
Abstract
Background:
Autoimmune thyroid disease (AITD) is highly prevalent. Although AITD is less common in males, it is unclear whether estradiol (E2) combined with total testosterone (T) contributes to the prevalence of AITD. This study evaluated the association between the E2/T ratio and the prevalence of AITD in males.
Methods:
The data were obtained from a cross-sectional population-based study, the SPECT-China study, 2014–2015. A total of 4109 males ≥18 years of age were enrolled in this study. Participants underwent several checkups, which included assays of serum E2, T, thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) levels, as well as thyroid ultrasonography (US). AITD was defined based on the presence of TPOAb and TgAb levels, and the presence of thyroid US findings.
Results:
Overall, the prevalence of positivity for TPOAb and/or TgAb (TPO/TgAb[+]) was 11.02%, and the positivity for TPOAb and/or TgAb together with US (TPO/TgAb[+] and US[+]) was 4.58%. The E2/T ratio levels were significantly higher in the TPO/TgAb(+) group and the TPO/TgAb(+) and US(+) group (7.91 ± 8.03 vs. 7.19 ± 10.30, p = 0.003; 8.78 ± 11.26 vs. 7.19 ± 10.30, p = 0.001) compared to the TPO and TgAb(–) group. The prevalence of TPO/TgAb(+) and US(+) significantly increased with an increasing E2/T ratio (p = 0.013). Binary logistic analysis showed that increased E2/T ratio levels were associated with an increased risk of AITD (TPO/TgAb[+]: odds ratio = 1.35, p = 0.002; TPO/TgAb[+] and US[+]: odds ratio = 1.48, p = 0.006).
Conclusions:
AITD is highly prevalent in males in China. Higher E2/T ratios were significantly associated with AITD among males. Further studies will be needed to assess whether there is a causal relationship between E2/T ratios and AITD.
Introduction
A
The ratio of estradiol to total testosterone (E2/T) is now widely used to explore the relationship between sex hormones, and possible synergistic effects of estrogen and androgen action, and clinical diseases, including autoimmune disease (4,9,10). It is unclear whether differences in estrogen and androgen levels contribute to the prevalence of AITD among males, which has only been studied rarely (11). A population-based observational investigation named Survey on Prevalence in East China for Metabolic Diseases and Risk Factors (SPECT-China) in 2014 and 2015 was performed to examine whether the ratio of E2/T is related to thyroid autoimmunity in males.
Materials and Methods
Study participants
SPECT-China is a population-based cross-sectional survey on the prevalence of metabolic diseases and risk factors in East China with a registration number of ChiCTR-ECS-14005052 (
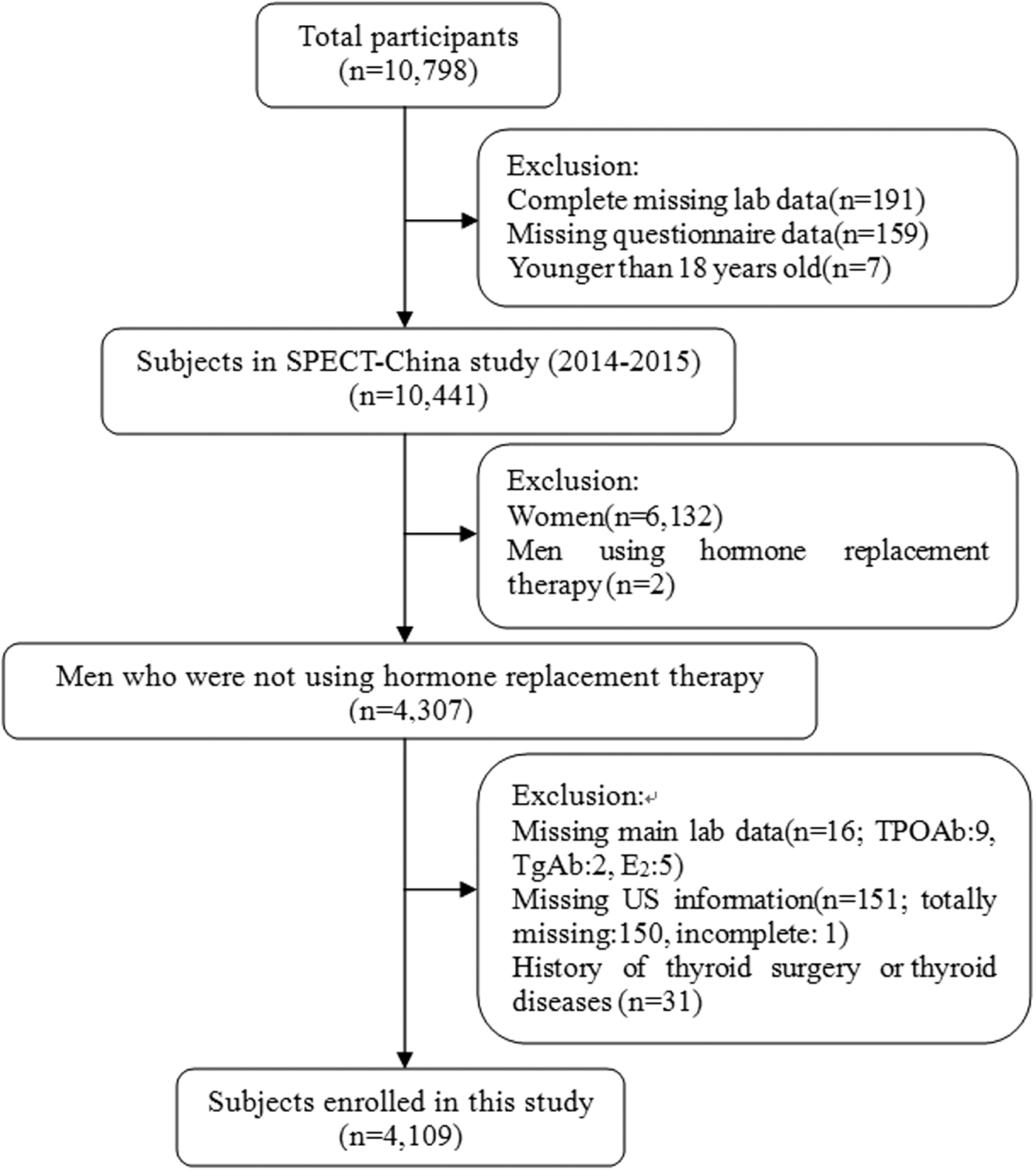
Flow chart of the inclusion and exclusion of participants.
The study initially enrolled 4307 men ≥18 years of age who were not using hormone replacement therapy. Men with missing main lab results including E2, T, thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb; n = 16), missing ultrasound (US) information (n = 151), or who had a history that included thyroid surgery or thyroid diseases (including hyperthyroidism, hypothyroidism, subacute thyroiditis, and radioactive iodine treatment history; n = 31) were excluded. Finally, 4109 subjects were included in the final analysis. The inclusion and exclusion of participants in this analysis is shown in Figure 1.
Data collection
At every step of this study, all data collection was performed by the same staff group from the Department of Endocrinology in Shanghai Ninth People's Hospital, Shanghai Jiaotong University School of Medicine. All staff successfully completed a standard training program that made them familiar with the specific tools and methods used. A standard questionnaire was administered by trained staff to obtain information on demographic characteristics, personal and family medical history, and risk factors in their daily lives. Clinical staff members were trained to measure blood pressure and obtain anthropometric measurements and blood samples.
Laboratorial assays
Serum samples for laboratorial assays were obtained by venipuncture after an eight-hour fast. Blood samples were stored at −20°C when collected and shipped by air in dry ice to one central laboratory, which was certified by the College of American Pathologists, within two to four hours of collection.
Serum TPOAb, TgAb, thyroxine (T4), triiodothyronine (T3), and thyrotropin (TSH) were measured by chemiluminescence immunoassays (Immulite 2000; Siemens, Munich, Germany). T and E2 were measured by chemiluminescence (Immulite 2000; Siemens). Sex hormone binding globulin (SHBG) was measured by a chemiluminescence immunoassay (E601; Roche, Basel, Switzerland). The minimal detectable limits for each sex hormone were as follows: 0.7 nmol/L (T), 73.4 pmol/L (E2), and 0.35 nmol/L (SHBG). The inter-assay coefficients of variation were as follows: 6.6% (T), 7.5% (E2), and 7% (SHBG). The intra-assay coefficients of variation were as follows: 5.7% (T), 6.2% (E2), and 7% (SHBG).
Thyroid US
Thyroid US examination was performed by the two same registered physicians, who both had a professional certificate for US awarded by the Ministry of Health of China, using B-mode US imaging (M7; Mindray Shenzhen, P.R. China) with a 10 MHz linear array probe. The scanning protocol in all cases included both transverse and longitudinal real-time imaging of the thyroid.
Definition of AITD
AITD was defined in two different ways: the serum TPOAb and/or TgAb positive (>60 IU/mL; TPO/TgAb[+]) group, and TPOAb and/or TgAb positivity together with characteristic US features (diffuse parenchymal hypoechogenicity and/or heterogeneous echogenic pattern of the thyroid gland; TPO/TgAb[+] and US[+]) group (12,13).
Statistical analysis
Continuous variables are expressed as the mean (±standard deviation) values, and categorical variables are presented as numbers (percentage). Continuous variables were compared using Student's t-test. The Mann–Whitney U-test was used for non-normally distributed continuous variables, and Pearson's chi-square test was used for dichotomous variables. To test for differences in characteristics between the TPO and TgAb(–) group and the TPO/TgAb(+) group or the TPO/TgAb(+) and US(+) group for E2/T ratio quartiles, the Kruskal–Wallis test and a one-way analysis of variance were used for non-normally and normally distributed continuous data, respectively. The odds ratio (OR) and confidence intervals (CIs) were calculated using a logistic regression to determine the risk of AITD based on the E2/T ratio. Survey analyses were performed with IBM SPSS Statistics for Windows v22 (IBM Corp., Armonk, NY). All analyses were two-sided. A p-value of <0.05 was taken to indicate a significant difference.
Body mass index (BMI) was calculated as the weight in kilograms divided by height in meters squared. Insulin resistance was estimated by the homeostatic model assessment (HOMA-IR) index: (fasting insulin [mIU/L]) × (FPG [mmol/L])/22.5.
Results
Clinical characteristics according to TPOAb, TgAb levels, and US findings
A total of 4109 subjects were enrolled in this study. The mean age was 54.1 ± 13.2 years, and the mean BMI was 24.9 ± 3.3 kg/m2. The overall prevalence of TPOAb positivity was 8.40% (n = 345), and that of TgAb positivity was 5.84% (n = 240). The prevalence rates of TPO/TgAb(+) and TPO/TgAb(+) and US(+) were 11.02% (n = 453) and 4.58% (n = 188), respectively. The characteristics of the study subjects in terms of TPO/TgAb positivity and US are summarized in Table 1. Participants with AITD had higher BMIs; higher neck, waist and hip circumferences; higher levels of Cr, TSH, and E2; higher E2/T ratios; and lower levels of T4 and T compared to participants in the TPO and TgAb(–) group.
p-Value vs. TPO and TgAb(–).
Data are presented as the mean ± standard deviation for continuous variables or as a number with proportion for categorical variables. Age, LDL, waist-to-hip ratio, waist circumference, and hip circumference are normally distributed.
Smokers: current and past smoking history. The smoking history is missing in 156 participants: 136 in the TPO and TgAb(–) group, 20 in the TPO/TgAb(+) group, and 8 in the TPO/TgAb(+) and US(+) group.
BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance; HbA1c, glycated hemoglobin; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ALT, alanine aminotransferase; T3, triiodothyronine; T4, thyroxine; T, testosterone; E2, estradiol; SHBG, sex hormone-binding globulin.
E2/T ratio levels according to AITD
The mean E2/T ratio levels (log-transformed for normal distribution) were compared between the TPO/TgAb(+) and TPO and TgAb(–) groups. The E2/T ratio was significantly higher in the TPO/TgAb(+) group compared to the TPO and TgAb(–) group (1.86 ± 0.63 vs. 1.77 ± 0.60; p = 0.004). When the TPO/TgAb(+) and US(+) group was compared with the TPO and TgAb(–) group, this trend became more significant (1.94 ± 0.62 vs. 1.77 ± 0.60; p < 0.001).
Prevalence of AITD according to E2/T ratio levels
To analyze the relationship between the E2/T ratio and AITD more effectively, the association between serum E2/T ratios and the prevalence of AITD was analyzed. Study subjects were classified into four groups based on their E2/T ratio quartiles (Q1: ≤4.05; Q2: 4.05–6.23; Q3: 6.23–8.84; Q4: ≥8.84). The general study subject characteristics in terms of the level of E2/T ratio quartiles are shown in Table 2. It was observed that the prevalence of AITD increased along with an increasing E2/T ratio. Statistical significance was only seen in the TPO/TgAb(+) and US(+) group (3.51%, 3.60%, 5.16%, and 6.03%; p = 0.013), while a marginal association was present in the TPO/TgAb(+) group (9.83%, 9.83%, 11.38%, and 13.05%; p = 0.061; Table 2 and Fig. 2).
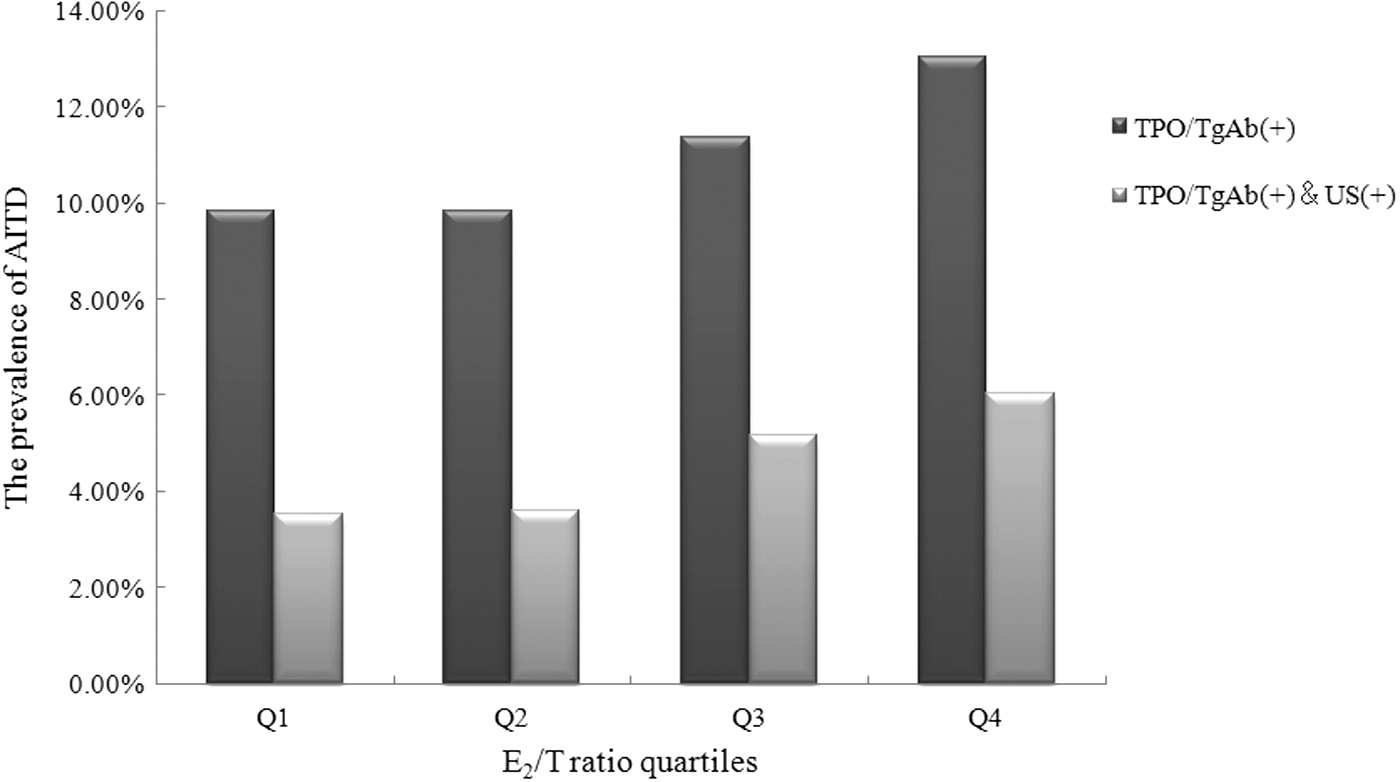
The prevalence of thyroid peroxidase (TPO)/thyroglobulin antibody TgAb(+) and TPO/TgAb(+) and ultrasound (+) according to estradiol (E2)/testosterone (T) ratio quartiles (Q) in men. The p-values were 0.061 and 0.013, respectively. E2/T ratios were divided into Q1 ≤4.05, Q2 4.05–6.23, Q3 6.23–8.84, and Q4 ≥8.84.
Data are presented as the mean ± standard deviation for continuous variables or as a number with proportion for categorical variables. Age, BMI, waist circumference, hip circumference, LDL, and T4 are normally distributed.
Smokers: current and past smoking history. The smoking history is missing in 156 participants (35, 35, 43, and 43 in Q1–Q4, respectively).
Relationship between E2/T ratio levels and AITD
The adjusted ORs were evaluated in the TPO/TgAb(+) and TPO/TgAb(+) and US(+) groups. The adjusted ORs were calculated after adjusting for age, BMI, smoking history (including current and past), HOMA-IR, triglycerides (TG), low-density lipoprotein, high-density lipoprotein, TSH, T4, and SHBG. The TSH, TG, HOMA-IR, SHBG, and E2/T ratios were log-transformed before regression analysis in order to achieve a normal distribution. Binary logistic analysis showed that increased E2/T ratios were associated with an increased risk of TPO/TgAb(+) and TPO/TgAb(+) and US(+). The ORs were 1.35 ([CI 1.12–1.62]; p = 0.002) and 1.48 ([CI 1.12–1.95]; p = 0.006), respectively (Table 3).
TSH, TG, HOMA-IR, SHBG, and E2/T ratio levels were log-transformed before regression analysis.
AITD, autoimmune thyroid disease; OR, odds ratio; CI, confidence interval.
Discussion
AITDs, including Graves' disease and Hashimoto's thyroiditis, comprise the most common autoimmune disease in humans. In principle, AITD is a histological diagnosis. However, the diagnosis can be made by clinical evaluation, antibody measurement, and US findings. Cogni et al. reported that the basic mechanisms in the development of thyroid autoimmunity may be due to a combined TPO- and Tg-specific cytotoxic immune response (14). High levels of either TPOAb or TgAb serve as a clinical marker for the detection of AITD (5,14,15). It has been reported that the prevalence of detectable thyroid antibodies, primarily TPOAb, comprises 10–12% of the healthy population (12,16,17) and approximately 7.0% of all adult men (18). Additionally, 2.3% of Korean males were found to have both TPOAb positivity and US positivity (12). The prevalence of TPOAb and/or TgAb positivity together with US positivity in this study was 4.58% among males in East China.
Cutolo et al. (4) indicated that E2 and T appear to interfere oppositely with the expression and production of pro-inflammatory cytokines by activated macrophages and modulate the downregulation of immune and inflammatory reactions. Estrogen and T play different roles in both inflammatory and anti-inflammatory effects on the immune response through several pathways (19 –22). A recent study showed that higher E2 levels were associated with thyroid autoimmunity in 1263 males by the presence of positive TRAb, but not by TPOAb or TgAb, which suggested that E2 may play a role in the pathogenesis of Graves' disease in men (11). The present cross-sectional study enrolled 4109 males, which was far more than the previous study, and the role of T in autoimmunity was also taken into account. The present study demonstrates that E2/T ratios are significantly increased in men with AITD. The adjusted odds ratio of AITD increased by 35% and 48% for higher E2/T ratios in the TPO/TgAb(+) and TPO/TgAb(+) and US(+) groups, respectively, which further confirms a close relationship between higher E2/T ratios and AITD.
Chailurkit et al. (11) suggested an extrathyroidal origin of thyroid autoimmunity. The nature of the factors external to the thyroid gland is uncertain. The present findings suggest that the combined effect of estrogen and T may be such a factor. It must be noted that the findings apply only to males. For females, the severity of AITD does not decrease with menopause, and the prevalence of thyroid autoimmunity does not differ by menopausal status (23). Second, pregnancy is a triggering factor for thyroid disruption and autoimmunity (24). This may be due to pregnancy-induced immune tolerance (25).
However, this study also has several limitations. First, the finding of an association between E2/T ratios and AITD suggests that the E2/T ratio may play a role in the pathogenesis of AITD in men. However, association does not indicate causation, and a reverse effect of AITD leading to changes in E2 and T still needs to be excluded. Second, sex hormones were only measured on a single occasion in order to characterize each subject's hormonal status. However, this is not expected to affect the results because single measurements on morning samples should provide representative and reliable data in large epidemiological studies (26). Third, all the participants enrolled in this study were from East China, and most subjects recruited were Han Chinese. The findings may not therefore be generalizable to other areas in China or other ethnicities.
In summary, AITD is highly prevalent among males in China. The present analysis found that higher E2/T ratios were significantly associated with AITD among males. Further studies should determine the possibility of a causal relationship and investigate the underlying mechanisms of this finding.
Footnotes
Acknowledgments
The authors thank all team members and participants from Institute and Department of Endocrinology and Metabolism, Shanghai Ninth People's Hospital, Shanghai Jiaotong University School of Medicine (Shanghai, China), Shangyu People's Hospital (Zhejiang, China), Fengcheng Hospital (Shanghai, China), the Third Affiliated Hospital of Nanchang University (Jiangxi, China), Nanjing Drum Tower Hospital The Affiliated Hospital of Nanjing University Medical School (Jiangsu, China), the First Affiliated Hospital of Anhui Medical University (Anhui, China) in the SPECT-China study 2014–2015.
The SPECT-China study was supported by National Natural Science Foundation of China (81570726, 81270885, 81070677); fund for Clinical Potential Subject Construction of Shanghai JiaoTong University School of Medicine (2014); Ministry of Science and Technology in China (2012CB524906); Science and Technology Commission of Shanghai Municipality (14495810700); The Fourth Round of Three-year Public Health Action Plan of Shanghai (no. 15GWZK0202); and Foundation of Shanghai Jiao Tong University School of Medicine (no.14XG10026, 2014–2016).
The funders played no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; or preparation, review, and approval of the manuscript.
Clinical Trial Registration Number: ChiCTR-ECS-14005052 (
Author Disclosure Statement
The authors have nothing to disclose.