-mutated classical variant of papillary carcinoma also presented with DM but was less common (1/8). In 11/15 cases, the clinician was able to diagnose distant disease based on the clinical presentation. In 3/4 incidental cases that were genotyped, TERT promoter mutations were found.
Conclusions:
When DM occur in primary thyroid carcinoma with low-risk histology, they are almost always found at presentation. The majority are encapsulated follicular variant of PTC with capsular invasion only. TERT promoter mutations occur at a higher rate than that seen in PTC in general and may help explain the aggressive behavior of these histologically deceptive primary carcinomas.
Introduction
O
Materials and Methods
Study population
The study was approved by the Institutional Review Board of Memorial Sloan-Kettering Cancer Center (MSKCC, New York, NY). The institutional database was searched for patients diagnosed, treated, and followed by the endocrinology service at MSKCC for metastatic non-ANA FCDC between 1983 and 2009. These individuals developed DM either at the initial presentation or during clinical follow-up. A total of 123 patients with adequate pathologic data and clinical information were identified from this database and were included in the present study. Additionally, 11 cases of well-differentiated primary thyroid carcinomas with low-risk histology and DM were retrieved from the MSKCC pathology database and were also included.
Definition of primary thyroid carcinomas with low-risk histology
Primary well-differentiated FCDC without evidence of poorly differentiated component, EVI, gross ETE beyond the thyroid, and/or significant amount of nodal metastasis to neck lymph nodes were considered as low-risk histology. Thus, the histotypes included were PTC, follicular carcinoma (FTC), and Hürthle cell carcinoma (HCC). Significant metastatic lymph node disease was defined as pathologically confirmed metastatic thyroid carcinoma to more than five cervical lymph nodes and/or a metastatic lymph node measuring at least 1 cm in greatest dimension. These tumors were subjected to a meticulous histopathologic re-review by two endocrine pathologists (R.G. and B.X.).
Pathology review
Tumor size was measured as the maximal diameter of the resected tumor specimen. Mitotic rate was determined by counting 10 high power fields (HPFs, 400 × , field size 0.24 mm2) with an Olympus microscope (U-DO model BX41; Olympus America, Inc., Center Valley, PA) in the areas of greatest concentration of mitotic figures. Capsular invasion was defined as complete penetration of the capsule by the tumor, and the number of these foci was recorded. The presence of vascular invasion was noted only when such foci were present within or beyond the capsule in accordance with criteria outlined by the Armed Forces Institute of Pathology (AFIP) fascicle (16). Briefly, only when the invasive focus protruded into the lumen of the vessel in a polypoid manner covered by endothelial cells, or when it was attached to the vessel wall or associated with thrombus formation, was it considered true vascular invasion. Areas of vascular invasion that were closely adjacent to one another were counted as separate foci. The capsular and vascular invasion was subdivided into two categories: focal (<4 invasive foci) and extensive (≥4 foci). The presence or absence of microscopic ETE into the perithyroid soft tissue stroma was documented. Microscopic resection margins were categorized as positive (tumor at the inked margin) or negative (no tumor at the inked margin). Finally, when a regional lymph node sampling was performed during the initial surgery, the number of lymph nodes, metastatic status, size, presence of extranodal extension, and histological type of the metastasis were also recorded. Poorly differentiated carcinoma (PDC) was defined using the MSKCC criteria (17). In brief, a diagnosis of PDC was rendered when a tumor exhibited tumoral necrosis or elevated mitotic index of ≥5 mitotic figures per 10 HPFs (400 × ), regardless of the growth pattern and nuclear features.
Clinical review
The patient's charts were reviewed to record the following clinical parameters: age at diagnosis, sex, serum thyroglobulin (Tg) level at presentation and after total thyroidectomy, serum thyrotropin (TSH) levels after thyroidectomy, timing of the DM (i.e., at the initial presentation or during clinical follow-ups), site(s) of DM, presenting symptoms especially those attributed to DM, and disease status at the last follow-up. Additionally, gross extension beyond the thyroid (GET), defined as any appreciable gross adhesion and/or frank invasion of the primary thyroid carcinoma or metastatic carcinoma from a neck lymph node to the adjacent structures observed during the initial operation and confirmed histologically, was documented.
Molecular analysis
DNA was extracted from formalin-fixed paraffin-embedded (FFPE) tumor sections and matched benign tissue. Eight primary well-differentiated thyroid carcinoma with low-risk histology and adequate DNA material were subjected to massive parallel high-output sequencing using MSKCC-IMPACT™ (MSKCC Integrated Mutation Profiling of Actionable Cancer Targets; MSKCC, New York, NY) platform, which is a hybridization capture-based assay for targeted deep sequencing of all exons and selected introns of 410 key cancer genes, encompassing the majority of established oncogenes and tumor suppressor genes (18).
Results
From 123 patients with non-ANA FCDC with DM, 74 (60%) patients had DM at the time of initial clinical presentation, while the remaining 49 (40%) developed DM during follow-ups. The vast majority (97%) of patients had at least one of the following high-risk features: a pathologic diagnosis of PDC (n = 65; 53%), EVI (n = 62; 51%), GET documented during the initial thyroidectomy ± neck dissection (n = 21; 17%), and/or significant volume of metastatic disease in the neck lymph nodes (i.e., >5 lymph nodes and/or the largest involved lymph node >1 cm in size; n = 4; 3%; Fig. 1). In contrast, only 4/123 (3%) patients had a well-differentiated carcinoma without the above-mentioned high-risk histologic features in their primary. An additional 11 patients were also retrieved from the MSKCC pathology database (outside the data limit of the endocrinology database, as well as cases referred to the hospital) who developed DM and were diagnosed with well-differentiated thyroid carcinomas without PDC, EVI, GET, and significant nodal disease. In total, 15 patients had low-risk histology in their primaries and DM. In all 15 cases, DM was found at initial presentation.
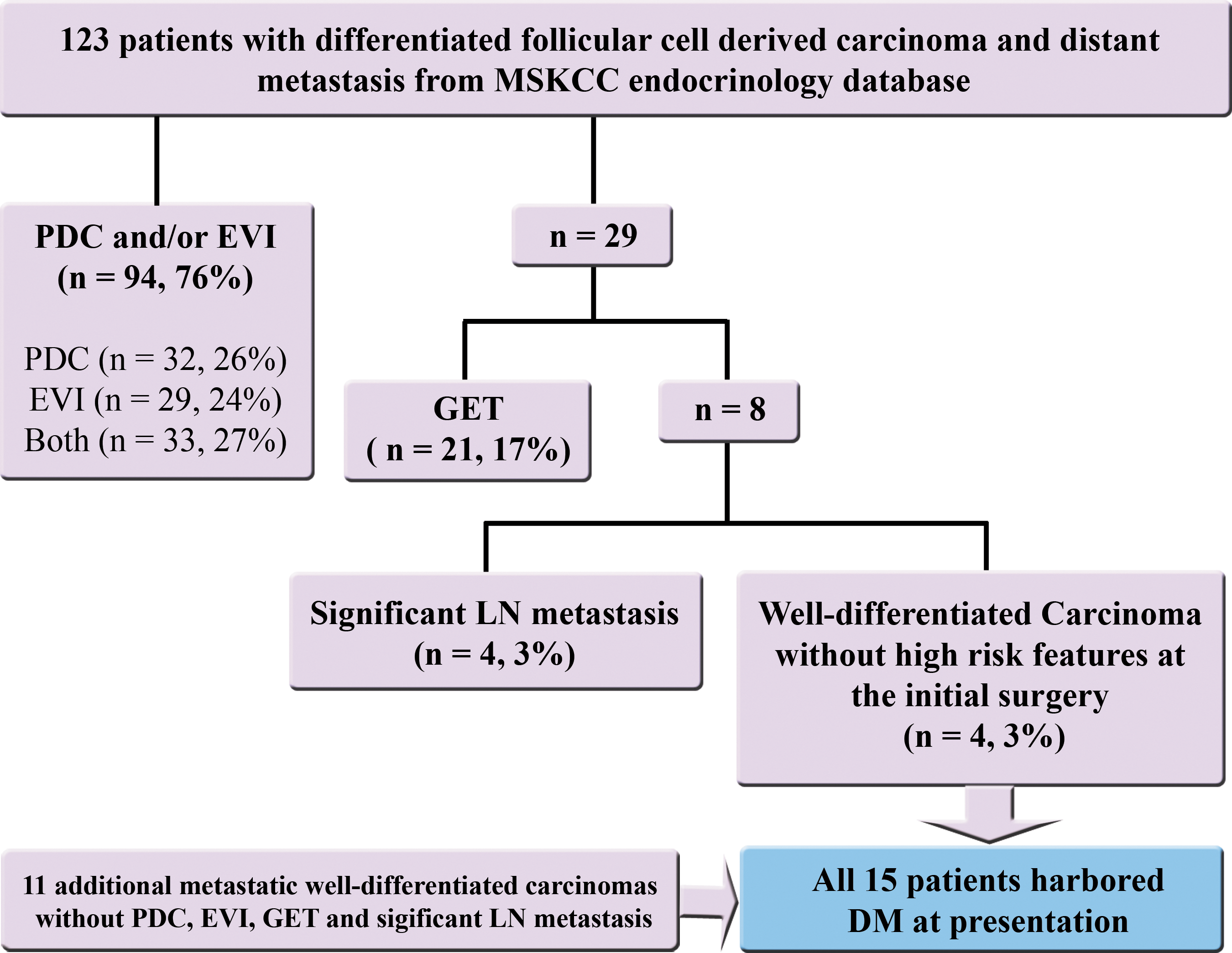
Workflow, methodology, and characteristics of the study cohort, which encompassed 123 patients with differentiated follicular cell–derived carcinoma and distant metastasis (either at clinical presentation or developed during follow-up). PDC, poorly differentiated carcinoma; EVI, extensive vascular invasion; GET, gross extension beyond the thyroid; LN, lymph node; DM, distant metastasis.
Clinicopathologic characteristics
The clinicopathologic features of these 15 well-differentiated primary thyroid carcinomas without high-risk features and with DM at presentation are summarized in Tables 1 and 2. These tumors occurred in older patients (median age of presentation = 63 years; range 50–75 years). There was a female predominance, with a female to male ratio of 2.75:1. In regard to sampling, a median of 2.2 blocks/cm of tumor was examined (range 1–5 blocks/cm of tumor). A median of 14 slides per thyroidectomy specimen was examined (range 3–43 slides). The majority (n = 8) of these tumors were encapsulated follicular variant of PTC with invasion (EFVPTC), while the remaining patients were diagnosed as infiltrative follicular variant of PTC (IFVPTC; n = 2), papillary microcarcinoma infiltrative follicular variant (n = 1), encapsulated PTC classical variant (n = 1), encapsulated FTC (n = 1), and encapsulated HCC (n = 2). Most of the patients had small tumors ≤2 cm in size (AJCC pT1, n = 10) without lymphovascular invasion (n = 12). All 15 cases had negative surgical margins and exhibited no evidence of microscopic ETE. Twelve tumors were encapsulated, while the remaining three were partially encapsulated or lacked a capsule completely. All 12 completely encapsulated carcinomas exhibited capsular invasion, either focal (n = 9) or extensive (n = 3), with foci ranging from one to seven per case. Ten of the 12 encapsulated carcinomas displayed capsular invasion only without vascular invasion. The number of foci of vascular invasion was as follows: absent in 10 cases, one focus in one patient, and two foci in another. One case displayed fewer than four foci at the initial routine diagnostic evaluation, but the exact number of foci could not be counted, since the slides were sent back to the original institution at the time of the study (Table 2). There were three tumors with only one focus of capsular invasion, no vascular invasion, and DM. The only patient who had nodal metastasis at the initial operation harbored a completely encapsulated classical variant of PTC that contained approximately 28% of tall cells and 7% of columnar cells. Intra-tumoral fibrosis and calcification were not assessable in two patients whose slides were sent back to their original institution at the time of the study. Among the 13 tumors with assessable intra-tumoral fibrosis and calcification, 12 had extensive intra-tumoral fibrosis, and 10 showed calcifications (Fig. 2). Six of the 15 cases had multicentric thyroid carcinomas harboring one or more foci of tumor in the form of papillary microcarcinomas in addition to the index lesion. All cases had histologically confirmed DM. Four of the 15 cases had mild mitotic activity (<5 mitosis per 10 HPFs; 400). No mitosis was found in the remainder.
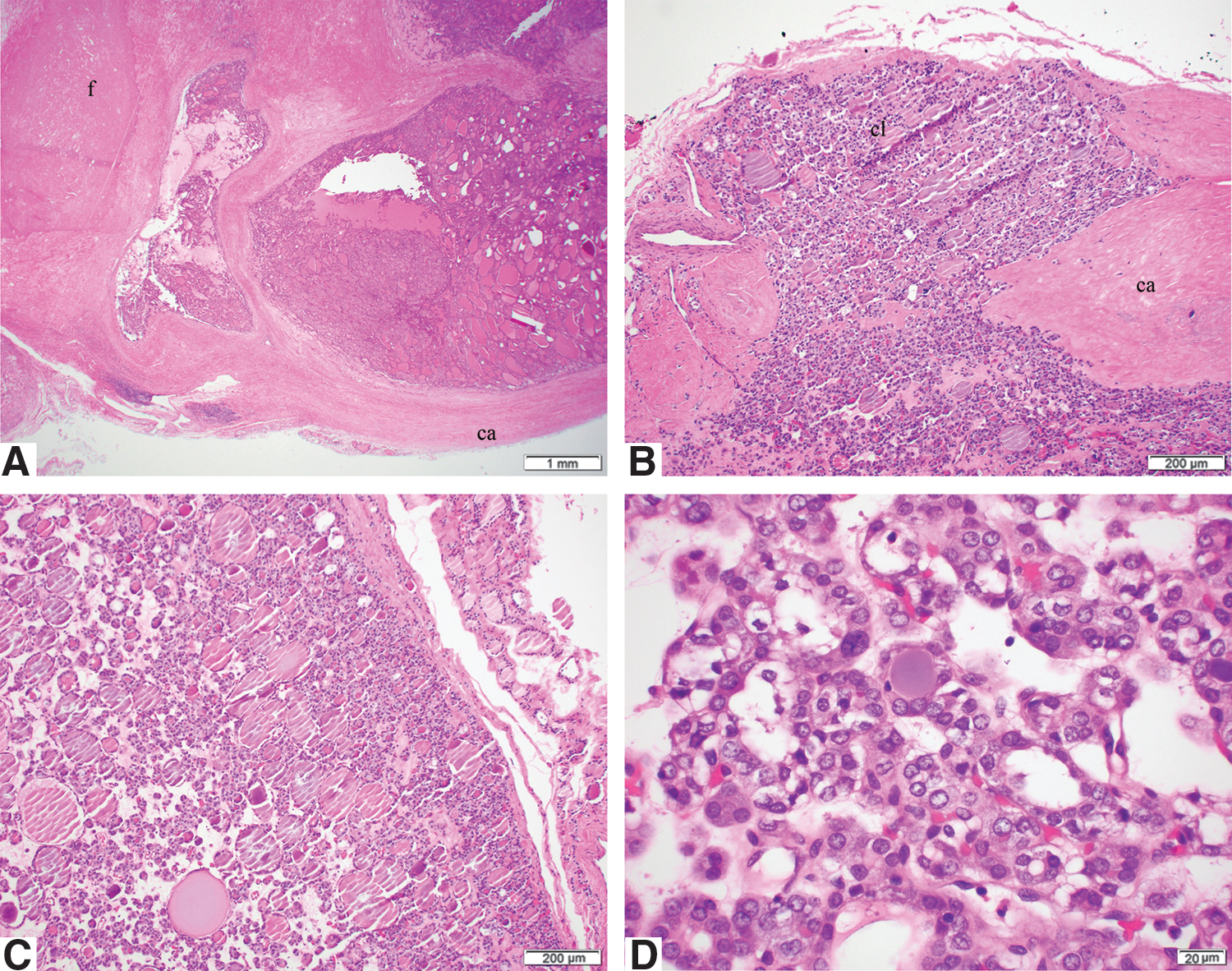
Microscopic pictures of encapsulated papillary thyroid carcinoma follicular variant with capsular invasion only and distant metastasis at presentation. (
AJCC, American Joint Committee on Cancer; PTC, papillary thyroid carcinoma; HCC, Hürthle cell carcinoma; FTC, follicular carcinoma.
Capsular invasion was not assessable, since tumor lacked a complete capsule.
Tumor size was the greatest diameter of the largest carcinoma focus.
AWD, alive with disease; CI, capsular invasion; DM, distant metastasis; DOD, dead of disease; DOUC, dead of unknown cause; EFC, encapsulated follicular carcinoma; EFVPTC, encapsulated follicular variant of papillary thyroid carcinoma; F, female; FTC, follicular thyroid carcinoma; HCC, Hürthle cell carcinoma; IFVPTC, infiltrative follicular variant of papillary thyroid carcinoma; M, male; NA, not applicable/not available; Pt, patient; PTC, papillary thyroid carcinoma; VI, vascular invasion.
The median follow-up for these 15 cases was 32 months (range 2–158 months). Four cases had a documented fatal outcome: two from unknown causes, and two from metastatic thyroid carcinoma. The remaining 11 cases were alive with disease at the time of last follow-up. The DM were predominantly found in the bone (n = 12), while metastasis to other sites were relatively rare, including the lung (n = 3), chest wall (n = 2), liver (n = 2), brain (n = 1), kidney (n = 1), and pelvic and buttock soft tissue (n = 2; Table 2). The majority of patients (n = 11) sought clinical attention for symptoms related to DM (e.g., pain, pathological fractures, palpable mass, or cognitive dysfunction). Four patients were asymptomatic and presented with lesions in the bone or lung noted on radiological studies performed for unrelated reasons. Four of the 11 symptomatic patients and none of the four asymptomatic patients were deceased at the last follow-up. Nine of the 15 patients did not have interpretable postoperative serum Tg levels because of high or unavailable serum TSH (n = 4), high antithyroglobulin antibodies (n = 1), or simply because the serum Tg assay was not performed (n = 4). The six cases with assessable post-thyroidectomy serum Tg had low postoperative (i.e., <5 ng/mL) Tg values (1.4 and 4.9 ng/mL), as well as high ones (49, 2058, 6303, and 7570 ng/mL). Preoperative serum Tg values were available in five cases and were elevated (78, 79, 640, 9300, and 14,675 ng/mL). Out of the four cases discovered incidentally, the postoperative serum Tg was low in one patient (1.4 ng/mL), high in another (6303 ng/mL), while in the remaining two, it was not available or uninterpretable.
Molecular characteristics
Targeted next-generation sequencing was performed on eight tumors, including five EFVPTC, one IFVPTC, one PTC classical variant, and one HCC, and the results are summarized in Table 3. The median mutation burden was 3 (range 1–7), with 6/8 tumors having two or more mutations. RAS mutations were the main driver in this cohort, affecting 5/8 tumors tested, including four EFVPTC and one IFVPTC. Only one tumor, a classical variant of PTC, harbored a BRAFV600E mutation. A RET/PTC rearrangement was not detected in this cohort. The two tumors that did not contain RAS or BRAF mutations were one EFVPTC and one HCC. Telomere reverse transcriptase (TERT) promoter mutations occurred at a high frequency (6/8) in this cohort. TERT promoter mutations co-occurred with either BRAF or RAS mutations in 4/6 tumors. A EIF1AX mutation was detected in one NRAS-mutated EFVPTC. Other mutations included NTRK1, PIK3CA, ARID2, ATM, CDKN1A, FAT1, RBM10, BAP1, INHA, PTPRS, PTPRT, and BCL6.
Discussion
DM are an infrequent occurrence in non-ANA FCDC, with a reported frequency of 1.2–13% (2 –8). As patients with DM carry a significant risk of death, with a five-year overall survival of 50–84% (4,5,9 –11) and a five-year disease-specific survival of 58–80% (3,5,6,11), it is of paramount importance to identify tumors at risk of developing DM at the time of initial presentation to assist clinical decision making.
Some published studies have suggested that the frequency of DM was different among the various histologic types, with HCC having the highest frequency, PTC the lowest, and FTC in between (7,8,19). Sugino et al. reported older age and larger tumor size as risk factors for DM in a cohort of 123 patients with FTC (20). In their study, the presence of vascular invasion was not associated with an increased risk of developing DM during follow-up. However, these authors did not evaluate the extent of vascular invasion. Recently, it has been shown that the vast majority of patients who die of non-ANA FCDC have aggressive histologic features in their primary tumors (15). A majority of these fatal carcinomas were associated with DM, which were the immediate cause of death in most fatal cases (13 –15). Similarly, in the current series, the overwhelming majority of patients with DM had in their primary tumors at least a poorly differentiated component, gross ETE, EVI, and/or a significant volume of lymph node metastases (e.g., more than five positive lymph nodes and/or one positive node >1 cm in greatest dimension). Together, these results suggest that such histologic features are useful tools to identify tumors at risk of developing distant disease and cancer-specific death. Hence, it is crucial to evaluate and report these parameters at presentation and take them into consideration for risk assessment and treatment planning of non-anaplastic thyroid carcinoma.
As shown in this study, primary tumors with low-risk histology (i.e., lacking the above aggressive features) also can give rise to DM. However, this is a rare cause of distant disease, since it was present in only 3% of the database of patients with DM.
A large proportion (12/15) of these apparently indolent primary tumors were encapsulated carcinomas, including eight encapsulated follicular variant of papillary carcinoma, two encapsulated HCCs, one encapsulated classical PTC, and one encapsulated FTC. Except for the encapsulated classical PTC case, none of the remaining 11 patients developed lymph node metastases. This is expected for the HCC and FTC, as these tumors have the tendency to develop distant rather than regional metastases (21). In regard to encapsulated FVPTC, previous studies have shown a molecular profile and clinical behavior similar to that of follicular adenoma or FTC (22,23). Genotypically, EFVPTCs harbor a high frequency of RAS mutations (36%) and a lack of BRAF mutations (0%) (23). Clinically, encapsulated FVPTCs with invasion, especially those with EVI, tend to give rise to distant rather than locoregional lymph node metastases (22). Consistent with these previous publications, the present study found that the RAS mutation occurred at high frequency (5/8), and was the main driver mutation in this cohort of low-risk well-differentiated thyroid carcinoma with DM. The BRAF mutation, on the other hand, was a rare event, affecting the only person with a classical variant PTC. The present study provides further evidence of the molecular similarity of EFVPTC with invasion to FTC and the potential capacity and propensity of DM in these tumors.
An intriguing finding was the presence of marked intra-tumoral fibrosis in a very high percentage of these cases. PTCs with intra-tumoral nodular fibrosis and heterotopic ossification were shown to have higher incidences of lymph node metastasis and extrathyroidal invasion than those without these features (24). In that study, higher expression of basic fibroblast growth factor (bFGF), bone morphogenetic protein-2 (BMP-2), and vascular endothelial growth factor (VEGF) was found in PTC with nodular fibrosis. Neovascularization was also increased in tumors with nodular fibrosis. The authors, however, did not study the impact of fibrosis on distant disease. Of note, marked intra-tumoral fibrosis and/or heterotopic ossification were detected in two of three previously reported papillary microcarcinomas that developed DM and caused death (25). It is tempting to speculate that fibrosis in these tumors is indeed a regressive change, and similar to melanoma, regression may lead to under-staging/under-grading of the tumor. Further work is needed to understand the mechanisms leading to marked tumor fibrosis in patients with DM and indolent histology.
A more perplex finding is the absence of vascular invasion in most cases (12/15), including 8/10 encapsulated tumors. Since encapsulated low-grade thyroid carcinomas with capsular invasion are known almost never to behave aggressively (26), it is nearly impossible for the pathologists to predict distant spread based on histology alone in these unusual cases.
TERT promoter mutation is an uncommon molecular event in PTC, being reported in 9% of 496 PTCs in The Cancer Genomic Atlas study (27). On the other hand, TERT promoter mutation occurs at a high frequency in PDC and anaplastic thyroid carcinoma, with 40% and 73%, respectively (28,29). In PTC, TERT promoter mutations have been shown to be a molecular signature associated with aggressive clinical behaviors (e.g., propensity for regional and DM and disease-specific death) (30,31). Compared with the 9% mutation rate in PTC in general, TERT promoter mutation was highly prevalent (6/8) in this cohort of differentiated carcinoma with low-risk tumor morphology but DM. In four cases, TERT promoter mutations were associated with RAS or BRAF mutations. The co-existence of these two events has been shown to correlate with high risk of recurrence and to increase disease-specific mortality in differentiated thyroid carcinomas (29). The above TERT-related findings may explain the aggressive behavior of these tumors. Importantly, it suggests that TERT can be used as a molecular marker indicative of aggressive clinical behavior in these histologically indolent primary tumors.
Mutation in the eukaryotic translation initiation factor 1A X-linked (EIF1AX) has been reported to co-occur with RAS mutation in well-differentiated, PDC, and anaplastic thyroid carcinoma, and it is an adverse molecular signature in PDC (28,32,33). Consistent with such findings, co-existence of NRAS and EIF1AX was detected in one EFVPTC with DM at presentation in the present cohort. One of the cases in the study showed mutation of CDKN1A, which is a tumor suppressor gene encoding p21. Interestingly, higher expression of p21 was found to be associated with high-risk clinical features in PTC (34). Other notable alterations were those of ARID2, a member of the SWI/SNF remodeling complex, and ATM, a tumor suppressor gene. Both of these genes have been found to be mutated in PDC and anaplastic carcinomas (31). Most of the remaining somatic mutations found such as RBM10, FAT1, BAP1, BCL6, PTPRT, PTPRS, and INHA were seen in only one case and have not been reported in thyroid carcinomas.
From a practical point of view, the important question centers on how to identify aggressive behavior in these histologically indolent primary tumors. In the vast majority of cases (11/15), the clinician was able to diagnose distant disease based on the patient clinical presentation (e.g., bone fracture). There were, however, four cases where DM were detected incidentally by imaging ordered for non-thyroid diseases. In one of those patients, the endocrinologist would have suspected metastatic disease based on a high postoperative serum Tg (6303 ng/mL) had the patient being subjected to surgery before the discovery of distant disease. There was, however, another incidental case where the postoperative serum Tg was low (1.4 ng/mL). The aggressive behavior of this patient's tumor would in theory have been unrecognized by the clinician and pathologist based on the histology and Tg level. Three of these four incidental cases had tissue for genotyping. Interestingly, TERT promoter mutations were found in each of the genotyped cases and were associated with a RAS mutation in one individual, mutation in PIK3CA in another, and BRAFV600E in the patient with low postoperative serum Tg. The detection of TERT mutations seems to have the potential of unmasking the aggressive potential of these low-grade tumors.
In conclusion, this study demonstrates the power of meticulous, clinical, operative, and routine histopathologic examination in stratifying differentiated thyroid carcinomas. One can recognize patients with non-ANA FCDC at risk of DM based on the presence of the following four clinicopathologic features in the primary resection: GET, EVI, a histologic diagnosis of PDC, and significant lymph node metastasis involving more than five lymph nodes and at least one >1 cm in greatest dimension. Non-ANA FCDCs without these four clinicopathologic features very rarely develop DM. If DM does occur in such lesions, it is commonly present at the time of the initial clinical evaluation. In the vast majority of cases, the clinical presentation will uncover the DM associated with these indolent-appearing primary tumors. These tumors are enriched in RAS-mutated FVPTC and harbor a very high rate of TERT promoter mutations. The latter genetic alteration may help identify aggressive behavior in patients with these histologically low-risk primaries, including those extremely infrequent cases with asymptomatic DM.
Footnotes
Acknowledgments
The research reported in this publication was supported in part by the Cancer Center Support Grant of the National Institutes of Health/National Cancer Institute under award number P30CA008748. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist for all contributory authors.