
Abstract
Background:
Papillary thyroid cancer (PTC) is a common malignancy diagnosed during pregnancy. However, there is little information on the behavior of PTC during pregnancy. The aim of this study was to evaluate the natural course of PTC in pregnant women.
Methods:
The study included 19 patients with PTC who delayed thyroid surgery because they were diagnosed with PTC just before or during the early stages of pregnancy. Serial neck ultrasonography (US) was used to evaluate PTCs before surgical treatment and the clinical outcomes after surgery.
Results:
The median maximal PTC size at initial diagnosis on US was 0.91 cm (interquartile range [IQR] 0.61–1.11), and 13/19 (68.4%) patients had micro-PTCs (≤1 cm). The median maximal PTC size after a median 9.5 months of follow-up was 0.98 cm (IQR 0.72–1.12). There were three (16%) patients who showed a size increase, and five (26%) patients showed a volume increase during the follow-up periods. There was no clinically relevant change in the maximal tumor size during the follow-up period (p = 0.16). Serial US measurements of PTC size in seven available patients in each trimester showed no significant differences between the different trimesters (first vs. second trimester p = 0.81; second vs. third trimester p = 0.99). No newly developed lesions in the thyroid or cervical lymph nodes were detected by neck US during the follow-up period. Among 19 patients, 16 underwent thyroid surgery after delivery, and the median duration from diagnosis to surgery was 11.9 months.
Conclusions:
No clinically relevant changes associated with a progression of PTC were observed during pregnancy. Delayed thyroid surgery with active surveillance can be an appropriate approach for pregnant patients with PTC.
Introduction
P
According to the recent American Thyroid Association (ATA) guidelines, when a patient is diagnosed as DTC during pregnancy and the disease remains stable by mid-gestation, surgery may be deferred until after delivery (9). However, this is a weak recommendation based on low-quality evidence from studies suggesting that delayed thyroid surgery does not affect the outcome of DTC (10 –12). The first study evaluating the impact of pregnancy on tumor growth in PTC was conducted by Shindo et al. (13). This study enrolled nine patients with micro-PTCs (tumor size ≤1 cm) and suggested a risk for tumor enlargement during pregnancy. However, a recent study from the same group indicated that only 8% of the 51 patients showed an increase in the tumor size of micro-PTCs, and no new cervical lymph node (LN) metastasis was detected (14). There are currently a limited number of studies assessing the changes in DTC during pregnancy, and no data on the changes of DTCs >1 cm have been reported.
In the present study, the changes of PTCs during pregnancy were evaluated by neck ultrasonography (US) in 19 patients who were diagnosed with PTC just before or during early pregnancy. Changes in cervical LNs and clinical outcomes after thyroid surgery were also evaluated.
Materials and Methods
Patients and study design
This historical cohort study included patients who were diagnosed with PTC just before or during early pregnancy and who underwent delayed thyroid surgery or continued active surveillance between January 2005 and February 2015. Patients who were diagnosed with PTC after 20 weeks of pregnancy or those who did not have follow-up neck US images obtained before thyroid surgery were excluded. Finally, 19 patients with PTC were included in the study. Changes in tumor size, volume, and US findings in patients with PTC during pregnancy were analyzed. The study protocol was approved by the Institutional Review Board of the Asan Medical Center.
Neck US examination and diagnosis of PTC
Images of the thyroid gland and neck area were obtained by US using either an iU22 unit (Philips Healthcare, Bothell, WA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz). All thyroid nodules in US images were evaluated with both transverse and longitudinal planes. The maximal diameter was measured from one outer margin to the other side outer margin of the nodule. Neck US examinations and fine-needle aspiration cytology (FNAC) were performed by 11 fellows of head and neck, part under the supervision of two experienced radiologists (13 and 20 years of experience of thyroid US). The follow-up US protocol is well established, as previously reported, and inter-observer variations in measurements of the diameter and volume of thyroid nodules were about 13% and 7%, respectively (15). Neck US examinations and FNAC were performed by experienced radiologists. FNAC was performed under US guidance using a 23-gauge needle. The preoperative diagnosis of PTC was based on the results of FNAC according to the Bethesda system (16). FNAC and surgical specimens were reviewed by experienced endocrine pathologists.
Analysis of US images during pregnancy
Changes in thyroid nodules, which were pathologically diagnosed as PTC, were analyzed from initial and follow-up US images obtained before thyroid surgery. The tumor size was defined as the maximum diameter of PTC on US images. In patients with multifocal PTCs, the dimensions of the largest PTC lesion were used. The tumor volume was calculated using the formula for ellipsoids modified by Brunn et al. (tumor volume = length × width × thickness × 0.479) (17). Progression of PTC was defined as a 20% increase in at least two nodule dimensions, with a minimum increase of 2 mm or >50% increase in volume (18). When a nodule was abutting to the thyroid capsule without intervening thyroid parenchyma, it was determined as a subcapsular location (19).
Follow-up protocol after the initial treatment
After the initial treatment for PTC, patients were regularly followed up with physical examination, as well as the measurement of serum thyroglobulin (Tg), anti-Tg antibodies (TgAb), and thyroid function, and neck US every 6–12 months, as previously reported (20,21).
Statistical analysis
Statistical analysis was performed using R v3.0 and R libraries (R Foundation for Statistical Computing, Vienna, Austria). Graphs were produced using GraphPad Prism v5.0 (GraphPad Software, Inc., San Diego, CA). Continuous variables are presented as the median with interquartile ranges (IQR), and categorical variables are presented as numbers with percentiles. The Wilcoxon rank-sum test was used to compare the size of the tumors between the initial and final US. All statistical tests were two-sided, and p < 0.05 was considered statistically significant.
Results
Baseline characteristics of patients and initial neck US findings
Table 1 shows the baseline characteristics of the patients. The median age of the 19 pregnant women at the time of diagnosis of PTC was 33 years (IQR 32.0–34.0 years). Most of the patients were diagnosed with PTC during or before the first trimester of pregnancy; only one patient was diagnosed during the second trimester of pregnancy. The median maximal size of tumors on initial neck US was 0.91 cm (IQR 0.61–1.11 cm), and 13 (68.4%) patients were considered to have micro-PTCs. The median tumor volume on initial US was 0.22 cm3 (IQR 0.07–0.41 cm3). Three patients had LN metastasis from PTC in the lateral cervical compartment (N1b). Most PTCs in the study patients were found incidentally, and only two patients were diagnosed with PTC because of a symptomatic (palpable neck mass) at presentation.
Interquartile range.
US, ultrasonography; LN, lymph node; FNAC, fine-needle aspiration cytology.
Changes of PTCs during pregnancy detected by neck US
The median interval between the initial and follow-up neck US was 9.5 months (IQR 5.4–14.3 months). A minimal increase in the maximal diameter and volume of tumors was observed during pregnancy. The median longest diameter changed from 0.91 to 0.98 cm (p = 0.16; Fig. 1A). The median tumor volume increased from 0.22 to 0.27 cm3 (p = 0.05; Fig. 1B). Three (16%) patients showed a meaningful increase in the maximal diameter, and five (26%) patients showed a meaningful volume increase. Changes in the maximal diameter of tumors in each trimester of pregnancy were evaluated in seven patients (Fig. 1C). The representative US images for the patients are shown in Supplementary Figure S1 (Supplementary Data are available online at
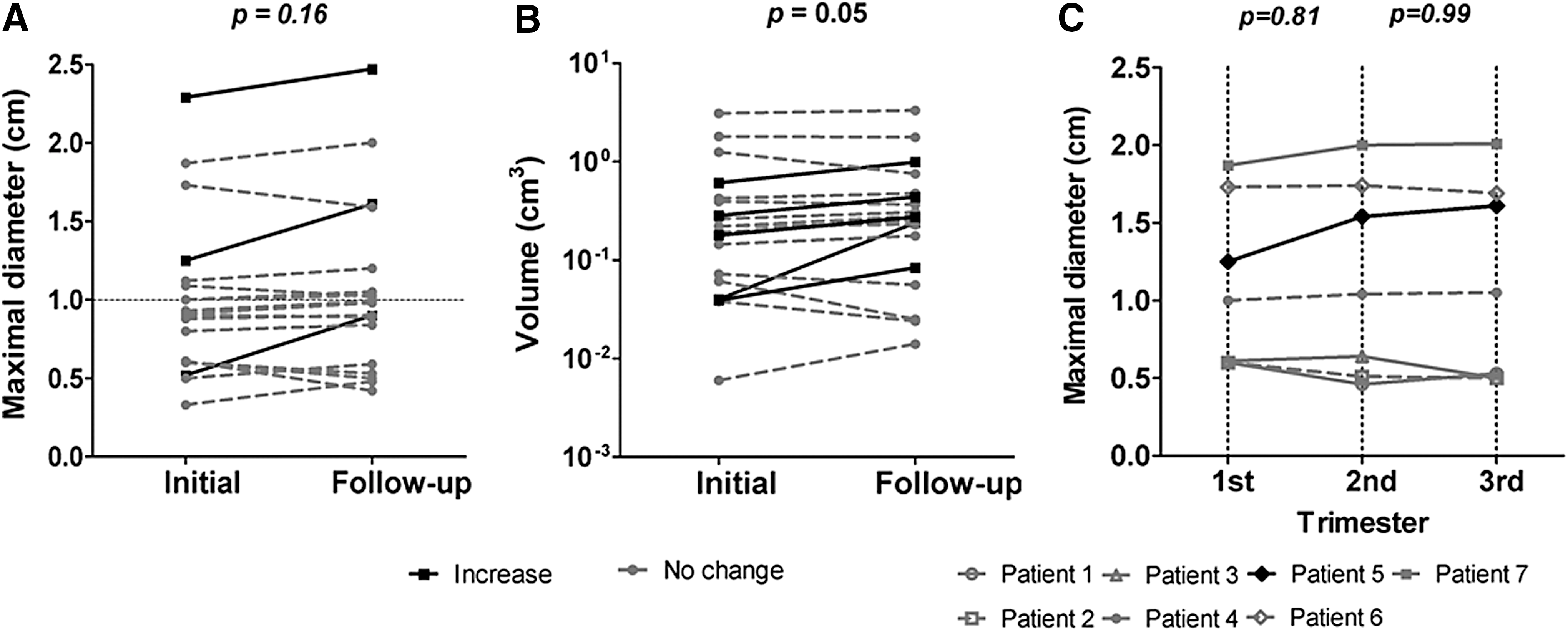
Changes in primary tumor size evaluated by neck ultrasonography (US) during pregnancy in patients with papillary thyroid carcinoma. Changes in maximal diameter (
Tumor size did not change significantly between trimesters during the 6.3 months of follow-up (first vs. second trimester p = 0.81; second vs. third trimester p = 0.99). Eight (42.1%) patients received thyrotropin (TSH) suppressive therapy before thyroid surgery, although there were no significant differences according to TSH suppression (p = 0.26). There was no newly developed cervical LN metastasis during pregnancy in the 16 patients without initial cervical LN metastases. Three patients showed metastatic LNs on the first US, and two of them showed a size increase of metastatic LNs on the follow-up US. The size of cervical LN metastasis increased from 1.96 to 2.67 cm in 5.3 months in one patient (#15). In the other patient (#16), the size of a metastatic LN increased from 0.95 to 1.46 cm, with internal bleeding, in 3.5 months. There were no additional LN metastases detected by follow-up US. Of note, there was no need for a change in the extent of surgery because of the delay in the patients with metastatic LNs.
Clinical and pathologic findings after thyroid surgery for PTCs
Most of the patients delivered at term, and two of the patients delivered at 36 weeks of pregnancy. Three patients with micro-PTCs were followed without thyroid surgery (active surveillance). Sixteen patients with PTC underwent thyroid surgery after delivery, and the median interval of delayed thyroid surgery was 11.9 months. The postoperative findings of these patients are summarized in Table 2. Most patients had classical PTC, and one patient had a tall-cell variant of PTC on pathological examination. Final pathology detected micro-PTCs in 11 (68.8%) patients and LN metastasis in nine (56.3%) patients. The median number of metastatic LN was 2.0 (IQR 1.0–6.0), and the median maximal diameter of the metastatic LN was 0.4 cm (IQR 0.4–1.1 cm). Multifocal PTCs were present in four (25.0%) patients, and nine (56.3%) patients had extrathyroidal extension. Six patients underwent radioiodine remnant ablation therapy. Serum Tg levels at one year after thyroid surgery are shown in Supplementary Table S1. None of the patients had persistent disease or a recurrence during the median 53.8 months (IQR 22.3–61.0 months) of follow-up.
CND, central lymph node dissection; MRND, modified radical neck dissection.
Discussion
This was a single-center study evaluating the changes of PTCs on serial neck US during pregnancy. A minimal increase in maximal tumor size and volume was observed during pregnancy. Three (16%) patients had a meaningful increase in maximal tumor size during the follow-up period, and no new cervical LN metastasis developed during pregnancy. These results support delayed thyroid surgery during pregnancy in patients with PTCs or micro-PTCs. Serial changes of PTCs were also examined in each trimester, and most patients showed no significant increase in tumor size. The present study included three patients with confirmed lateral cervical LN metastasis from PTC at initial diagnosis. The tumor size was >1 cm, and the tumor was located in the subcapsular area in all three patients. Two patients showed a meaningful size increase in both the primary tumor and metastatic cervical LNs on serial follow-up US. However, there was no change in the extent of the thyroid surgery because of the delay, and none of the patients developed distant metastasis. These findings suggest that delayed thyroid surgery during pregnancy can be considered for patients with PTCs.
Pregnancy is a unique condition, as it is accompanied by physiologic changes that can affect thyroid function and the thyroid gland itself. It is well established that human chorionic gonadotropin (hCG) stimulates the thyroid gland, which may be associated with thyroid tumor growth during pregnancy (22,23). Considering the marked rise of hCG during the first trimester, the tumor size could increase in early pregnancy. However, the present results show that the median maximal tumor size is comparable between trimesters in patients evaluated by neck US in each trimester (1.00 cm in the first trimester, 1.04 cm in the second trimester, and 1.05 cm in the third trimester). Thus, there was no apparent growth-stimulating effect of hCG on the thyroid tumors evaluated in the present study.
According to the recent ATA guidelines, TSH suppression therapy is recommended to maintain serum TSH levels at 0.1–1.0 mIU/L in pregnant women with PTC or suspicious PTC in their FNAC results (18). This recommendation is based on a study showing that high serum TSH concentration can be associated with an increased risk of thyroid cancer (24). However, a recent study indicated that this approach could increase the risk of thyrotoxicosis (TSH <0.1 mIU/L) in addition to the physiologically lower serum TSH level during pregnancy (25). In the present study, the changes in tumor size did not differ between the TSH suppression group and the other group during pregnancy. Currently, there is no clear evidence regarding the optimal serum TSH level in pregnant women with thyroid cancer or whether TSH suppressive therapy is helpful. Although the present study included only a small number of patients, this result raises questions and suggests a need for further studies addressing this issue.
The present study has limitations. The study consists of a historical cohort study, and there are limitations associated with its retrospective design. Not all patients performed serial neck US examinations in each trimester, and there were differences in the interval between US examinations. However, the median follow-up duration between the initial and the last preoperative US examination was 9.5 months, which is sufficient for assessing the sonographic changes during pregnancy. The relatively small number of patients is the other limitation of the study, and the possibility of selection bias needs to be considered. However, the findings are important because they support a conservative approach in patients with PTC during pregnancy, including patients with larger PTCs and those with lateral cervical LN metastasis. The tumor size change with maximal diameter and tumor volume was evaluated, and the results suggest that tumor volume is more sensitive to detect a change in tumor size.
In conclusion, the results of serial neck US showed no clinically relevant tumor growth or progression of PTCs in patients during pregnancy. Delayed thyroid surgery with active surveillance can be considered during pregnancy in PTC patients with or without cervical LN metastasis. Further comprehensive and larger prospective studies are needed to obtain more definitive evidence for the management of DTC in pregnant women.
Footnotes
Acknowledgments
This study was supported by a grant from the Korean Health Technology R&D project, Ministry of Health and Welfare, Republic of Korea (HC15C3372). An abstract covering part of this study was presented as a poster at the 86th Annual Meeting of the American Thyroid Association, September 23, 2016, in Denver, CO.
Author Disclosure Statement
No competing financial interests exist.