
Abstract
Background:
Differentiated thyroid cancer (DTC) has a good prognosis but a remaining risk of recurrence, and life-long follow-up as well as medication with levothyroxine may be necessary. The aim of this study was to clarify how thyroid-related symptoms affect health-related quality of life (HRQoL) 14–17 years after diagnosis in Swedish DTC patients.
Methods:
From the all-encompassing population-based Swedish Cancer Registry, 353 patients diagnosed with DTC during 1995–1998 were identified and invited to answer a study-specific questionnaire and the HRQoL questionnaire SF-36 14–17 years after their diagnosis. Subgroups were studied according to thyroid-related symptoms, both symptoms correlated to thyroid disease or levothyroxine treatment and side effects from surgery and radioiodine treatment.
Results:
Of the patients with DTC, 279 (79%) answered the questionnaires. In all, only 19 (7%) reported a recurrence. Patients with one single symptom (e.g., fatigue, sleeping disorders, irritability, lower stress resistance, muscle weakness, bodily restlessness, sweating, palpitations, or flushes) had significantly lower HRQoL measured with the SF-36 compared to those without that specific symptom (p < 0.001). Furthermore, those 238 patients with at least one symptom, regardless of which one, had significantly lower HRQoL in all eight SF-36 domains compared to patients that no thyroid symptom (n = 34; p < 0.001). In seven patients, the questionnaires were not complete in terms of the thyroid-related questions. The association between thyroid symptoms and lower HRQoL remained after adjusting for age, sex, comorbidities, education, and menopause.
Conclusions:
DTC patients reporting thyroid symptoms scored lower in HRQoL compared to those with no symptoms >14 years after diagnosis.
Introduction
D
Due to the usually good prognosis and rising prevalence of DTC (8), the importance of health-related quality of life (HRQoL) is increasing. Despite the longevity of DTC patients, HRQoL has been shown to be lower compared to the general population (9 –11) and even as low as in other cancer patients with more aggressive malignancies (12). Because TSH suppression can be associated with cardiovascular side effects, symptoms from hyperthyroidism could also be expected in thyroid cancer survivors. Some studies have demonstrated thyroid symptoms that could be related to TSH suppression, for example fatigue, insomnia, flushes, and anxiety. These symptoms are also correlated to decreased HRQoL (10,13,14). Nevertheless, TSH suppression in itself is not unambiguously associated with lower HRQoL (15).
Although HRQoL is improving over time, it is still lower compared to a general population years after diagnosis (15,16). Fear of recurrence, comorbidities, and a negative view on life all impact HRQoL (9). However, the relationship between side effects from treatment and HRQoL has been sparsely described.
The aim of this nationwide, population-based cohort study in Sweden was to describe thyroid-related symptoms and patient-related characteristics in relation to long-term HRQoL 14–17 years after a diagnosis of thyroid cancer.
Materials and Methods
Study design and population
A population-based, nationwide, cross-sectional cohort study was performed in June 2012 in Sweden. All patients diagnosed with DTC between 1995 and 1998 were identified from the all-encompassing Swedish Cancer Registry. The Swedish Cancer Registry includes all patients with a cancer diagnosis and is considered to be of good quality, with a national coverage of >96% (17). Thus, patients included were 35–64 years of age at inclusion in 2012, corresponding to 18–50 years at diagnosis. Younger patients would have been children at the time of diagnosis, and older patients might have had heterogeneous confounding factors (18). Patients fulfilling the inclusion criteria were invited to participate by mail. By completing and returning questionnaires, patients consented to participate and agreed for their data to be used for research purposes. Up to two reminder letters were sent to non-responders. The study was approved by the Regional Ethical Review Board in Stockholm (2011/718-31/2 and 2011/1847-32).
Data collection
Socio-demographic variables and comorbidities
Participants were asked to provide information on their age in years, sex, level of education, and occupation/employment. Patients reported comorbidities diagnosed by a physician, and the following diagnoses were registered: previous myocardial infarction, hypertension, atrial fibrillation, previous stroke, diabetes, chronic obstructive pulmonary disease, asthma, kidney failure, rheumatoid arthritis/osteoarthritis, osteoporosis, depression under treatment or other psychiatric disease, cancer, or any other specified disease. Comorbidities were subsequently grouped into “none,” “one,” or “at least two.”
Cancer-related variables
Patients reported their primary treatment in different preset categories, namely: none, total thyroidectomy, hemithyroidectomy with or without cervical lymph node dissection uni- or bilateral, radioiodine treatment, and external radiotherapy. When appropriate, the patients reported whether they had a locoregional recurrence or distant metastases (yes/no), and if yes, which treatment was given from a preset list.
Thyroid-related symptoms
At the time of initiation of the study, there were no relevant questionnaires validated in Swedish. Therefore, a study-specific questionnaire was developed based on items regarding symptoms relevant for thyroid cancer patients based on existing questionnaires available in English but not in Swedish.
The term “thyroid-related symptoms” was used to cover both symptoms that probably are related to thyroid disease or levothyroxine treatment and side effects from surgery and/or radioiodine treatment. The specified symptoms related to thyroid disease or levothyroxine treatment were: fatigue, sleeping disorders, irritability, lower stress resistance, muscle weakness, bodily restlessness, sweating, palpitations, and flushes. The following symptoms with a probable relation to thyroid cancer treatment were also registered: xerostomia, hoarseness, dysphagia, numbness in the operation area, salivary gland problems, and other symptoms. The severity of the symptoms probably related to thyroid disease or levothyroxine treatment was scored on a five-point response scale ranging from 1 = “not at all” to 5 = “very much.” Treatment-related symptoms were scored on a three-point response scale ranging from 1 = “not at all” to 3 = “disturbing.”
HRQoL
HRQoL was assessed with the Swedish version of the SF-36 (19,20), v2.0, a well-validated HRQoL questionnaire used in many international publications (21). The SF-36 is a multipurpose, short-form survey with 36 questions regarding physical and mental health. Many years after their diagnosis, thyroid cancer patients are not expected to have symptoms suitable to measure with a cancer-specific questionnaire. Therefore, the SF-36, a general HRQoL questionnaire, was chosen. All patients were Swedish-speaking, and thus the Swedish version of the SF-36 was used. The SF-36 is provided in two versions with different recall periods (one and four weeks, respectively). The four-week version was used, since symptoms over time were evaluated. Responses were linearly transformed to a score between 0 and 100 according to the SF-36 manual (22) on each of the eight domains: physical functioning (PF; e.g., “Does your health now limit you walking more than a mile?”); physical role functioning (RP; e.g. “Have you accomplished less than you would like as a result of your physical health?”); bodily pain (BP; e.g., “How much bodily pain have you had during the past four weeks?”); general health (GH; e.g., “My health is excellent”); vitality (VT; e.g., “Did you have a lot of energy?)”; social functioning (SF; e.g., “During the past four weeks, to what extent has your physical health or emotional problems interfered with your normal social activities?”); emotional role functioning (RE; e.g., “Have you accomplished less than you would like as a result of any emotional problems?”); and mental health (MH; e.g., “Have you felt downhearted or blue?”). A higher score signifies a better HRQoL. The SF-36 questionnaire was distributed first in the mailed questionnaires.
Statistical analyses
Patient characteristics were described by standard descriptive statistics (Table 1). In regard to thyroid-related symptoms, the patients completed a questionnaire with five verbal alternatives (Likert scale). For the analysis, the results were divided into three groups: “no symptoms,” “moderate symptoms” (including “a little” and “moderate”), and “major symptoms” (including “quite a bit” and “very much”).
Patients were aged 35–64 years (M = 51 years).
HRQoL, health-related quality of life; DTC, differentiated thyroid carcinoma.
In a comparison of all domains on the SF-36, a difference of 5–10 points (scale 0–100) between groups was interpreted as a clinically relevant, minimally important difference (MID) (23). A difference of 10–20 points corresponded to a moderate difference, and >20 points corresponded to a considerable difference (23). Statistical significance was tested using the Mann–Whitney U-test or Kruskal–Wallis test at the 0.050 level. When evaluating HRQoL data, statistical significance alone is not sufficient. Therefore, MID was used as a supplement. The MID is defined as the smallest difference in score that patients consider to be important (24).
To safeguard the statistics further, the responses to the SF-36 domains were also dichotomized into “good” versus “poor” in order to assess a correlation between thyroid-related symptoms and HRQoL. Adjustments were made for age, sex, comorbidities, education, and menopause. Patients answering “no” or “little” symptoms/impact on HRQoL on all questions in one domain were categorized as having good HRQoL. Otherwise, they were categorized as having poor HRQoL. Logistic regression models were used to assess associations in the form of odds ratios (ORs) with confidence intervals (Cis) between good and poor HRQoL levels.
The time period was set to four years (1995–1998) in order to gather a sufficient number of patients for power calculation. Missing responses in both the SF-36 and the study-specific questionnaire were handled according to the SF-36 manual scoring software (half-scale rule). The statistical software Stata v12.1 (Stata Corp., College Station, TX) was used for all analyses.
Results
Patient characteristics
Of 353 eligible individuals, 279 (79%) answered the questionnaires. Eleven (3%) patients returned unanswered questionnaires, and two envelopes were returned undelivered. The majority (78%) of patients were women. The mean age was 51 years (range 35–64 years), and the follow-up time was 14–17 years according to the inclusion criteria. The majority (85%) had at least 10 years of education. Half of the patients reported one or more comorbidities. The median body mass index was 26 kg/m2 for men and 24 kg/m2 for women; half of the women were pre-menopausal. All patients reported surgery as their primary treatment, 105 (38%) mentioned that they had received radioiodine treatment, and five (2%) stated receiving external radiotherapy. Only a few (n = 19; 7%) stated any kind of recurrence (Table 1).
There was no statistical difference between responders and non-responders regarding age and sex.
Thyroid-related symptoms
Thyroid-related symptoms such as fatigue, sleeping disorders, irritability, lower stress resistance, muscle weakness, bodily restlessness, sweating, palpitations, flushes, xerostomia, hoarseness, dysphagia, numbness in the operation area, and salivary gland problems were reported by the majority (88%; n = 238/272) of patients. In seven patients, the questionnaires were not complete in terms of thyroid-related symptoms. Almost half (42%) reported major symptoms, and 46% reported moderate symptoms. All patients with major thyroid symptoms had significantly lower HRQoL in all SF-36 domains compared to patients without these symptoms (p < 0.001). The difference between HRQoL in patients with moderate thyroid symptoms compared to patients with no symptoms was statistically significant in seven of eight domains (p < 0.001–0.02; not in RE), and was also clinically significant in half of the domains (BP, VT, SF, and MH). The difference in SF-36 scores was >20 points in all comparisons between patients with major and no symptoms, corresponding to a clinically considerable difference, with the exception of PF, which had a difference of 19 points (Table 2).
Domains in bold corresponds to minimum of small clinically significant difference, i.e. ≥5 points.
Thyroid-related symptoms categorized as no, moderate, or major based on the following aspects: muscle weakness, fatigue, palpitations, bodily restlessness, sleeping disorders, sweating, flushes and lower stress resistance, xerostomia, hoarseness, dysphagia, numbness in the operation area, and salivary glands problems.
p-Value assessed with Kruskal–Wallis test.
Statistically significant difference between patients with moderate and no thyroid symptoms, p < 0.001–0.02, assessed with Mann–Whitney test (data not shown in the summary table above).
SD, standard deviation; SF-36, Short Form-36 Health Survey.
Symptoms related to thyroid disease or levothyroxine treatment
Between 35% and 77% of patients (depending on symptom) reported symptoms related to thyroid disease or levothyroxine treatment: fatigue, sleeping disorders, irritability, lower stress resistance, muscle weakness, bodily restlessness, sweating, palpitations, or flushes. Regarding each symptom separately, all patients with either moderate or major symptoms grouped together had significantly lower HRQoL compared to patients without that symptom (p < 0.001). All comparisons were also clinically significant with >10 points difference in all SF-36 scores. When comparing patients with no symptoms with major symptoms, the difference was >20 points, regarded as a considerable clinical difference, except for palpitations, sweating, and flushes (Table 3; p < 0.001).
HRQoL is compared between patients with (both moderate and major) and without thyroid-related symptoms. HRQoL is also compared between patients with no symptoms and patients with major thyroid-related symptoms.
For each symptom, the difference in SF-36 points (0–100) between patients without that specific symptom is compared to patients with moderate + major symptoms and with patients with only major symptoms. The lowest value for each symptom is the smallest difference between patients with and without that symptom regarding all eight SF-36 domains. The highest value is the greatest difference in the SF-36 domains between patients with and without symptoms. A difference of 5–10 points is regarded as a minimal clinical difference, 10–20 is moderate, and >20 is a considerable clinical difference.
Differences in SF-36 points printed in bold correspond to a minimum of small clinically significant differences, i.e. ≥5 points.
p-Value assessed with Mann–Whitney test. p-Values assessed both between no symptoms and major symptoms and between no symptoms and moderate + major symptoms. All p-values <0.001.
The most prevalent symptoms—fatigue, sleeping disorders, and irritability—affected more than half of the patients, and these symptoms had a large negative effect on HRQoL. Comparing patients with major and no symptoms, SF-36 scores differed by >20 points, corresponding to a clinically considerable difference (p < 0.001; Figs. 1 –3).
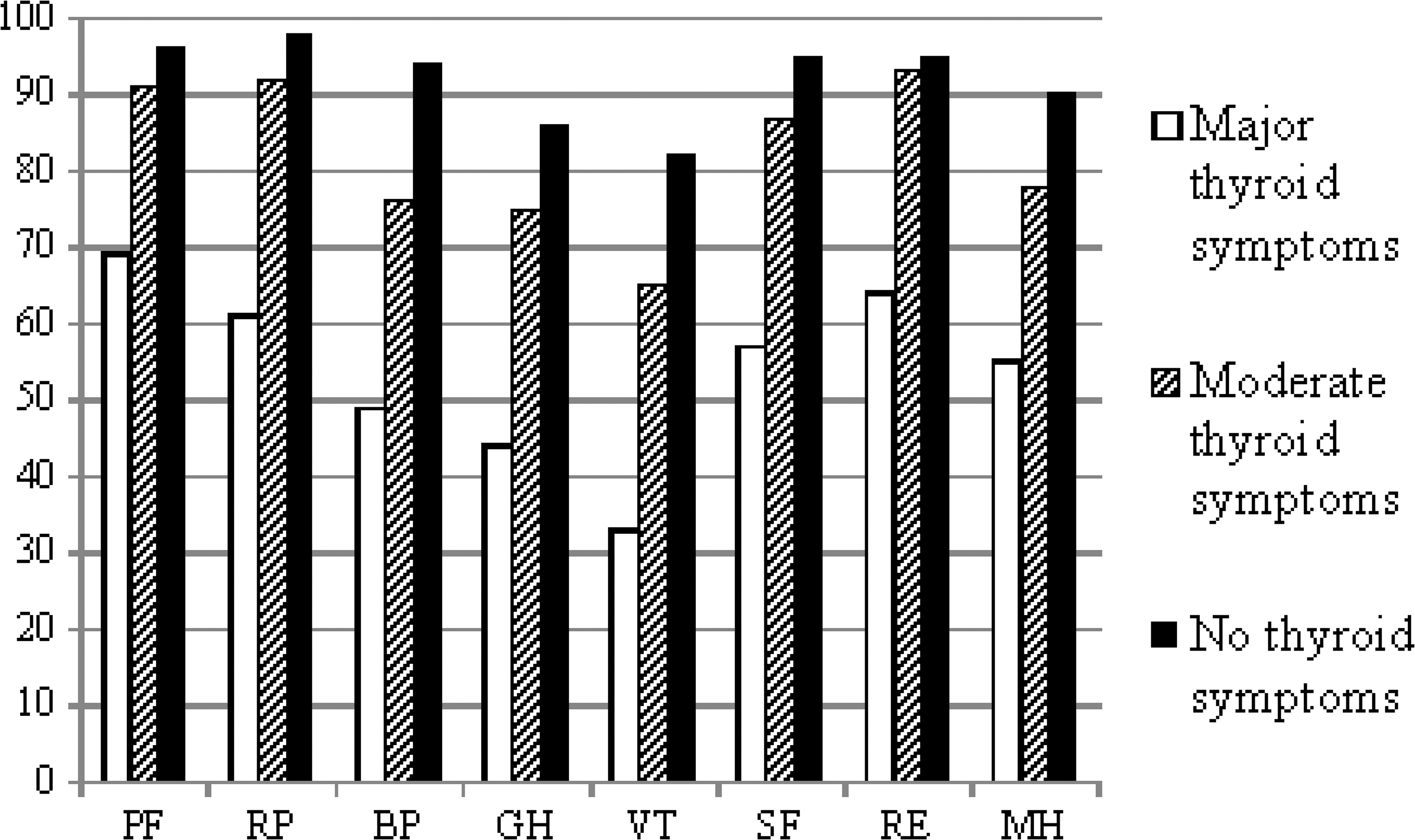
Differences in long-term HRQoL (i.e., 14–17 years after diagnosis) measured with the Short Form-36 Health Survey (SF-36; 0–100 points) in patients with differentiated thyroid cancer (DTC), analyzed on the three most prevalent thyroid-related symptoms. HRQoL in patients without fatigue is compared to HRQoL in patients with moderate and major symptoms of fatigue. HRQoL, health-related quality of life.
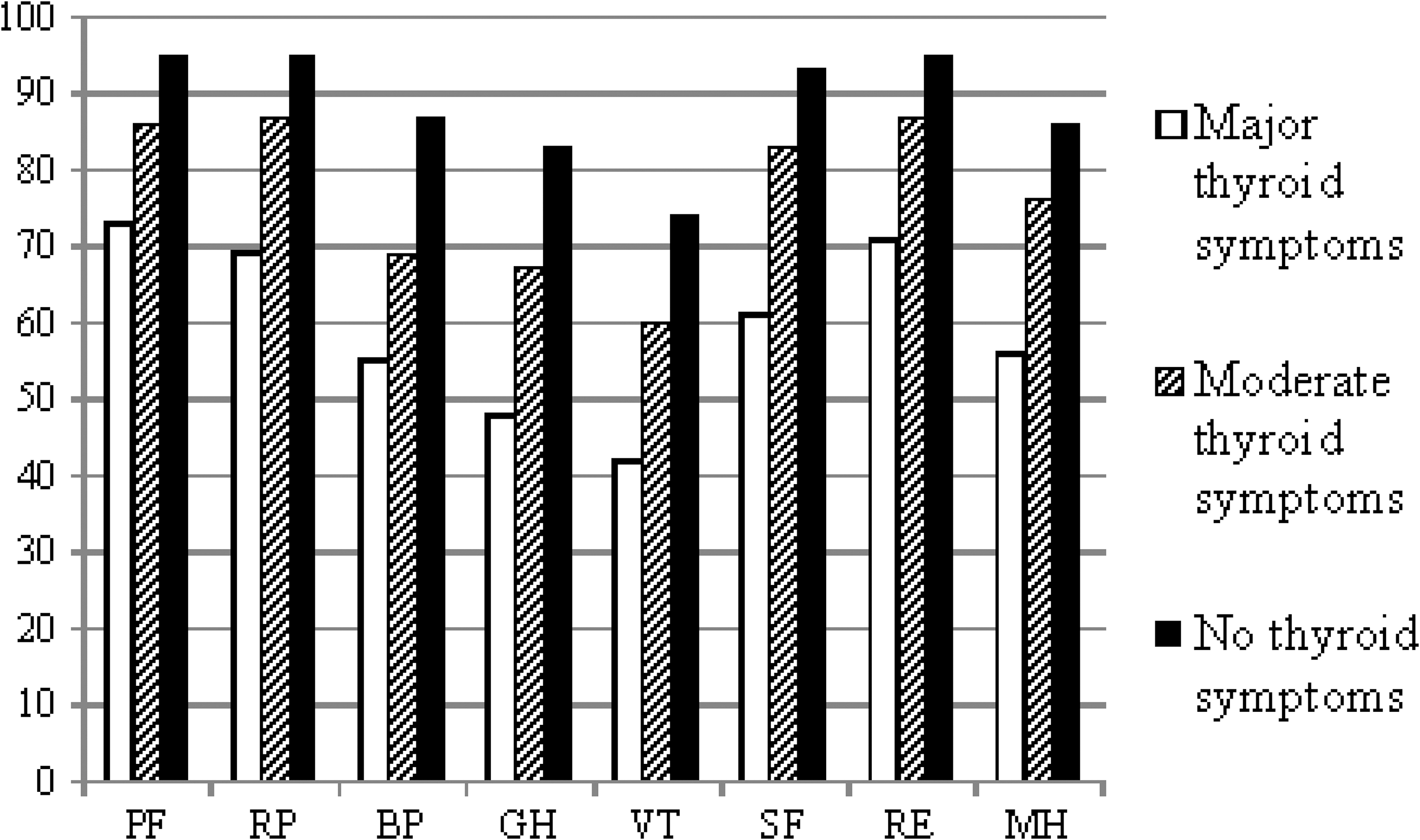
Differences in long-term HRQoL (i.e., 14–17 years after diagnosis) measured with the SF-36 (0–100 points) in patients with DTC, analyzed on the three most prevalent thyroid-related symptoms. HRQoL in patients without sleeping disorders is compared to HRQoL in patients with moderate and major symptoms of sleeping disorders.
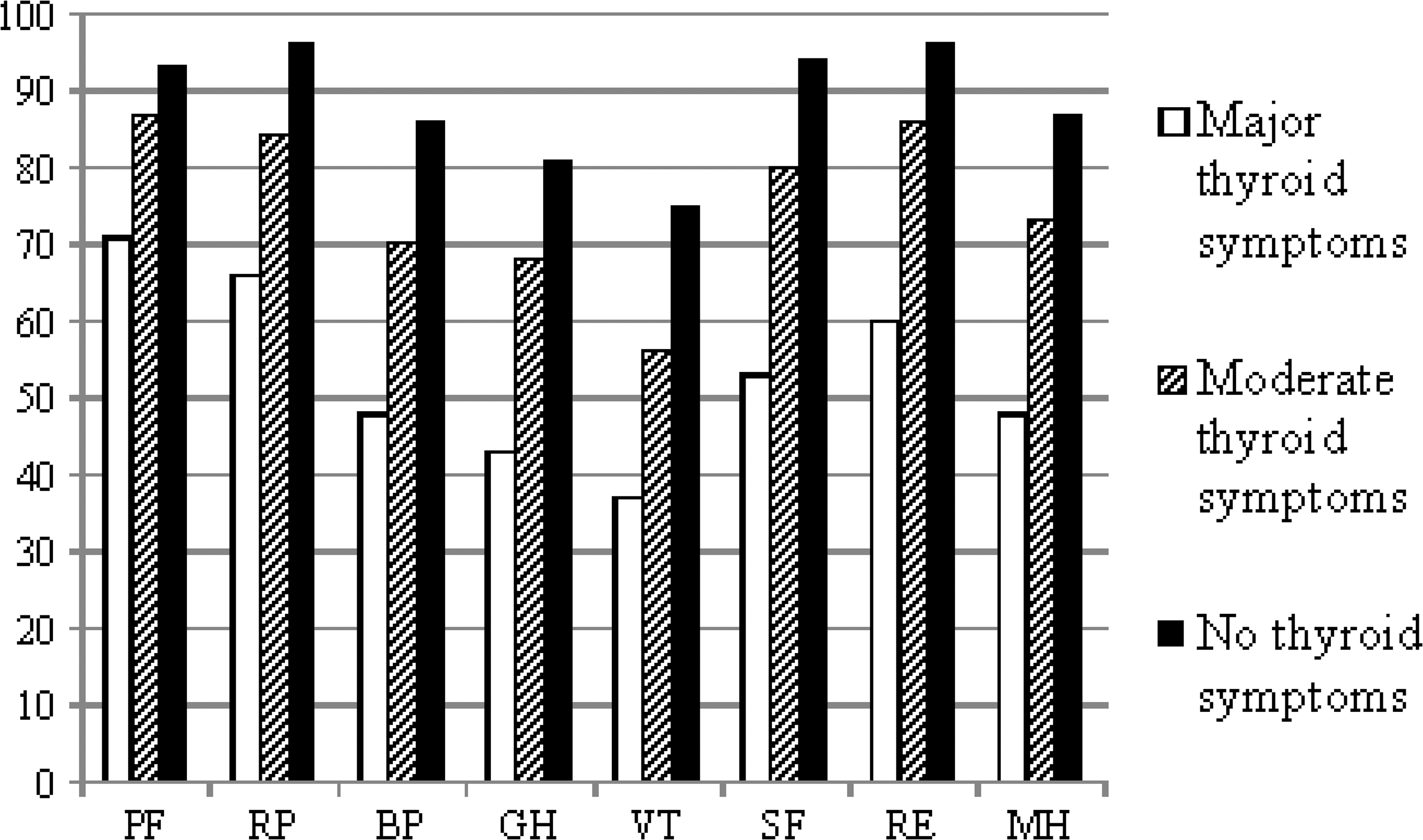
Differences in long-term HRQoL (i.e., 14–17 years after diagnosis) measured with the SF-36 (0–100 points) in patients with DTC, analyzed on the three most prevalent thyroid-related symptoms. HRQoL in patients without irritability is compared to HRQoL in patients with moderate and major symptoms of irritability.
Symptoms with a possible relation to surgery or radioiodine treatment
There were few patients with symptoms with a possible relation to surgery or radioiodine: xerostomia (16%; n = 44), hoarseness (13%; n = 35), dysphagia (10%; n = 28), numbness in the operation area (5%; n = 14), and salivary gland problems (4%; n = 10). All patients with major symptoms had statistically and clinically lower HRQoL on all eight SF-36 domains compared to patients with no symptoms (p < 0.001; data not shown).
Association between thyroid-related symptoms and patient characteristics
There was a significant association between comorbidities and thyroid
There was a clear correlation between thyroid-related symptoms and a decrease in HRQoL on all SF-36 domains. A statistically significant difference was demonstrated between patients with no thyroid related-symptoms and patients reporting major thyroid-related symptoms (p < 0.01). These differences remained after adjustment for age, sex, comorbidities, and education (Table 4) and for women after adjustment for menopause (data not shown).
Thyroid-related symptoms are divided into no, moderate, or major symptoms. Crude odds ratios are adjusted for age, sex, comorbidities, and education.
Multivariable model adjusted for age (in two groups: 35–49 and 50–65 years), sex, comorbidities (in three groups: 0, 1, or at least 2), and education (low vs. middle and high).
p < 0.05.
OR, odds ratio; CI, confidence interval. Domains: PF, physical functioning; RP, physical role functioning; BP, bodily pain; GH, general health; VT, vitality; SF, social function; RE, emotional role functioning; MH, mental health.
Discussion
This nationwide population-based cohort study shows that the vast majority of thyroid cancer patients still had thyroid-related symptoms negatively affecting their HRQoL 14–17 years after diagnosis. Several of the symptoms that could be related to thyroid hormone treatment affected more than half of the patients, while symptoms possibly related to surgery and radioiodine treatment were much less frequent.
According to recent international guidelines (2), less aggressive treatment of DTC, including lobectomy (25) and selective use of radioiodine, has been suggested to minimize the risk of side effects. An increasing number of the newly diagnosed tumors are low risk (26), and some data support that less aggressive treatment, including lobectomy, does not affect risk of recurrence or survival (2,25). Thus, thyroid cancer patients might suffer from lifelong side effects without obtaining benefit from their treatment. The significant number of symptoms affecting HRQoL identified in this study supports the concept of less aggressive treatment. According to international guidelines (2), the degree of TSH suppression should be adjusted according to risk of recurrence, and fewer patients on TSH suppression might decrease treatment-related symptoms, which could probably improve HRQoL.
While the incidence of thyroid cancer is steadily increasing worldwide, treatment-related side effects might become of greater importance. In the United States, thyroid cancer is the fifth leading cause of cancer in women, accounting for 6% of all cancers (27), and it is projected to be the third most common cancer in women in 2019 (8). Furthermore, in Sweden and the other Nordic countries, a rapid increase in thyroid cancer incidence has been observed in both men and women over the last 15 years (28). This increase in thyroid cancer survivors makes it extremely important to minimize treatment burden and side-effects.
Treatment-related side effects
Interestingly, symptoms related to treatment with radioiodine were rare in this study. Only 4% of patients reported salivary gland problems, and xerostomia was reported by 15%. In previous studies, salivary gland problems have been reported in 5–67% of patients, which is probably related to different time points of measurement and a lack of validated instruments (7). On the other hand, xerostomia is scarcely reported in the literature but has been described in 15% of patients more than three years after radioiodine treatment (29), which is in good agreement with the present findings. The low rate of salivary gland problems in this study could be related to the low incidence of reported recurrence; only 7% of the patients reported any kind of recurrence. Thus, only a few patients received high cumulative doses of radioiodine, which is known to increase the risk of sialoadenitis (30), as well as the risk of xerostomia (31).
Although several years had passed since diagnosis, many patients still had a substantial number of thyroid
Persisting symptoms might still be affected by unknown factors in thyroid hormone metabolism, but studies do not support the assumption that thyroid suppression, or lack of endogenous triiodothyronine, are conclusively able to explain decreased HRQoL in thyroid cancer patients (32).
Fatigue was the most prevalent symptom in this study, reported by >70% of patients. This is supported by previous studies, where fatigue seems to be a particularly important symptom in thyroid cancer survivors (35,36). Treatment of fatigue has been sparsely studied, but exercise seems to decrease post-treatment fatigue significantly in thyroid cancer patients (37) while restoration of TSH suppression does not (34). Sleeping disorders were frequent in this study, which is also supported by previous studies (38), where in addition to insomnia, sleep quality seems important to thyroid cancer patients (36).
According to the present results, patients had many symptoms that might have been related to treatment from their thyroid cancer, although many years had passed since diagnosis. This is partly in contrast to the fact that previous studies have shown increasing HRQoL over time. In one study, HRQoL was affected only after thyroid hormone withdrawal, and HRQoL returned to baseline at eight months of follow-up (39). During long-term follow-up, HRQoL was lower compared to a control group at the beginning of the study, but at five years of follow-up, the two groups were comparable (40). In other studies, however, HRQoL remained lower during follow-up (41). A possible reason for an increase in HRQoL over time in thyroid cancer survivors is the response shift, which allows the patients to adapt to their illness (42). However, fear of a recurrence and worries about employment can negatively affect HRQoL many years after a diagnosis of cancer (9,36,43).
Methodological aspects
The strengths of this study are the population-based approach, which included all thyroid cancer patients in Sweden diagnosed between 1995 and 1998, and the positive attitude to participate, which gave a high response rate. This provides valuable information about self-reported symptomatology many years after the diagnosis of thyroid cancer in a whole population. Furthermore, as a measure of HRQoL, the SF-36 is a well-validated questionnaire that has been shown to be sensitive when measuring HRQoL in thyroid cancer patients (39). All the data in this study—symptoms, treatment, and recurrences—were self-reported. Since the main outcome was long-term HRQoL, this method was considered to be adequate, although there might have been limitations to treatment-related details, for example. Furthermore, the SF-36 as a general HRQoL questionnaire might not capture all the different perspectives in DTC patients. Although the study-specific questionnaire that we used is not validated, it is a reasonable complement to the SF-36. No validated disease-specific Swedish HRQoL questionnaires for thyroid cancer patients were available at the time of data collection.
Conclusions
Although DTC patients have an excellent prognosis, many of them still have a substantial amount of symptoms affecting their HRQoL negatively >14 years after diagnosis. These data might support the ongoing discussion about treating at least low-risk DTC patients less aggressively.
Footnotes
Acknowledgments
This work was supported by grants from The Cancer Research Foundations of Radiumhemmet; Serafimerlasarettet Foundation; Capio research Foundation; and Foundation Stiftelsen för Kirurgiskt samarbete. The manuscript was proofread by David Boniface. Statistical support was received from Johan Bring. This study was presented as an abstract at the 15th International Thyroid Congress (ITC), Orlando, FL, 2015.
Author Disclosure Statement
No competing financial interests exist.