
Abstract
Background:
There is a lack of well-powered data regarding outcomes in stage IV differentiated thyroid carcinoma (DTC) treated with postsurgical radiation. The objective of this study was to examine survival in patients with stage IV papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC) who received radioactive iodine (RAI), external beam radiation therapy (EBRT), or neither following surgery.
Methods:
In this retrospective cohort study, data collected from the National Cancer Data Base (NCDB) yielded 11,832 patients with stage IV DTC who underwent primary surgical treatment between 2002 and 2012. Patients were stratified by histology and sub-stage. Fully parametric, multilevel survival-time models were used to evaluate survival outcomes in three adjuvant treatment groups: RAI, EBRT, or no adjuvant radiation. Hazard ratios (HR) and time ratios (TR) were calculated against patients who did not receive radiation. All models were adjusted for demographic and clinical factors.
Results:
The mean age of all patients was 61.6 years (SD = 11.6), and 57.5% were female. Patients who received EBRT had significantly higher 5- and 10-year hazards of death in several PTC sub-stages (10-year HRPTC Stage IV-A = 2.12 [confidence interval (CI) 1.79–2.52]; HRPTC Stage IV-B = 2.03 [CI 1.33–3.10]). For stage IV-B PTC requiring EBRT, lifespan after diagnosis was shortened by a factor of 3 when compared to patients who did not receive radiation (TRPTC Stage IV-B = 0.32 [CI 0.16–0.62]). In contrast, RAI was significantly associated with improved 5- and 10-year survival in both PTC and FTC patients regardless of pathological sub-stage. Large reductions in mortality were observed in patients with FTC who were treated with RAI (HRFTC Stage IV-C = 0.19 [CI 0.06–0.65]). When patients with stage IV-C FTC were treated with RAI, life-span after diagnosis doubled (TRFTC Stage IV-C = 1.98 [CI 1.31–3.00]).
Conclusions:
Through the NCDB, this study sought to describe prognosis and survival for adjuvant radiation in stage IV DTC. RAI was associated with improved survival for stage IV DTC. Despite treatment benefits conferred by adjuvant EBRT, indications to treat with EBRT were associated with poorer survival outcomes in patients with advanced-stage DTC, particularly PTC.
Introduction
R
Multiple retrospective studies have indicated that treatment with radiation is beneficial to survival outcomes in particular postsurgical populations (3). Practice guidelines from the American Head and Neck Society (AHNS) specifically delineate that external beam radiation therapy (EBRT) is recommended in patients with gross residual disease following surgical resection, except for those <45 years of age with disease that has high avidity for radioactive iodine (RAI), and in patients >45 years of age with likely microscopic disease that is not RAI avid (4). The ATA recommends treatment with RAI in patients with T2–T4 or N1 or M1 disease (5). However, there have been few well-powered studies examining the outcomes of adjuvant radiation in advanced disease. The purpose of this investigation was to evaluate survival trends and differences in a large cohort of patients with stage IV DTC treated with RAI, EBRT, or neither following surgery.
Materials and Methods
Data acquisition
The National Cancer Data Base (NCDB) collects mortality data for a random sample of all inpatient discharges with cancer diagnoses. Data were collected from the NCDB from 2002 to 2012, which yielded a cohort of 11,832 patients with stage IV DTC who underwent primary surgical treatment.
Ethical approval
All records were de-identified at the time of acquisition. In accordance with Louisiana State University guidelines and the Policy for Protection of Human Research Subjects of the U.S. Code of Federal Regulations, Institutional Review Board approval was not required for this study.
Data measures and outcomes
Patients were stratified by cancer histology, specifically follicular thyroid carcinoma (FTC) versus papillary thyroid carcinoma (PTC). The NCBD histology codes used to categorize participants into the FTC group were as follows: 8050, 8260, 8340, 8342, 8343, 8344, or 8350. Participants were classified into the PTC group if they had any of the following codes: 8290, 8330, 8331, 8332, or 8335 (Supplementary Table S1; Supplementary Data are available online at
Data were also collected from the NCDB regarding demographics, treatments, histologic grade, and American Joint Committee on Cancer (AJCC) staging. Patients were additionally stratified by sub-stage into three groups: IV-A, IV-B, and IV-C. The primary outcome of interest was all-cause mortality starting at the time of diagnosis. Data regarding disease-specific survival and recurrence were not available through the NCDB. Administrative censoring was implemented after 5 and 10 years of survival time.
Exposure
All patients received surgical treatment with thyroidectomy. Patients subsequently received one of three types of adjuvant radiation therapy (RT): RAI, EBRT, or no RT.
Statistical analysis
Data management and all statistical analyses were performed using STATA/SE v13 (StataCorp). Continuous variables are presented as median (interquartile range [IQR]), and categorical variables are presented as the number (proportion) of patients. p-Values for continuous variables correspond to Wilcoxon rank-sum tests for two-group comparisons and Kruskal–Wallis tests for comparisons of more than two groups. p-Values for categorical variables correspond to Pearson's chi-square tests.
Multi-level (random effects) models were used to adjust for the clustering scheme intrinsic to the NCDB. Patients may be nested within years if they have the same procedure more than once or within hospitals if they have more than one procedure in the same hospital. Additionally, hospitals may be nested within regions, resulting in a potential source of bias due to differences in practice by hospital.
The survival of 11,832 patients representing 56,764.46 person-years at risk was analyzed using fully parametric, multi-level survival-time models using Weibull distributions to obtain unadjusted and adjusted hazard ratios (HR) with corresponding confidence intervals (CI). All survival models assume proportional hazards between groups. Analyses were performed as univariate models and were subsequently adjusted using multivariable models for age, sex, race/ethnicity, clinical variables (surgical length of stay, treatment with neck dissection), and socioeconomic factors (insurance status, primary payer, median income quartile of patient zip code, and percent of residents without a high school education in patient zip code).
Unadjusted and adjusted time ratios (TR) with corresponding CI were also calculated. TR is an alternative and effective measure of relative hazard. Provided is an explanation of the mathematical relationship between the survival function and TR. For this example, only two cohorts are used (EBRT vs. no RT).
Given that two groups are exposed to different treatments, the survival over time of the reference group (no RT) is represented by the function S
noRT(t), and the survival of the comparison group (EBRT) is S
EBRT(t). The relative times (TR) are defined for 0 < p < 1, where p is the proportion of patients, as the ration of corresponding quantiles, therefore:
where
Results
Descriptive statistics
Within the study cohort of 11,832 patients, 1036 (8.76%) had FTC and 10,796 (91.24%) had PTC. Table 1 shows a profile of socio-demographic and clinical variables stratified by DTC type and by RT treatment group.
p-Values for age and surgical length of stay (SLOS) were obtained using non-parametric tests (see Methods). All other p-values were obtained using Pearson chi-square tests.
p < 0.1; ** p < 0.05; *** p < 0.001.
NS, no statistically significant difference (p > 0.1); FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma; RT, radiation therapy; NCDB, National Cancer Data Base; EBRT, external beam radiation therapy; RAI, radioiodine therapy; LN, lymph node; AJCC, American Joint Committee on Cancer.
FTC-specific trends
Patients with FTC who were treated with RAI were significantly younger (median 66 years [IQR 58–75 years]) than patients who received EBRT (median 69 years [IQR 62.5–77 years]) or no RT (median 73 years [IQR 61–80 years]). There were no significant differences in sex, ethnicity, primary payer, median income quartile, or percent of high school education between the three RT groups for patients with FTC. RAI patients had a greater proportion treated with neck dissection (47.4%) than patients who did not receive adjuvant RT (35.7%) or EBRT (33.0%). The most common AJCC sub-stage among FTC patients was stage IV-C across all RT groups (no RT = 47.6%; EBRT = 64.6%; RAI = 53.5%). The next most common was stage IV-A (no RT = 39.5%; EBRT = 23.1%; RAI = 39.2%), followed lastly by stage IV-B (no RT = 12.9%; EBRT = 12.3%; RAI = 7.2%).
There were statistically significant differences in 5- and 10-year mortality between RT groups. FTC patients treated with EBRT had the highest mortality rate, with 51.4% at 5 years and 59.9% at 10 years, compared to 45.5% at 5 years and 51% at 10 years in patients who received no adjuvant RT. Patients treated with adjuvant RAI had the lowest mortality, with 29.2% at 5 years and 36.8% at 10 years. Kaplan–Meier curves for survival among FTC patients stratified by treatment are presented in Figure 1.
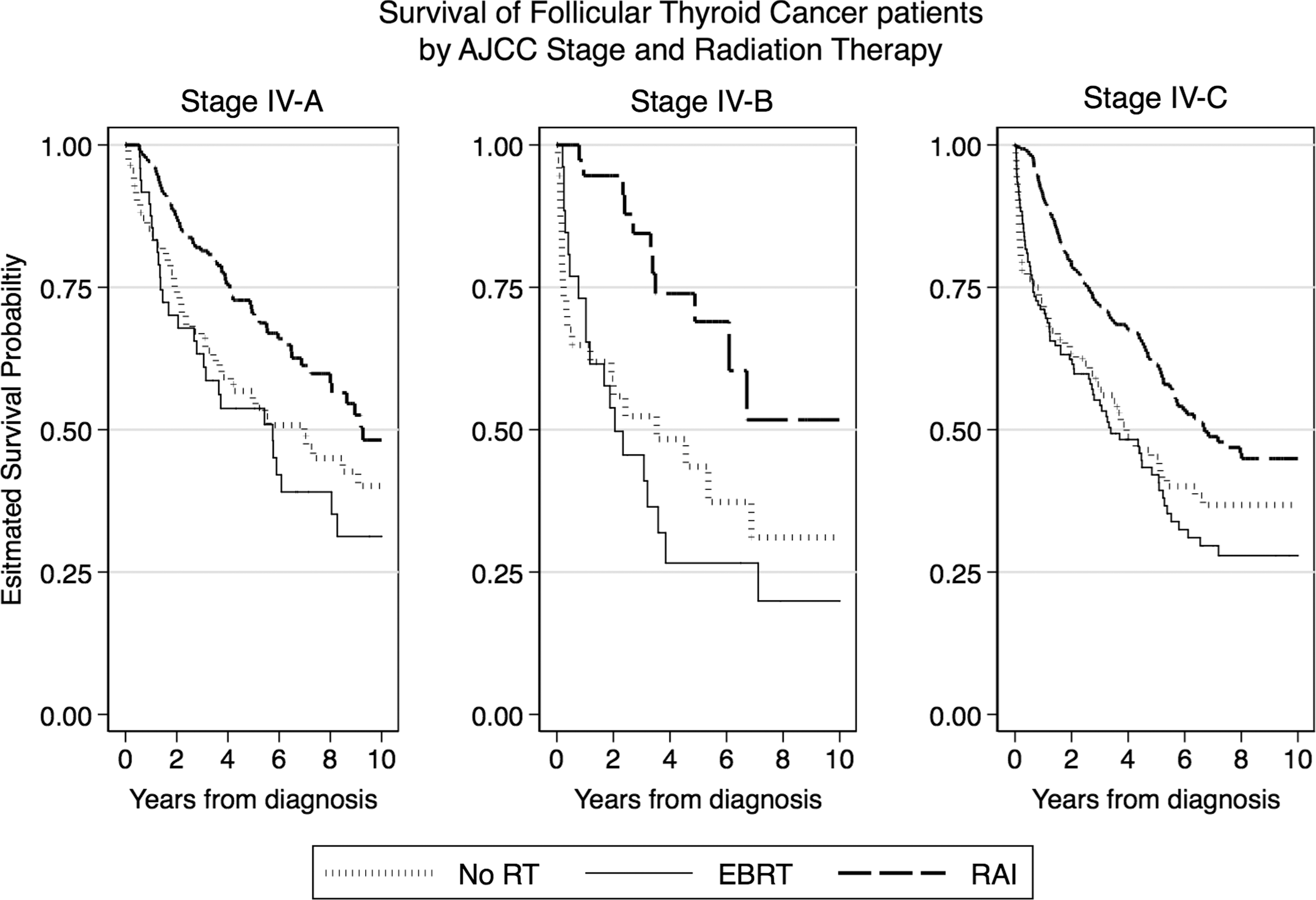
Stage IV follicular thyroid carcinoma (FTC) survival. Kaplan–Meier estimation of 10-year survival of FTC patients stratified by American Joint Committee on Cancer (AJCC) sub-stage and adjuvant radiation therapy (RT) received.
PTC-specific trends
PTC patients who were treated with RAI were also significantly younger (median 58 years [IQR 51–68 years]) than those who received no RT (median 61 years [IQR 52–72 years]) or EBRT (median 65 years [IQR 57–74 years]). For all RT groups, the majority of patients were female (no RT = 59%; EBRT = 50.5%; RAI = 58%). A large majority of patients in all groups were ethnically white/Caucasian (no RT = 85%; EBRT = 84.4%; RAI = 87.2%). With regards to primary payer, 47.6% of patients who did not receive adjuvant RT had private insurance, 39.5% had Medicare, and 5.3% had Medicaid. In comparison, EBRT patients were less likely to have private coverage (38.1%) and more likely to have Medicare (50.3%), with a similar proportion of Medicaid (5.6%). Conversely, patients treated with RAI had a greater proportion of patients with private insurance at 59%, with fewer patients covered by Medicare (31.7%) or Medicaid (4.3%). These differences in primary payer were statistically significant (p < 0.001).
In contrast to FTC patients, the majority of PTC patients underwent surgical neck dissection. Of PTC patients treated with RAI, 86.8% underwent neck dissection compared to 80.3% of patients who received no RT and 72.5% treated with EBRT. Unlike FTC patients, most PTC patients regardless of RT group were classified as AJCC stage IV-A (no RT = 81.5%; EBRT = 51.2%; RAI = 86.7%). The next most common stage was IV-C (no RT = 12%; EBRT = 31.5%; RAI = 9.7%), followed lastly by stage IV-B (no RT = 6.5%; EBRT = 17.4%; RAI = 3.6%).
Mortality trends similar to the FTC group were noted in the PTC group, with significant differences in 5- and 10-year survival between RT groups. Those treated with EBRT had the highest mortality, with 46.6% at 5 years and 50.7% at 10 years. Patients who were not treated with RT had 22.7% mortality at 5 years and 25.5% mortality at 10 years. PTC patients who received RAI had the lowest mortality rates: 11.0% at 5 years and 14.0% at 10 years. Kaplan–Meier curves for survival among PTC patients stratified by treatment are presented in Figure 2.
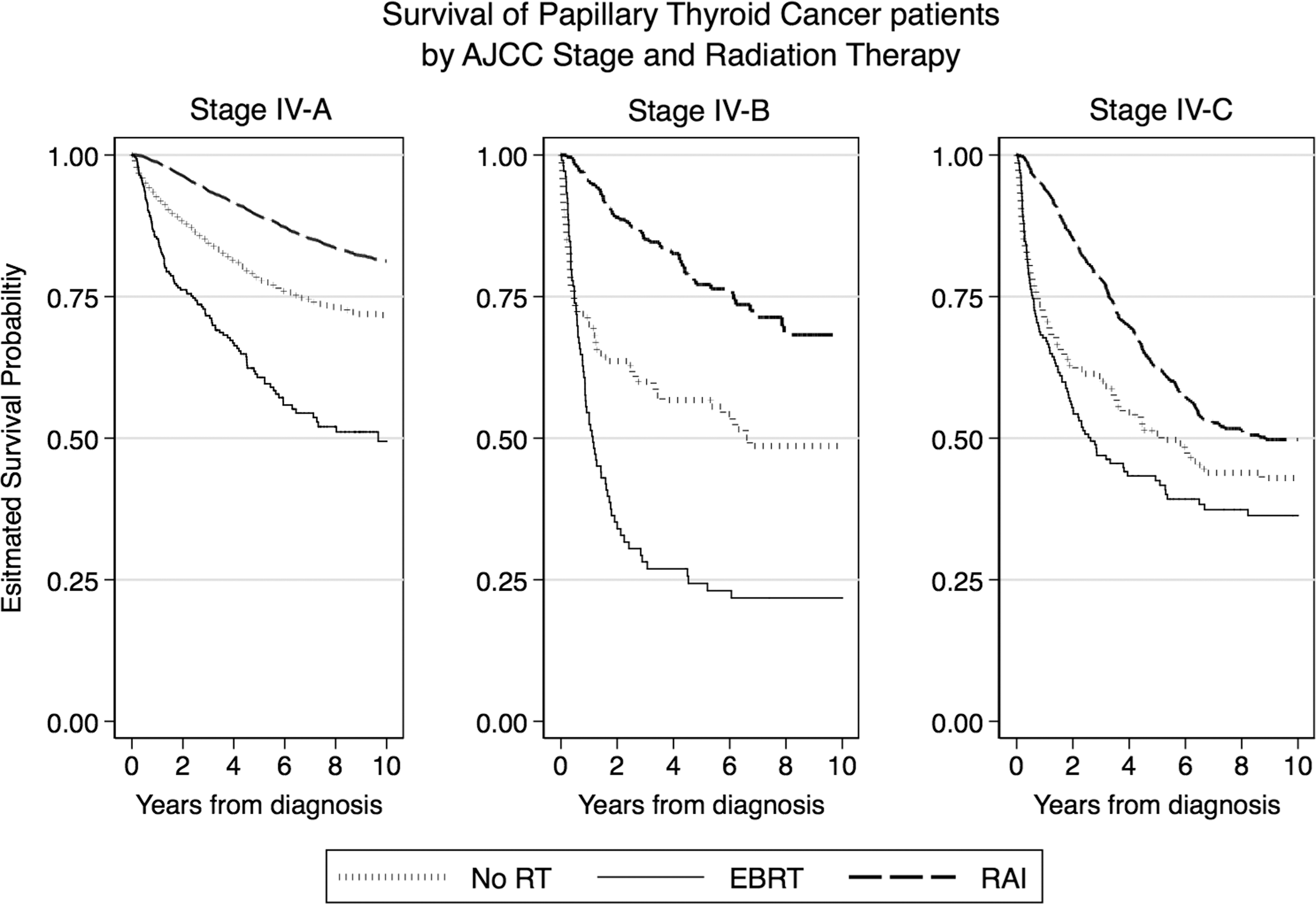
Stage IV papillary thyroid carcinoma (PTC) survival. Kaplan–Meier estimation of 10-year survival of PTC patients stratified by AJCC sub-stage and adjuvant RT received.
Univariate analysis
Several statistically significant associations were identified on univariate analysis to increase hazards of death (Table 2). Patients with stage IV-A and IV-B PTC who were treated with adjuvant EBRT had a significantly higher five-year hazard of death (HRPTC Stage IV-A = 2.04 [CI 1.74–2.39]; HRPTC Stage IV-B = 2.23 [CI 1.42–3.51]) and 10-year hazard of death (HRPTC Stage IV-A = 2.12 [CI 1.79–2.52]; HRPTC Stage IV-B = 2.03 [CI 1.33–3.10]) compared to their counterparts who did not receive RT. No other EBRT groups showed statistically significant increases in hazard of death compared to patients who did not receive RT.
p < 0.1; ** p < 0.05; *** p < 0.001.
CI, 95% confidence interval.
RAI was significantly associated with better survival in both PTC and FTC, regardless of stage. RAI groups had a 5- and 10-year reduction in hazard of death compared to patients who did not receive RT. The largest death hazard reduction was observed in the five-year survival of RAI patients with stage IV-B FTC (HRFTC Stage IV-B = 0.31 [CI 0.12–0.80]), while the most modest reduction was observed in the 10-year survival of patients with stage IV-A FTC (HRFTC Stage IV-A = 0.62 [CI 0.53–0.72]).
Multivariable analysis
Multivariable analyses were performed to control for study design elements such as clustering, clinical factors, and demographic differences and did not differ from univariate results, with two exceptions (Table 3). The increased hazard of death observed in univariate analysis comparing EBRT versus no RT for patients with stage IV-A PTC was no longer statistically significant at 5 years (HRPTC Stage IV-A = 1.2 [CI 0.91–1.59]) or 10 years (HRPTC Stage IV-A = 1.29 [CI 0.93–1.79]). However, treatment with EBRT in patients with stage IV-B PTC remained significantly associated with higher mortality in multivariable models, with increased 5- and 10-year hazards of death when compared to patients who received no RT (5-year HRPTC Stage IV-B = 1.67 [CI 1.08–2.58]; 10-year HRPTC Stage IV-B = 1.74 [CI 1.12–2.70]).
All models were adjusted for age, sex, race/ethnicity, clinical variables (surgical length of stay and treatment with neck dissection), and socioeconomic factors (insurance status, primary payer, median income quartile of patient zip code, and percent of residents without a high school education in patient zip code).
p < 0.1; ** p < 0.05; *** p < 0.001.
Reductions in death hazards in patients treated with RAI versus no RT previously observed in univariate analysis remained statistically significant in multivariable models. Patients with stage IV-A, IV-B, and IV-C disease in both FTC and PTC groups had significant reductions in death hazards. In multivariable analysis, the largest reduction was observed in the 10-year survival of RAI patients with stage IV-B FTC (HRFTC Stage IV-B = 0.17 [CI 0.05–0.55]). Unlike univariate models, the most modest reduction to hazard of death was observed in the 10-year survival of patients for stage IV-C FTC (HRFTC Stage IV-C = 0.66 [CI 0.54–0.82]).
Time ratios (acceleration of death)
Acceleration of failure models were used to translate findings obtained from proportional hazard models into TR. Therefore, HR >1 corresponds to TR <1 and, conversely, HR <1 corresponds to TR >1. Similarly, TR <1 indicates acceleration of death and shortening of life, whereas TR >1 signifies postponement of death and prolongation of life. These values are listed in Table 4. These overlapping results are presented because TR measures can be easily interpreted and are helpful for patient–physician communication of complex results.
p < 0.1; ** p < 0.05; *** p < 0.001.
TR, time ratio.
For example, recall that an increased hazard of death was observed for stage IV-B PTC patients treated with EBRT when compared to patients who did not receive any modality of RT (unadjusted 5-year HRPTC Stage IV-B = 2.23 [CI 1.42–3.51]). The respective TR for this group of patients is 0.32 (0.16–0.62), indicating from the time of diagnosis, mortality was accelerated, that is, life was shortened, by a factor of 3 compared to stage IV-B PTC patients who did not receive RT.
Similarly, reductions in mortality were translated into TR that show the extent to which life was prolonged. Patients with stage IV-C FTC treated with RAI exhibited a TR of 1.98 (1.31–3.00), indicating that these patients lived twice as long following diagnosis as their counterparts who did not receive RT.
Significant control variables
Multivariable analysis yielded several significant covariates (Supplementary Tables S2 and S3). Age was found to be significantly related to higher death hazards in all comparisons, except for two groups: stage IV-B and IV-C FTC. Overall, each additional year of age increased the hazard of death by 2–5% up to a maximum 9% per year. Female patients had a lower hazard of death compared to males, specifically in PTC (5-year HRPTC Stage IV-A = 0.70 [CI 0.63–0.78]; HRPTC Stage IV-C = 0.67 [CI 0.50–0.90]). Compared to white patients, African Americans had improved five-year survival for stage IV-C FTC (HRFTC Stage IV-C = 0.77 [CI 0.61–0.97]), but this difference was not statistically significant at 10 years (HRFTC Stage IV-C = 0.81 [CI 0.62–1.06]). However, African Americans with PTC had lower survival rates compared to white patients both at 5 years (HRPTC Stage IV-C = 1.20 [CI 1.02–1.40]) and 10 years (HRPTC Stage IV-C = 1.18 [1.03–1.36]). Tumor grade showed a dose response in most models, where death hazards worsened in the following order: well differentiated tumors < moderately differentiated tumors < poorly differentiated tumors < undifferentiated. Of note, >50% of NCDB data entries lacked tumor grade information.
Discussion
Adjuvant RT
To the authors' knowledge, this is largest study that examines long-term survival in patients with stage IV DTC treated with EBRT or RAI in the postsurgical setting. The study cohort of 11,832 patients had demographics similar to previous studies, thus supporting the external validity of the data (3,7). Female sex and younger age were found to be associated with a survival benefit. These trends corroborate by previous findings (8,9).
It is well established that oncologic outcomes in DTC are worse with extrathyroidal extension or with cervical or distant metastasis (10). Adjuvant treatments in stage IV DTC are therefore particularly valuable in this disease process that otherwise has excellent outcomes in earlier stages. In this study, PTC patients had better survival than FTC patients had. This supports previously published results, and may potentially be due to a higher proportion of patients with distant metastasis (stage IV-C), as seen with the present data. The highest survival rates were seen in patients with stage IV-A PTC. This is not surprising, given that it represents the subset of patients in the cohort with the earliest stage of disease and more favorable histology (3).
The treatment benefits of RAI in DTC have been studied immensely (3,7,8,11,12), and the large cohort of advanced-stage disease further demonstrates improved overall survival in stage IV DTC at 5 and 10 years. Crude overall survival was greatest in patients with PTC treated with RAI, approaching an excellent survival rate of 90% at five years, despite having stage IV disease. All treatment groups showed an association between adjuvant RAI and improved survival, with decreases in death hazards in both univariate and multivariable analyses. As measured by TR, patients with stage IV DTC prolonged their survival following diagnosis by a factor of 1.53–4.66 in multivariable models and 1.63–4.92 in univariate models. This indicates that RAI is an effective and valuable adjuvant treatment for DTC following surgical resection.
The most impressive survival benefit was observed in stage IV-B patients (TRFTC Stage IV-B = 4.41 [1.79–10.87]; TRPTC Stage IV-B = 4.92 [2.42–10.00]). Stage IV-B is defined by T4b disease, indicating direct invasion of the tumor through the pre-vertebral fascia or encasing the carotid artery or mediastinal vessels. T4b staging also implies that the entirety of the tumor is unlikely to be resected by surgery alone, with a high likelihood of remnant local disease following surgery. The remaining disease would therefore need to be addressed in adjuvant treatment, which may be the basis for the particularly large benefit of RAI in stage IV-B patients.
Multiple prior studies have demonstrated a survival benefit with EBRT in DTC patients (3,11,13 –16). Brierley et al. found that adjuvant EBRT in patients >60 years of age with extrathyroidal extension but no gross residual disease following surgery was associated with improved cause-specific survival (81% vs. 64.6%) and disease-free survival (86.4% vs. 65.7%) at 10 years (3). Chow et al. identified a similar benefit in PTC patients with gross residual disease, with EBRT improving 10-year cause-specific survival from 49.7% to 74.1% (11). In their meta-analysis, Fussey et al. found that patients who received adjuvant EBRT had decreased locoregional recurrence: 8% compared to 25% (13).
Interestingly, the data in this study paradoxically show that survival outcomes in patients with stage IV DTC, specifically PTC, treated with EBRT were worse than patients who did not receive any adjuvant RT. The effects of confounding variables may influence these results. Age was found to be a statistically significant covariate in multivariable models, with death hazards increasing by 2–5% per year of life. As previously noted, PTC patients treated with EBRT were significantly older than patients who did not receive treatment with adjuvant RT, which may partially account for the observed mortality differences.
A greater proportion of EBRT patients were also at a more advanced stage. Nearly two-thirds of FTC patients who received EBRT had stage IV-C disease compared to just 47.6% in the no RT group and 53.5% in the RAI group. A similar trend was observed in PTC patients, with stage IV-B and IV-C respectively representing 17.4% and 31.5% of EBRT patients versus 6.5% and 12.0% of patients treated with no adjuvant RT and 3.6% and 9.7% of patients treated with RAI.
Older age and more advanced stage in the cohort of EBRT patients were likely confounders in the observed results of increased death hazards and mortality. Indeed, statistical significance for increased hazard of death was lost in the stage IV-A PTC group treated with EBRT in multivariable analysis after adjustment for covariates including age and stage. However, all EBRT groups in patients with PTC trended toward an increased hazard of death at 5- and 10-year survival in multivariable models, and the increased HR associated with EBRT in stage IV-B PTC group remained statistically significant in multivariable analysis. This indicates that the observed association between EBRT and increased hazards of death and mortality in PTC cannot entirely be accounted for by covariates alone.
Crude all-cause mortality at 5 and 10 years of both PTC and FTC groups was significantly increased in patients who received EBRT and decreased in patients treated with RAI. Similar to PTC patients, FTC patients with stage IV disease treated with adjuvant EBRT trended toward increased death hazards on univariate analysis. This was observed in stages IV-A, IV-B, and IV-C, with all groups having increased hazard of death at both 5 and 10 years after diagnosis, though none of these values reached statistical significance. Interestingly, most of these HR reversed on multivariable analysis. In multivariable models, FTC patients with stage IV-A, IV-B, and IV-C disease had reduced death hazards at five years, and patients with stage IV-B and IV-C disease had reduced death hazards at 10 years. Although none of these values reached statistical significance, these trends suggest differences in sensitivity to EBRT between FTC and PTC, and may be of interest in future research.
Indications for EBRT per AHNS practice guidelines include clinical considerations known to have importance prognostic implications. Patients with gross residual disease following surgical resection and patients with microscopic or macroscopic disease that has low avidity for RAI are limited to EBRT as the only treatment option, and these patients have previously been shown to have greater mortality and poorer survival outcomes (4). Therefore, to conclude that treatment with EBRT increases mortality in patients with DTC would be a misinterpretation of the data. A more appropriate conclusion would be that indications to treat with EBRT inherently confer a poorer prognosis in patients with advanced-stage DTC, particularly PTC. For example, tumors that have low iodine uptake or increased FDG avidity on positron emission tomography imaging are prognostically unfavorable but have minimal treatment benefit from adjuvant RAI and may therefore be treated with EBRT (17,18). Therefore, despite the survival benefit with EBRT that has been demonstrated in previous studies in certain DTC patients, overall survival outcomes are poorer in patients with stage IV DTC in whom EBRT is indicated than they are in patients who do not receive adjuvant RT.
Race/ethnicity and socioeconomic status
Prior studies have shown differences in DTC outcomes based on race/ethnicity. Harari et al. found that nonwhite ethnic minorities, patients of lower socioeconomic status (SES), and patients with Medicaid or no insurance were more likely to present with lymph node metastasis from DTC, and that black patients had poorer overall survival (19). While SES and insurance were not associated with sub-stage or survival in this study, African American patients with PTC were found to have higher mortality (5-year HRPTC Stage IV-C = 1.20 [CI 1.02–1.40]); 10-year HRPTC Stage IV-C = 1.18 [CI 1.03–1.36]). Previous data from Wenaas et al. indicated that black patients with advanced-stage PTC are less likely to receive treatment in compliance with ATA guidelines (20), which may account for the worse survival outcomes with advanced PTC in African Americans observed in this study. Interestingly, African American patients in the study cohort had improved survival with stage IV-C FTC when compared to white patients, suggesting that racial disparities in survival may be different with PTC and FTC.
Limitations
Like all retrospective cohort studies, patients were not controlled or randomized into treatment groups and are therefore subject to potential sources of bias. Biermann et al. attempted a prospective, randomized trial to examine the effect of adjuvant EBRT in pathologic T4 DTC, but were unable to recruit a sufficient number of patients (21). In the present study, possible skewing effects of confounding variables were observed with age, sub-stage, and other variables, although attempts to adjust for the effects of covariates were performed with multivariable analysis.
Additional limitations relate to deficiencies in the data set. Information regarding disease-specific survival and recurrence are not available through the NCDB, likely owing to the difficulty of obtaining certain data through the sampling methods inherent to the NCDB. Analysis was limited by missing data entries, most notably with tumor histologic grade. More than 50% of patients had missing grade data across both DTC types and all RT treatment groups. The authors therefore advise caution when interpreting the significance of tumor grade data in this study.
Conclusions
Through the NCDB, this study sought to describe prognosis and survival outcomes for stage IV DTC based on AJCC sub-stage and the postsurgical treatment that the patient received. In this large retrospective cohort, RAI was associated with improved 5- and 10-year survival for stages IV-A, IV-B, and IV-C PTC and FTC. In contrast, EBRT was associated with poorer survival outcomes, particularly with PTC. While indications for treatment with RAI and EBRT may explain survival differences, the data suggest that treatment with RAI inherently confers better prognosis and survival, and treatment with EBRT confers poorer prognosis and survival. This study is limited by lack of randomization and missing data within the NCDB, particularly regarding tumor grade and recurrence data.
Footnotes
Acknowledgments
This abstract was presented at the American Head and Neck Society 9th International Conference on Head and Neck Cancer in Seattle, WA, July 16–20, 2016.
Author Disclosure Statement
No competing financial interests exist.