
Abstract
Background:
Despite improvements in the surgical and medical treatment of papillary thyroid carcinoma (PTC), subsets of patients suffer from structural recurrence after initial treatment. This study evaluated the timing and patterns of recurrence in completely resected PTC patients.
Methods:
A retrospective review of a prospectively maintained thyroid cancer database was performed. The timing and patterns of recurrence were reviewed in 2250 patients with PTC >1 cm who achieved complete remission after total thyroidectomy and/or radioactive iodine treatment. Univariate and multivariate analyses were performed to identify factors predictive of recurrence patterns.
Results:
During 8.1 years of mean follow-up, 68 (3.0%) patients developed structural recurrences: 53 lymph node recurrences (LNR), 11 local soft tissue recurrences (LR), and four distant recurrences (DR). Two patients died of DR. Younger patients had a higher proportion of LNR, and older patients had a tendency toward LR/DR. LNR showed a peak incidence between one and three years after remission, but LR/DR showed a delayed peak incidence between two and four years. The factors that significantly increased the risk of LNR were multifocal tumor and lymph node metastasis (central/lateral). The factors that increased the risk of LR/DR were old age, large tumor size (>2 cm), and lateral lymph node metastasis. In addition, central neck dissection significantly reduced subsequent LR/DR.
Conclusion:
Patterns of recurrence after complete PTC resection are variable and associated with specific clinicopathologic factors. Understanding the timing and patterns of recurrence may lead to more effective adjuvant treatment and improved long-term follow-up strategies.
Introduction
T
Most PTC recurrences occur in the lymph nodes. Non–lymph node recurrences such as local soft-tissue or distant-organ recurrences are rare. Therefore, PTC recurrence types are classified into three groups according to location in this study: lymph node recurrence (LNR), local soft-tissue recurrence (LR), and distant recurrence (DR) (7,10,11). Previous studies of other cancers, such as breast or esophageal cancer, suggested that each recurrence pattern has unique risk factors (12 –17). Time to recurrence and prognosis also shows differences according to pattern (12,16). Thus, it was hypothesized that the recurrence pattern in PTC is linked to different clinical features. Furthermore, each pattern of recurrence could be associated with a different prognosis.
This study evaluated the timing and patterns of recurrence in completely resected PTC patients. It also investigated the predictive factors of each recurrence pattern.
Materials and Methods
The prospectively maintained institutional thyroid cancer database of 2250 consecutive patients who achieved remission for PTC at Samsung Medical Center between 1994 and 2010 was retrospectively reviewed. The Institutional Review Board at Samsung Medical Center approved this study. Patients <18 years old and with an initial tumor size <1.0 cm were excluded from this study (Fig. 1).
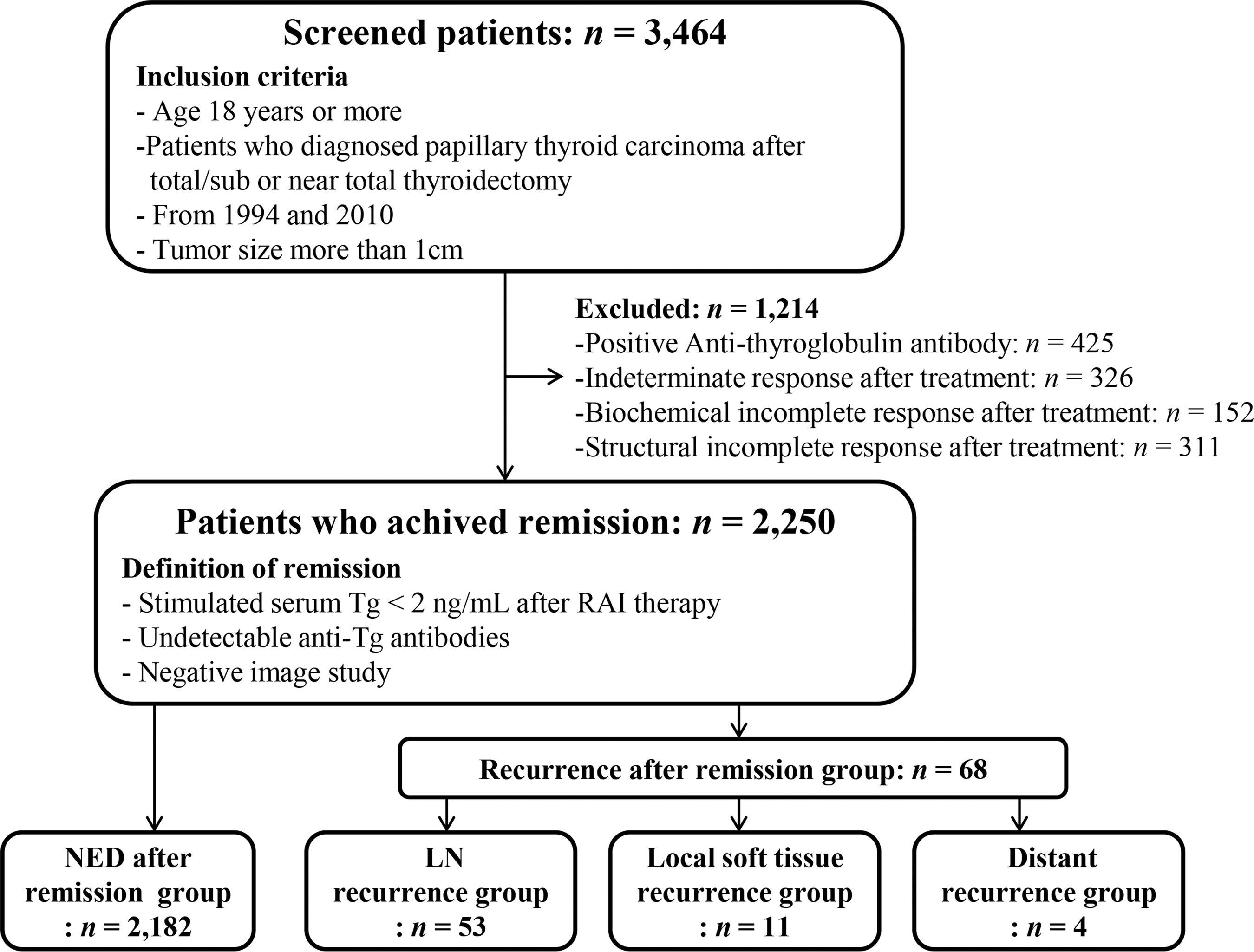
Flow diagram of study subjects. For analysis of recurrence, patients who achieved remission were included. These patients were subdivided into no evidence of recurrence (NED), lymph node recurrence (LNR), local soft-tissue recurrence (LR), and distant recurrence (DR).
Remission was defined as stimulated serum thyroglobulin (Tg) <2 ng/mL with undetectable anti-Tg antibodies (<60 IU/mL), absence of significant visible uptake above background activity in the neck on diagnostic whole-body scan, and negative ultrasonography after initial therapy (2,7,9). Recurrence was noted when a recurred lesion was detected after remission. PTC recurrence types were classified into three groups: LNR, LR, and DR according to location. LNR included recurrence in either the central or lateral LN. LR was defined as recurrence in the thyroid bed or perithyroidal soft tissue except the lymph nodes. Both LNR and LR were diagnosed as pathological confirmation after aspiration or reoperation. DR was found by pathological confirmation or imaging studies such as whole-body scan, computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) scans (17). Various factors that could affect the recurrence of PTC were included for analysis (17 –22). Age at initial diagnosis and sex were included as patient factors. Surgeon volume, type of surgery (total thyroidectomy or near/subtotal thyroidectomy), initial central neck dissection, and radioactive iodine (RAI) therapy were included as treatment factors. A high-volume surgeon was defined as performing >100 thyroid surgery cases in one year (17). Initial central neck dissection was defined based on the review of operative note. Tumor histology, tumor size, multifocal tumor, extrathyroidal extension, resection margin, lymph node metastasis, and distant metastasis were included as tumor factors. Unfavorable tumor histology included tall cell, diffuse sclerosing, columnar cell, solid, and hobnail variants of PTC (17). Multifocal tumor was defined as two or more discrete areas of PTC within the surgical specimen.
Almost all (99%) of the patients in this study had undergone total thyroidectomy. Prophylactic central neck dissection (ipsilateral or bilateral) was performed in 85% of patients. Therapeutic lateral neck dissection was performed in some patients with biopsy-proven lateral cervical lymph node metastasis. Most (92%) patients were treated with RAI following levothyroxine withdrawal or recombinant human thyrotropin (rhTSH) stimulation. An initial dose of 30–200 mCi of 131I was used for remnant ablation or treatment of remaining or metastatic disease. Serum Tg and anti-Tg antibodies had been measured at three months after surgery and then every six months during the first five years, and every 12 months thereafter. Following surgery, cervical USG was performed at 6–12 months and then periodically, depending on the patient's risk for disease and the Tg status. Various imaging modalities, including neck and chest CT, MRI, and PET scans, and cytological/histological proof were obtained to detect recurrent or metastatic lesions. TSH suppression therapy by levothyroxine was maintained to achieve an optimal serum TSH level.
Statistical analysis
Continuous data are expressed as mean ± standard deviation (SD). Data on categorical characteristics are expressed as percent values or absolute numbers. For comparison of clinical and pathological characteristics among groups, a chi-square test or Fisher's exact test was used for categorical data, and a t-test or Mann–Whitney test was used for continuous data. For calculated disease-free survival (DFS), a Kaplan–Meier test was performed. Multivariate Cox's proportional hazard model applying the backward elimination method was used to identify independent factors associated with each pattern of recurrence. A p-value of <0.05 was considered significant. Statistical analysis was performed using IBM SPSS Statistics for Windows v23 (IBM Corp., Armonk, NY).
Results
Baseline clinical and pathological characteristics of all patients with PTC
Data were retrieved for 2250 patients who achieved remission after optimal therapy for PTC >1 cm in diameter. The clinicopathologic characteristics of patients are shown in Table 1. Among them, 1842 (82%) were women and 408 (18%) were men. The mean age was 48 years (range 18–86 years). A total of 2230 (99%) patients underwent total thyroidectomy, and 1914 (85%) underwent central neck dissection. After surgery, 2064 (92%) patients were treated with RAI. The mean primary tumor size was 1.77 cm (range 1.1–10.8 cm). Lymph node metastases in the central and lateral neck were noted in 1191 (53%) and 345 (15%) patients, respectively. Gross extrathyroidal extension was found in 539 (24%) patients. Advanced stages (stage III and IV) were found in 1108 (49%) patients. Although 220 (9.8%) patients had TNM stage IV, 218 (9.7%) patients were TNM stage IVA (N1b). The mean duration from initial operation to last follow-up was 8.1 ± 3.8 years.
Continuous data are given as mean ± SD; categorical data are given as absolute numbers (percentage values).
RAI, radioactive iodine; CND, central neck dissection; ETE, extrathyroidal extension; LNM, lymph node metastasis; SD, standard deviation.
The five-year disease-free survival (DFS) rate was 97.8%, and the 10-year rate was 95.6%. Among the patients, 2182 (97%) had no recurrence after initial remission (no evidence of disease [NED] group). However, 68 (3%) patients experienced disease recurrence during the follow-up period (recurrence group).
Comparison of the clinical features of the recurrence group and the NED group
The clinical characteristics of the recurrence group were compared to the NED group. The recurrence group was significantly associated with unfavorable histology, large tumor size, and central and lateral lymph node metastases (p < 0.05). The NED group had a higher proportion of patients treated by a high-volume surgeon than did the recurrence group (p = 0.042; Supplementary Table S1; Supplementary Data are available online at
When classified by the American Thyroid Association (ATA) initial risk stratification system, 105 patients were in the low risk of recurrence category, 1600 patients were intermediate risk, and 545 high risk. The recurrence rates according to the ATA initial risk groups were 1.91% (two patients with low risk), 3.06% (49 patients with intermediate risk), and 3.12% (17 patients with high risk; Supplementary Table S2).
Risk factors associated with each recurrence type
The clinical characteristics of each recurrence type were compared to those of the NED group. We classified recurrence into three types: LNR (n = 53), LR (n = 11), and DR (n = 4) according to location (Fig. 1). LR and DR were analyzed together because they had a small number of patients and similar clinical characteristics (Fig. 2).
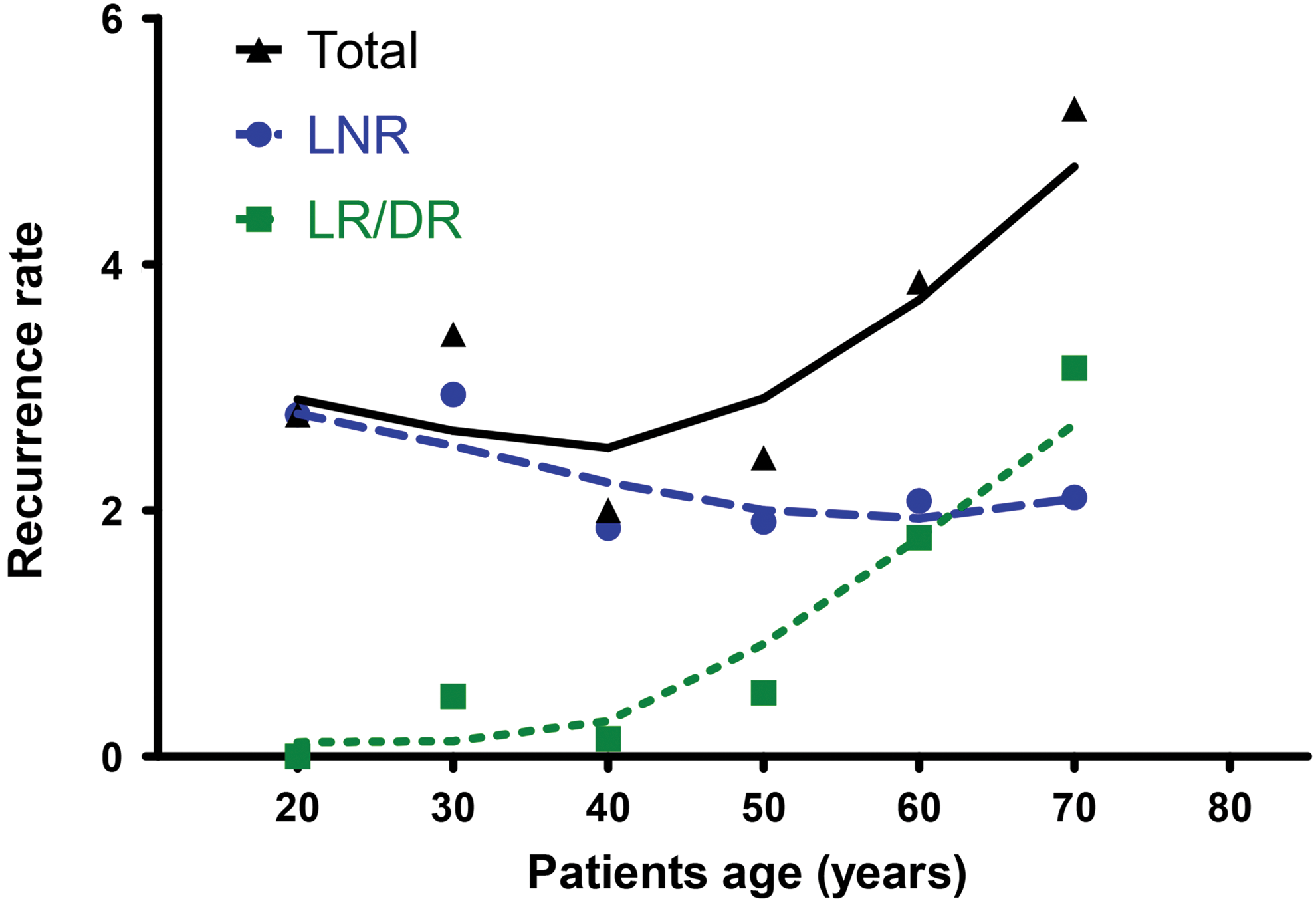
Recurrence rates according to age. Total recurrence rate showed a modified U-shape. However, subdivided into recurrence pattern, younger patients had more lymph node recurrence, and older patients had a tendency for increased LR/DR rate according to increased age. Color images available online at
On univariate analysis, LNR showed significant differences in unfavorable histology, large tumor size, and central and lateral lymph node metastases compared to the NED group (p < 0.05). LR and DR showed significant differences with regard to old age, proportion of initial central neck dissection, and tumor size compared to the NED group (p < 0.05; Table 2).
Continuous data are given as mean ± SD; categorical data are given as absolute numbers (percentage values); a chi-square test or Fisher's exact test were used for categorical data, and a t-test or Mann–Whitney test was used for continuous data.
p < 0.05; ** p < 0.01.
NED, no evidence of disease; LNR, lymph node recurrence; LR, local soft-tissue recurrence; DR, distant recurrence.
Cox's proportional hazard model was used to evaluate the risk factors for each type of recurrence. In unadjusted analysis, tumor size, multifocal tumor, unfavorable histology, and central and lateral lymph node metastases were significant risk factors for LNR (p < 0.05). When adjusted for all other variables, multifocal tumor and central and lateral lymph node metastases were independent risk factors for LNR (Table 3). Age, initial central neck dissection, and tumor size were significantly associated with LR/DR in unadjusted analysis. When adjusted for other variables, age, initial central neck dissection, tumor size, and lateral lymph node metastasis were independently associated with LR/DR (p < 0.05). Unfavorable histology was not adjusted because LR/DR did not have unfavorable histology. When tumor size was stratified into three groups (1–2 cm, 2–4 cm, and >4 cm), tumor size >2 cm was a significant risk factor for LR/DR (hazard ratio [HR] = 5.87 [confidence interval (CI) 1.40–24.65]; p = 0.016; Table 4).
Multivariate Cox proportional hazard ratio analysis was performed.
CI, confidence interval; HR, hazard ratio.
Multivariate Cox-proportional hazard ratio analysis was performed.
CI, confidence interval; CND, central neck dissection; RAI, radioactive iodine; ETE, extra-thyroidal extension; LNM, lymph node metastasis.
Different recurrence patterns according to age and recurrence time
The recurrence rate of each type according to age was analyzed. In LNR, the recurrence rate showed a peak at 20–39 years. However, it increased with age in LR/DR (Fig. 2). The recurrence rate of each type according to recurrence time was also analyzed. Recurrences were found at 3.86 ± 3.04 years in LNR and 4.38 ± 1.89 years in LR/DR after remission, respectively (Table 2). In LNR, recurrence increased sharply, showed a peak at one to three years, and was noted until 14 years. However, LR/DR showed a minor peak at two to four years and lasted until eight years (Fig. 3).
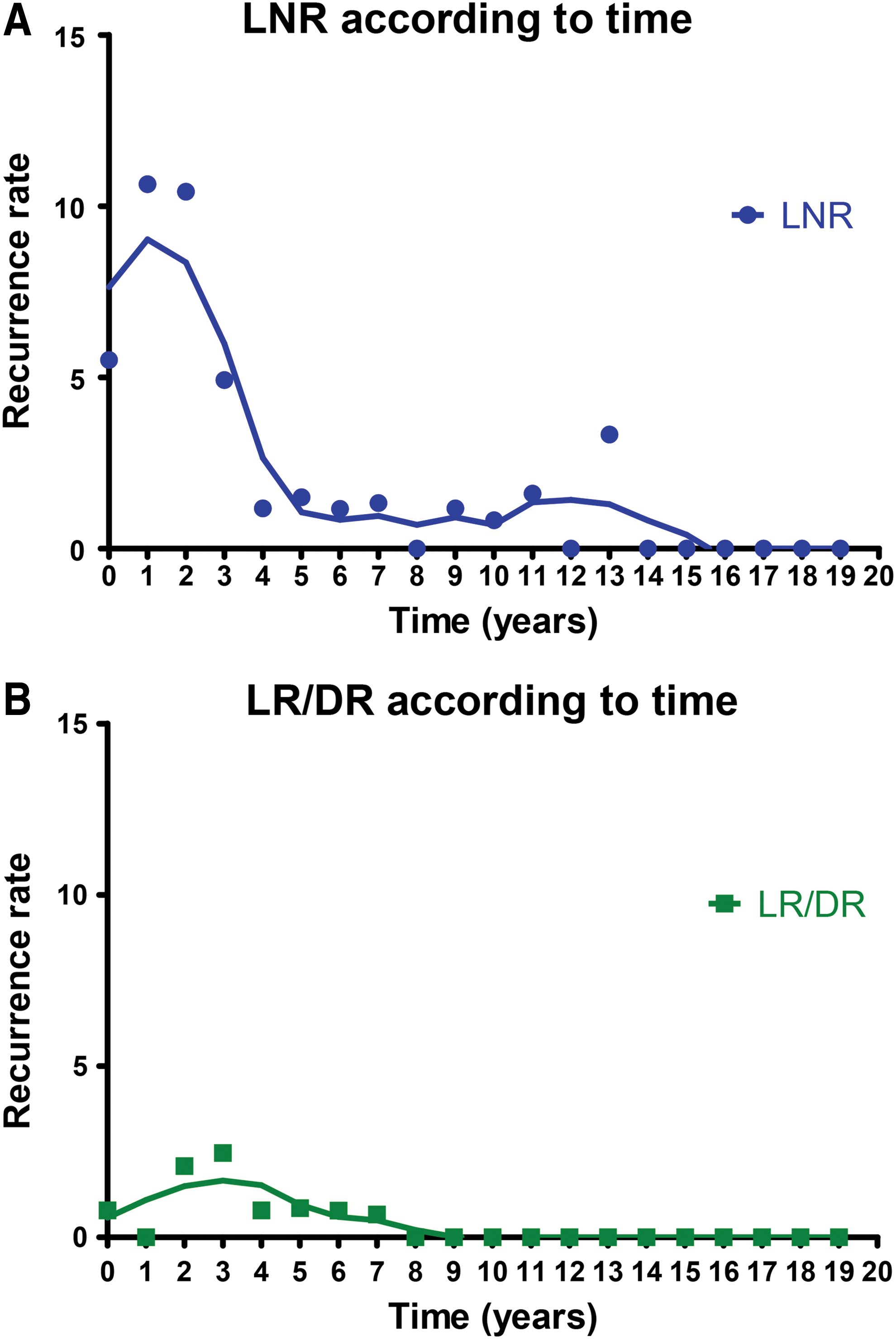
Recurrence rates according to time. (
Final outcomes of recurred patients
Among 53 patients with LNR, 41 (77%) achieved remission after additional therapy. Three patients had persistent disease, and two patients did not receive additional treatment. Seven patients were lost to follow-up. Among 11 patients with LR, eight (73%) achieved remission after additional therapy. Two patients had persistent disease, and one was lost to follow-up. Among four patients with DR, two died at 1.2 and 4.3 years after recurrence, respectively. The other two patients were living with stable distant metastases.
Discussion
This study suggests that different recurrence sites have different clinical features in PTC. Recurrence rates for different recurrence sites differed according to age and recurrence time. Multifocal tumor and central and lateral lymph node metastases were independent risk factors for LNR, but older age, absence of the initial central lymph node dissection, tumor size >2 cm, and lateral lymph node metastasis were independent risk factors for LR/DR.
This study included patients with PTC >1 cm in diameter who achieved remission after initial therapy. Recurrence was noted when a recurred lesion was detected after remission (7,9). However, recurrence in most previous studies was defined when structural evidence of disease was found after initial therapy. In that case, patients with persistent disease could be included in the recurrence subjects. In this study, remission was defined as stimulated serum Tg <2 ng/mL with undetectable anti-Tg antibodies, absence of significant visible uptake above background activity in the neck on diagnostic whole-body scan, and negative USG after initial therapy. Therefore, patients with structurally or biochemically persistent disease were excluded. Due to the strict definition of recurrence, clinical characteristics and rates of recurrence in this study were different from those of other studies (1,2,5).
This study suggests that the different recurrence types are associated with different risk factors and prognosis. A previous study indicated that both younger and older patients had high recurrence rates (5). Overall recurrence rate according to age showed a U-shape. Although young patients with PTC had a high recurrence rate, their mortality rate was low (4). However, older patients with PTC had high recurrence and high mortality rates. Therefore, it was assumed that these two types of recurrence are associated with different clinical characteristics. In this study, although the overall recurrence rate showed a modified U-shape, LNR showed a peak at younger ages (20–39 years), while LR/DR increased with age. In addition, only two LR/DR patients died at 1.2 and 4.3 years after recurrence, respectively. These findings indicate that LNR is associated with low-mortality recurrence in younger patients. However, LR/DR may be associated with high-mortality recurrence in older patients.
When the recurrence rate according to recurrence time was analyzed, most recurrences occurred within four years. This is a consistent finding with a previous study that evaluated the time to recurrence (2). Recurrence rate according to recurrence time was quite different among recurrence types. LNR showed an early peak at one to three years after remission and then declined but lasted until 14 years. However, LR/DR showed a relatively late minor peak at two to four years after remission and lasted until eight years. Most recurrences occurring after eight years were LNR, which was not associated with mortality and seems to represent slow-growing tumors.
Previous studies reported that initial central neck dissection could decrease disease-specific mortality (23,24). In this study, most patients (85%) underwent initial central lymph node dissection. In multivariate analysis, initial central lymph node dissection significantly decreased LR/DR (HR = 0.20 [CI 0.05–0.71]; p = 0.013). This finding suggests that initial central neck dissection decreases disease-specific mortality by reducing LR/DR not LNR.
To the authors' knowledge, this is the first study that evaluated the clinical characteristics of PTC recurrence patients according to pattern of recurrence after remission. Each pattern of recurrence had distinct clinical characteristics and could have a different impact on prognosis. LR/DR had worse prognosis than LNR, and the risk factors were old age, tumor size >2 cm, and lateral lymph node metastasis. In order to reduce and prevent the morbidity of LR/DR in PTC patients with risk factors, prophylactic central lymph node dissection should be incorporated at initial surgery, and vigilant monitoring should be pursued.
There are several limitations to this study. First, there were a relatively small number of patients with recurrences. This study included only patients in remission, and a strict definition of recurrence was applied. Recurrence rate after remission is lower than that after initial treatment (2). Biochemical abnormalities, any evidence of disease on imaging studies, or biopsy-proven disease without remission were considered as persistent disease rather than recurrent disease. Second, the DR number was too small to perform statistical analysis. Therefore, LR and DR were analyzed together because they showed similar recurrence patterns. However, LR and DR might have different clinical characteristics and different risk factors. It is necessary to compare LR to DR in a further large-scale study. Third, because there were only two deceased patients in this study, survival analyses could not be performed. Lastly, the present study did not evaluate the genetic background of the tumors such as BRAF and TERT promoter mutations (25).
In summary, the pattern of recurrence showed a different incidence according to time course and patient age. This finding has an important impact on prognosis. Furthermore, each recurrence pattern was associated with a different spectrum of risk factors. Understanding the timing and patterns of recurrence may lead to more effective adjuvant treatment and improved long-term follow-up strategies.
Footnotes
Acknowledgments
We thank statistician Seonwoo Kim, PhD, of Samsung Biomedical Research Institute for her assistance in statistical analysis.
Author Disclosure Statement
None of the authors has anything to declare.